(UroToday.com) The 2026 ASCO GU Annual Symposium hosted a prostate cancer poster session. Dr. Takuma Kato presented updated real-world results from the FRONTIER study, evaluating the efficacy and safety of Radium-223 in the context of prior upfront therapy in the metastatic castration-resistant prostate cancer (mCRPC) setting.
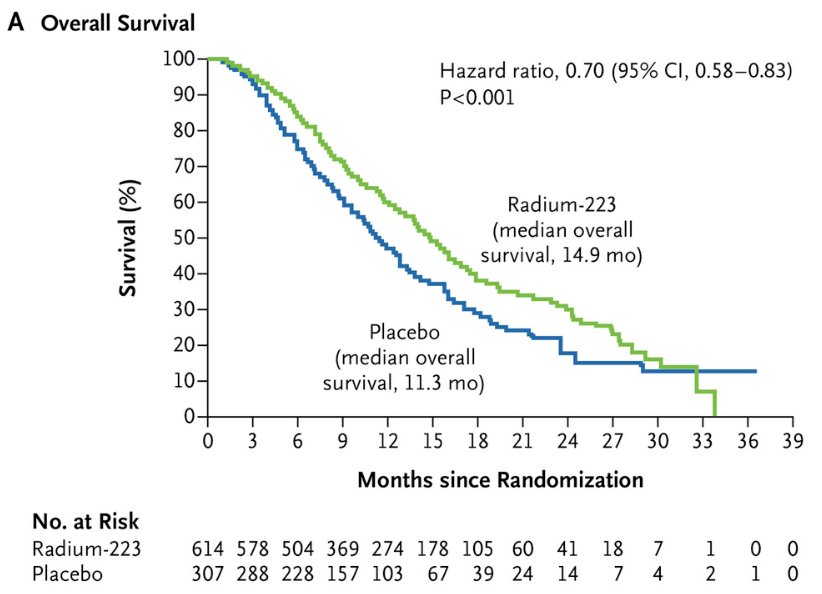
The ALSYMPCA trial was a phase III randomized trial of 921 mCRPC patients randomized 2:1 to receive six intravenous (IV) injections of radium-223 (50 kBq/Kg) or a matching placebo. All patients received the best standard of care, and 57% had received prior docetaxel. Patients receiving radium-223 demonstrated significantly improved median overall survival (14 versus 11.2 months; HR: 0.70, 95% CI: 0.55–0.88). Use of radium-223 was further associated with significantly prolonged time to a first symptomatic skeletal event (15.6 versus 9.8 months, p<0.001) and a significantly higher percentage of radium-223-treated patients achieved clinically meaningful improvements in quality-of-life outcomes (i.e., ≥10-point improvement in the FACT-P total score; 25% versus 16%, p=0.02).1
These results established radium-223 as an effective therapy for mCRPC patients following conventional hormonal therapy (i.e., ADT +/- NSAA). However, outcomes with radium-223 following contemporary upfront treatment intensification during the hormone-sensitive phase remain incompletely characterized. The study investigators, therefore, conducted a retrospective multicenter study in Japan to evaluate real-world outcomes of radium-223 among patients with mCRPC who had previously received upfront therapy intensification during the hormone-sensitive phase.
Patients with mCRPC treated with radium-223 between January 2020 and December 2023 across 84 institutions in Japan were retrospectively identified. Patients were categorized into two groups according to prior treatment during the hormone-sensitive phase: those who had received upfront intensified therapy versus those treated with ‘vintage’ hormonal therapy (i.e., ADT +/- NSAA).
To minimize baseline imbalances between groups, propensity score matching was performed. Continuous variables were compared using the Mann–Whitney U test or Student’s t-test, as appropriate, whereas categorical variables were compared using the chi-square test. Overall survival and cancer-specific survival were estimated using the Kaplan–Meier method and compared using log-rank testing.
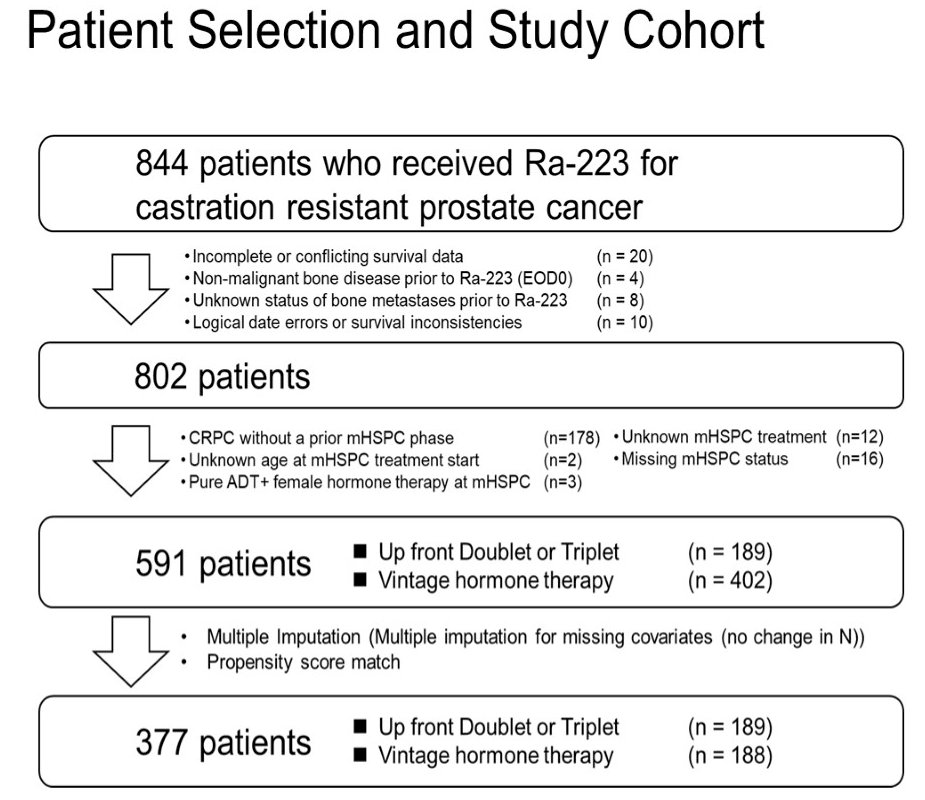
Among 844 patients who received radium-223 for castration-resistant prostate cancer, 802 met the eligibility criteria. Following propensity score matching, 377 patients were included in the analysis, of whom 189 received upfront doublet/triplet therapy, and 188 received ‘vintage’ hormonal therapy.
Radium-223 was administered across multiple lines of therapy, most commonly in the 1st or 2nd line CRPC settings, with significant differences observed between the two treatment groups:
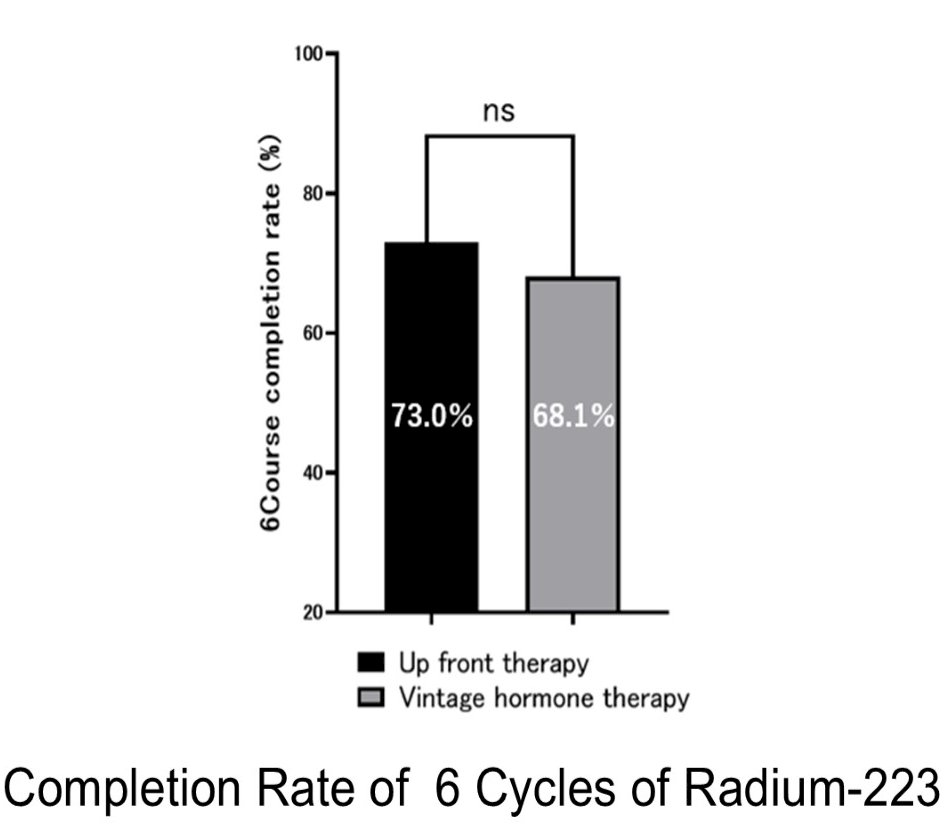
The completion of the planned six-cycle course of radium-223 was similar between groups, with completion rates of 73% among patients who had received upfront intensified therapy compared with 68% among those treated with ‘vintage’ hormonal therapy, indicating comparable treatment feasibility irrespective of prior systemic intensification.
Baseline characteristics were overall well-balanced between the two groups. The median age at radium-223 initiation was similar between groups (72 vs 73 years, p=0.08). Performance status distribution was likewise comparable, with the majority of patients having ECOG 0–1 in both cohorts. Patients in the upfront intensification cohort had lower median PSA levels at radium-223 initiation (6.5 vs 15.7 ng/mL, p=0.001) and modestly lower alkaline phosphatase levels (85 vs 99 IU/L, p=0.046), potentially suggesting slightly lower disease burden at treatment initiation. Other laboratory parameters, including LDH, CRP, albumin, hemoglobin, platelet count, and neutrophil count, were similar between groups.
The extent of bone disease distribution was also comparable, with similar proportions of patients across EOD categories (<6, 6–20, >20 metastases, or superscan). Rates of baseline cancer-related pain were similar, as was the use of bone-modifying agents, which was reported in approximately three-quarters of patients in both cohorts.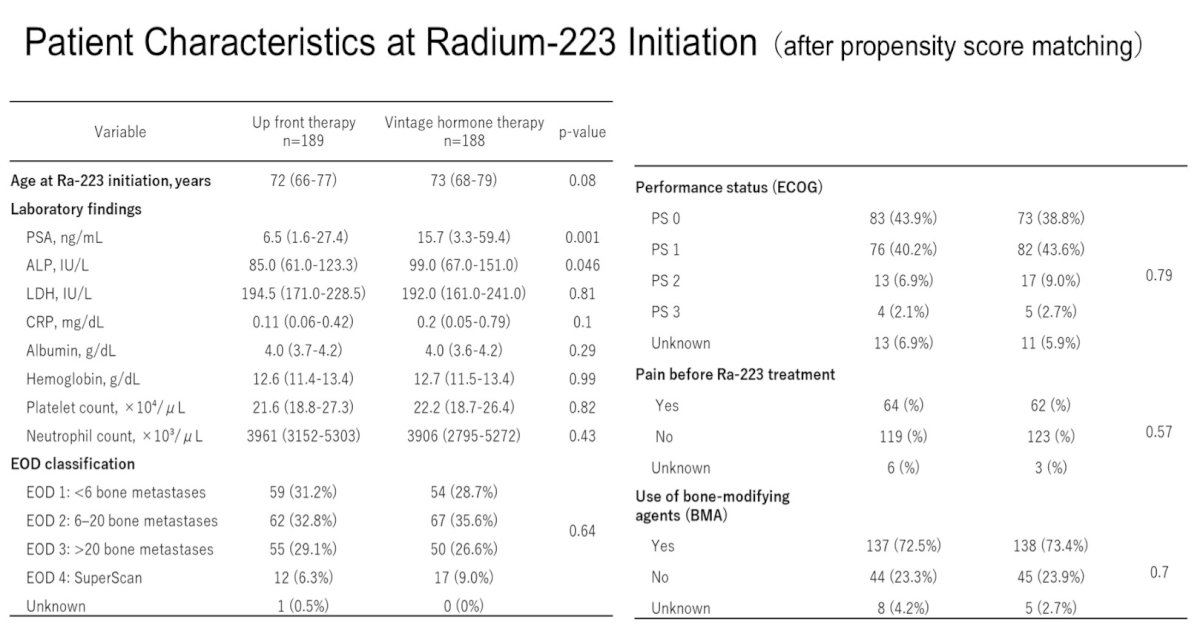
Progression outcomes following radium-223 were comparable between cohorts. At data cut-off, disease progression was reported in 86.8% of patients in the upfront therapy group versus 77.1% in the ‘vintage’ hormonal therapy group, with a median time to progression from radium-223 initiation of approximately 5 months in both cohorts. Reasons for progression were similar, with radiographic progression representing the most common cause (~47–50%), followed by PSA progression (~76–77%), with smaller proportions attributable to clinical symptom progression or other causes.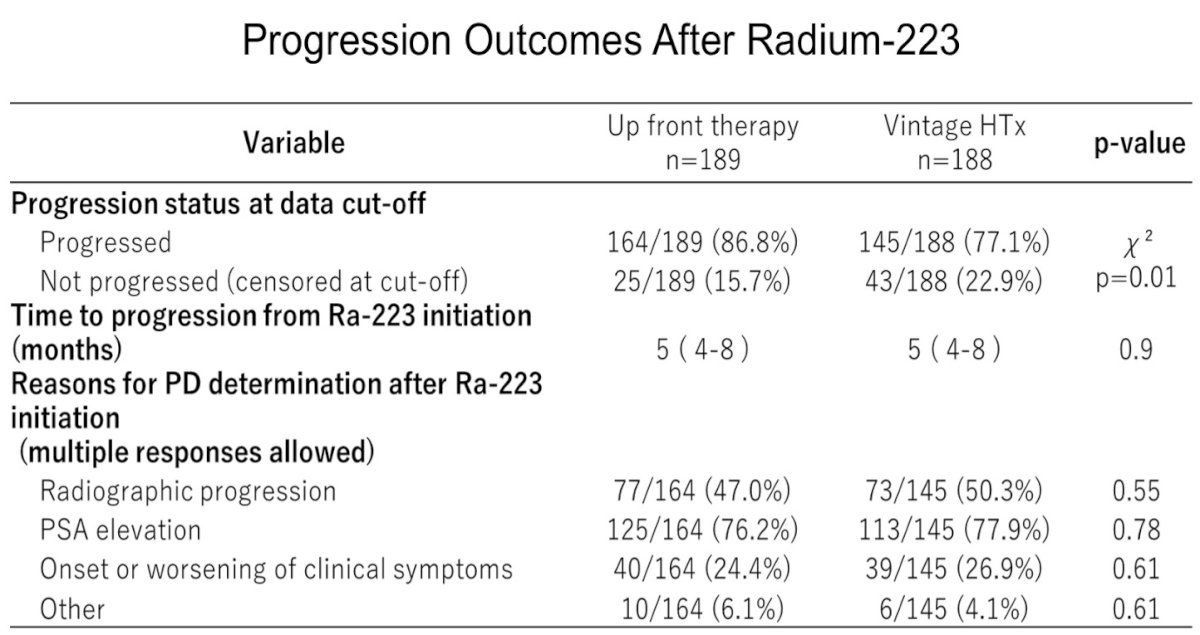
Overall survival analyses among patients completing six cycles of radium-223 demonstrated no significant differences between groups, including when stratified by line of therapy (second line or later). These findings suggest that prior treatment intensification during the hormone-sensitive phase does not appear to compromise subsequent radium-223 efficacy in the castration-resistant setting.

Safety analyses showed broadly comparable hematologic toxicities, including anemia (~4–7%), neutropenia (~5–6%), and thrombocytopenia (~1–2%), as well as low rates of non-hematologic toxicities such as hepatic dysfunction or other organ toxicities. Symptomatic skeletal events occurred in approximately 10–11% of patients overall; however, the incidence was markedly higher among patients who did not receive bone-modifying agents (approximately 36%) compared with those receiving bone-protective therapy (~15%), underscoring the importance of concomitant skeletal protection.
Collectively, these real-world data suggest that prior upfront treatment intensification during the hormone-sensitive phase does not adversely affect disease control, survival outcomes, or treatment completion with subsequent radium-223 therapy in mCRPC. Outcomes appear comparable between patients treated with modern upfront intensification and those previously treated with ‘vintage’ hormonal therapy, while consistent use of bone-modifying agents remains critical to mitigate skeletal complications.
Presented by: Takuma Kato, MD, PhD, Assistant Professor, Department of Urology, Faculty of Medicine, Kagawa University Hospital, Miki, Kagawa, Japan
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the 2026 ASCO GU Annual Symposium, San Francisco, CA, February 26th–28th, 2026
Reference:- Parker C, Nilsson S, Heinrich D, et al. Alpha emitter radium-223 and survival in metastatic prostate cancer. N Engl J Med 2013;369(3):213-223.