(UroToday.com) The 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026, was host to the Poster Session A: Prostate Cancer. Dr. Edwin M. Posadas presented Poster 156: A randomized phase 2 study of enhanced AR blockade with enzalutamide in high-risk patients with biochemical relapse undergoing salvage radiation: Final results from RTOG 3506 (STEEL).
Dr. Posadas began by noting that patients with adverse pathologic features who develop BCR after RP benefit from the addition of androgen deprivation therapy (ADT) to salvage radiotherapy (SRT). However, outcomes remain suboptimal in patients with multiple aggressive features. Based on this, the investigators hypothesized that enhanced androgen receptor blockade (eARB) with enzalutamide could further improve outcomes in this high-risk setting.
This randomized phase II trial enrolled post-RP patients with BCR (PSA ≥ 0.2 ng/mL) and at least one high-risk feature, including Gleason 8–10 disease, seminal vesicle invasion, pN1 disease, persistent PSA >0.1 ng/mL after RP, or PSA ≥ 0.7 ng/mL at recurrence. Patients were randomized 1:1 to receive 24 months of standard ADT (sADT) with an LHRH analog or intensified therapy consisting of LHRH analog plus enzalutamide 160 mg daily. The trial design is shown below.
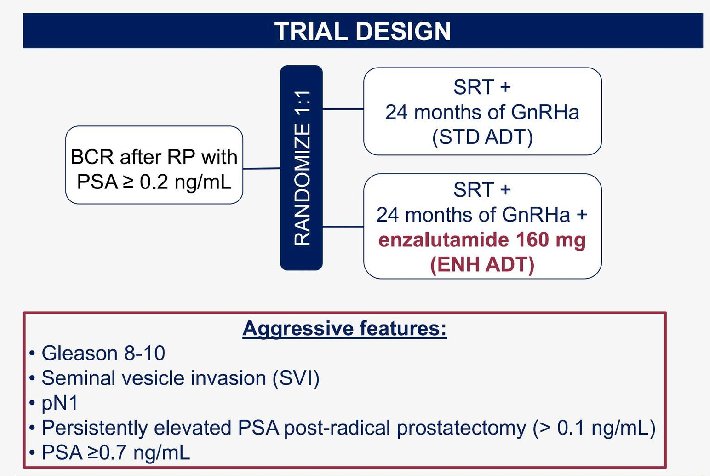
The radiotherapy strategy included both mandatory and optional components. Mandatory treatment volumes comprised the prostatic fossa, delivered to 66.6–70.2 Gy in 1.8 Gy fractions or 66–70 Gy in 2.0 Gy fractions, and the pelvis, delivered to 45–50.4 Gy in 1.8 Gy fractions or 44–50 Gy in 2.0 Gy fractions. Optional irradiation of the para-aortic lymph node region up to T12/L1 was permitted at the same dose as the pelvis. Boosts were also allowed: individual lymph node boosts could be delivered sequentially or concurrently to achieve an EQD2 (α/β = 3) up to 70 Gy with 1.8 Gy fractions or 65 Gy with 2.0–2.4 Gy fractions, while a prostatic fossa lesion boost was permitted sequentially only, up to 73.8 Gy in 1.8 Gy fractions or 74 Gy in 2.0 Gy fractions.
The primary endpoint was progression-free survival (PFS), defined as PSA ≥ 0.2 ng/mL after SRT or the initiation of new therapy.
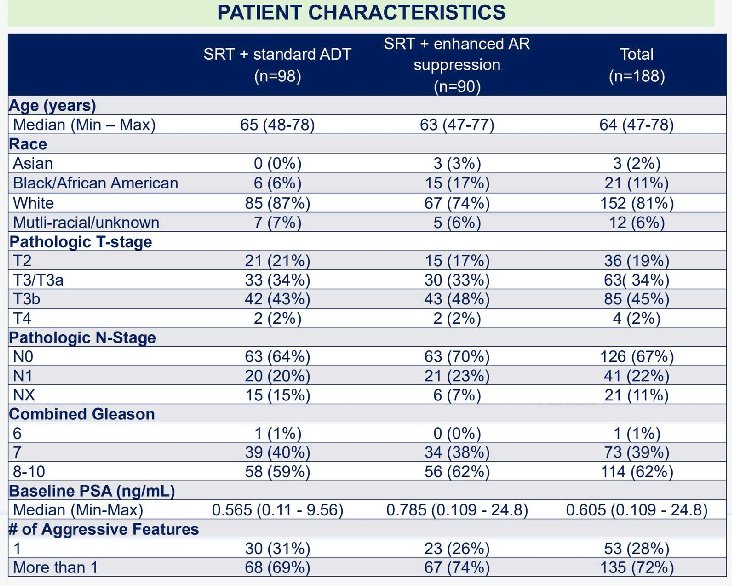
Between April 2019 and August 2022, 188 patients were enrolled, with well-balanced baseline characteristics. The median age was 64 years. High-risk features were common: 22% had pN1 disease, 77% had pT3a–b tumors, and 52% had Gleason 9 disease. Notably, over 70% of patients harbored more than two aggressive features. Median follow-up at the time of analysis was 34.6 months.
The SRT+eARB arm demonstrated improved PFS compared to SRT+sADT (HR 0.62; 80% CI 0.42–0.91; one-sided p=0.052). At two years, the biochemical failure rate was 19% (95% CI 12–28) in the SRT+sADT arm compared to 11% (95% CI 5–18) in the SRT+eARB arm.
Regarding safety, the most frequent grade 3–4 adverse events differed between treatment arms. In the SRT plus enhanced AR suppression arm (N=89), grade 3–4 lymphocyte count decrease occurred in 15% of patients compared with 5% in the SRT plus standard ADT arm (N=98). Hypertension was reported in 8% versus 5%, respectively. Other grade 3–4 events in the enhanced AR suppression arm each occurred in ≤2% of patients and included fatigue (2%), decreased white blood cell count (2%), hot flashes (1%), diarrhea (1%), anemia (1%), insomnia (1%), hyperglycemia (1%), and arthralgia (1%). In the standard ADT arm, grade 3–4 anemia (2%), urinary incontinence (3%), and weight gain (1%) were observed, with most other events occurring in ≤1% of patients.
With respect to treatment discontinuation, completion rates for GnRH analog therapy were similar between arms (89% with enhanced AR suppression vs 87% with standard ADT). Discontinuation due to adverse events occurred in 5% and 7%, respectively. In the enhanced AR suppression arm, 57% of patients completed enzalutamide per protocol, with discontinuations due to adverse events in 19%, withdrawal after starting therapy in 12%, withdrawal due to other complicating disease in 6%, and other reasons in 6%. No new safety signals were identified based on the reported adverse event profile.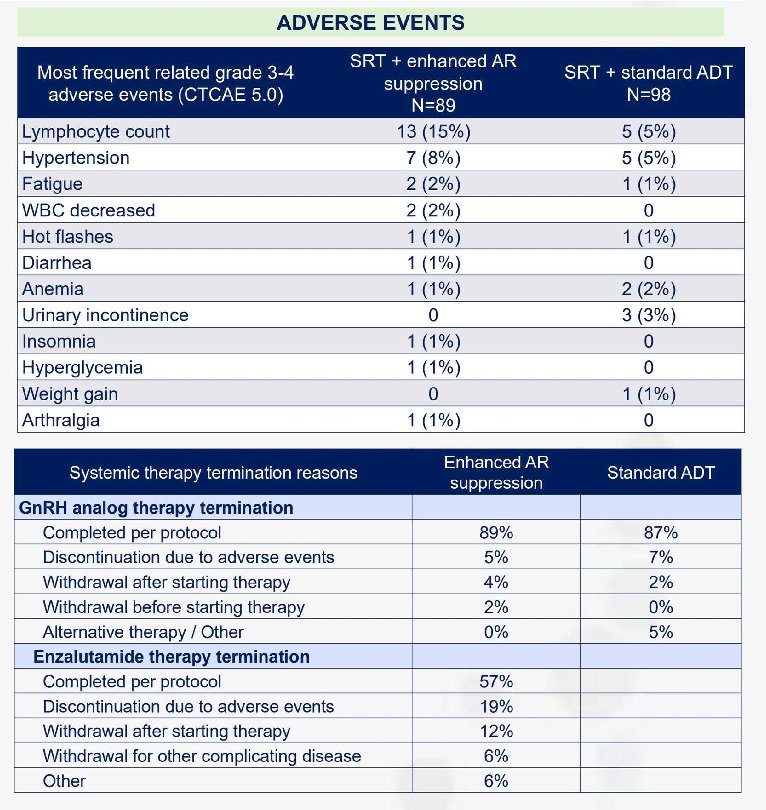
Dr. Posadas concluded his presentation with the following key takeaways:
- Intensification of androgen receptor blockade with enzalutamide added to standard ADT improved progression-free survival in high-risk patients receiving salvage radiotherapy.
- The absolute reduction in 2-year biochemical failure suggests a clinically meaningful benefit in a population with multiple aggressive features.
- Toxicity was increased with enhanced androgen receptor blockade but was consistent with prior enzalutamide studies and did not reveal new safety concerns.
- These findings support further evaluation in a phase III trial to confirm the benefit of intensified systemic therapy in the salvage setting.
Presented by: Edwin Posadas, MD, Samuel Oschin Cancer Center, Cedars-Sinai, Los Angeles, CA
Written by: Julian Chavarriaga, MD – Urologic Oncologist, Department of Urology at Penn State Health. @chavarriagaj on Twitter during the 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026.
Related content: Salvage Radiotherapy Intensification Tested in Men with High-Risk Biochemical Recurrence - Edwin Posadas