(UroToday.com) The 2026 GU ASCO annual meeting featured a testicular cancer session and a discussant presentation by Dr. Samuel A. Funt, discussing the abstract, “Initial results from CLIMATE, a prospective cohort study assessing the clinical utility of miR-371a-3p as a marker of minimal residual disease in clinical stage 1 testicular germ cell tumor: ANZUP 1906” by Dr. Ben Tran.
First-line cisplatin-based chemotherapy cures the majority of metastatic germ cell tumors, but there are substantial side effects associated with cisplatin-based chemotherapy, including (i) hearing loss and tinnitus, (ii) cardiovascular disease, and (iii) secondary malignant neoplasms in testicular cancer survivors. Thus, the goal of testicular germ cell tumor management is to minimize the chemotherapy burden whenever possible.
The definition of clinical stage 1 (CSI) testicular germ cell tumor is as follows:
- A normal CT of the chest, abdomen, and pelvis with contrast: this may need to be repeated at a short (4-6 week) interval if there are questionable findings
- Normal post-orchiectomy tumor markers: these may take time to normalize (check every 1-2 weeks), but there is time to wait if the CT is normal/borderline (the CT may need to be repeated during/after normalization)
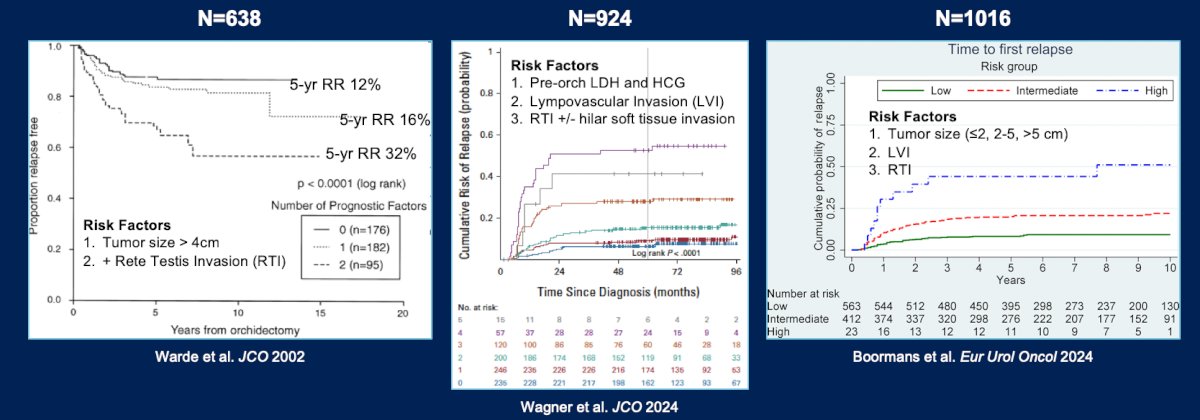
For patients with CSI seminoma, these are risk factors for relapse. Overall, 15% of patients with both rete testis invasion and tumor size > 4 cm approach a 30% 5-year risk of relapse. In the updated series, additional risk factors have been identified in an even smaller group of patients with a higher 5-year risk of relapse:
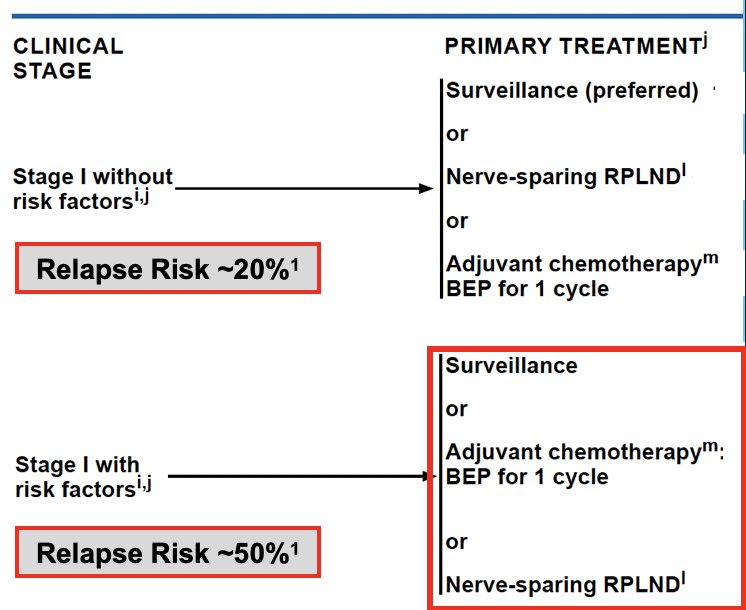
Based on the NCCN 1.2026 guidelines for the management of CSI seminoma, surveillance is strongly preferred for pT1-pT3 tumors, and the NCCN does not recommend risk-adapted treatment for CSI seminoma based on the current variables and with current treatments.
For CSI NSGCTs, the strongest clinical risk factor for recurrence is lymphovascular invasion, with ~50% of patients with lymphovascular invasion relapsing. Based on this risk factor, the NCCN 1.2026 guidelines for the management of CSI NSGCT recommend either surveillance (preferred) or nerve-sparing RPLND, or adjuvant chemotherapy with one cycle of BEP:
Dr. Funt emphasized that there are multiple considerations when counseling patients with CSI testicular germ cell tumors; improved biomarkers are needed to personalize management and avoid over-treatment and under-treatment.
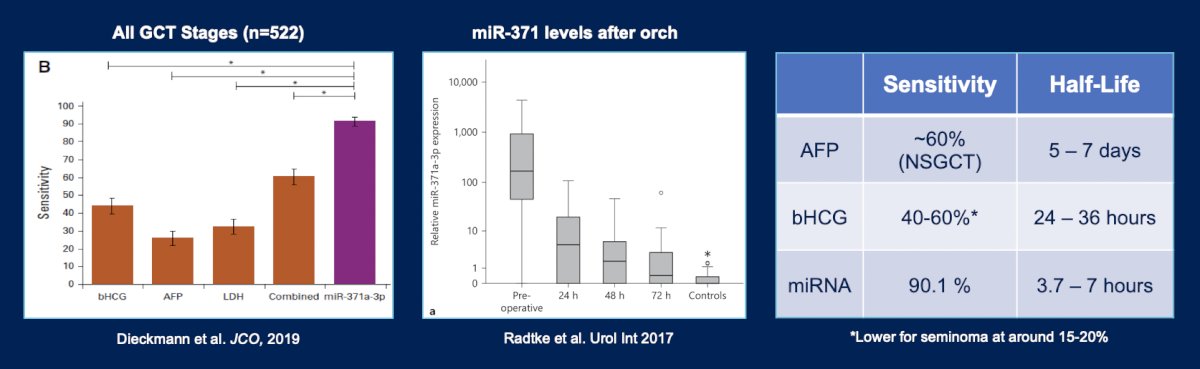
miRNA-371 has improved sensitivity and a shorter half-life than the traditional serum tumor markers:
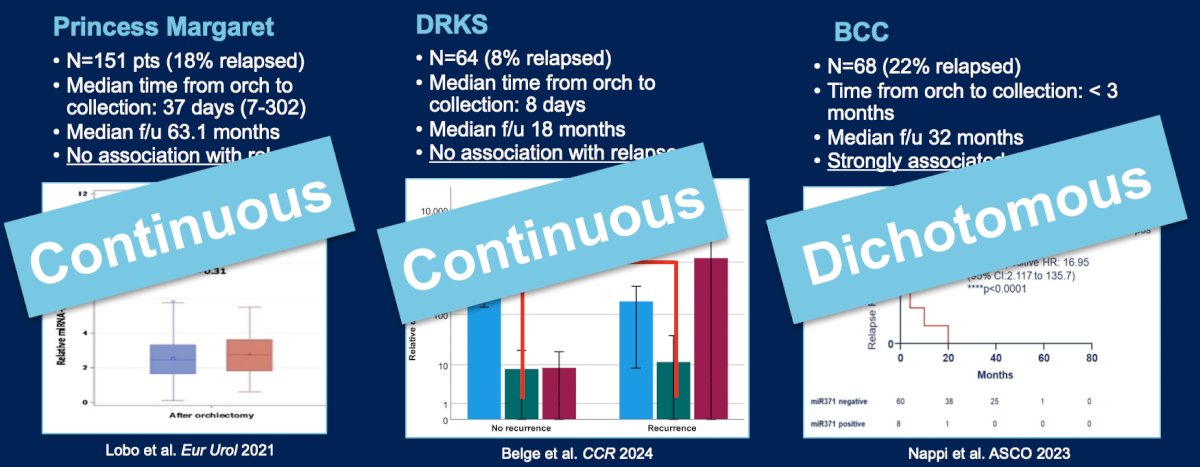
Dr. Funt notes that there is conflicting data on post-orchiectomy miR-371 and relapse risk in the CSI testicular germ cell tumor. The main difference between these studies is the use of miR-371 median levels versus the dichotomous positive versus negative categorization. Additionally, all of these studies were retrospective studies relying on archival samples:
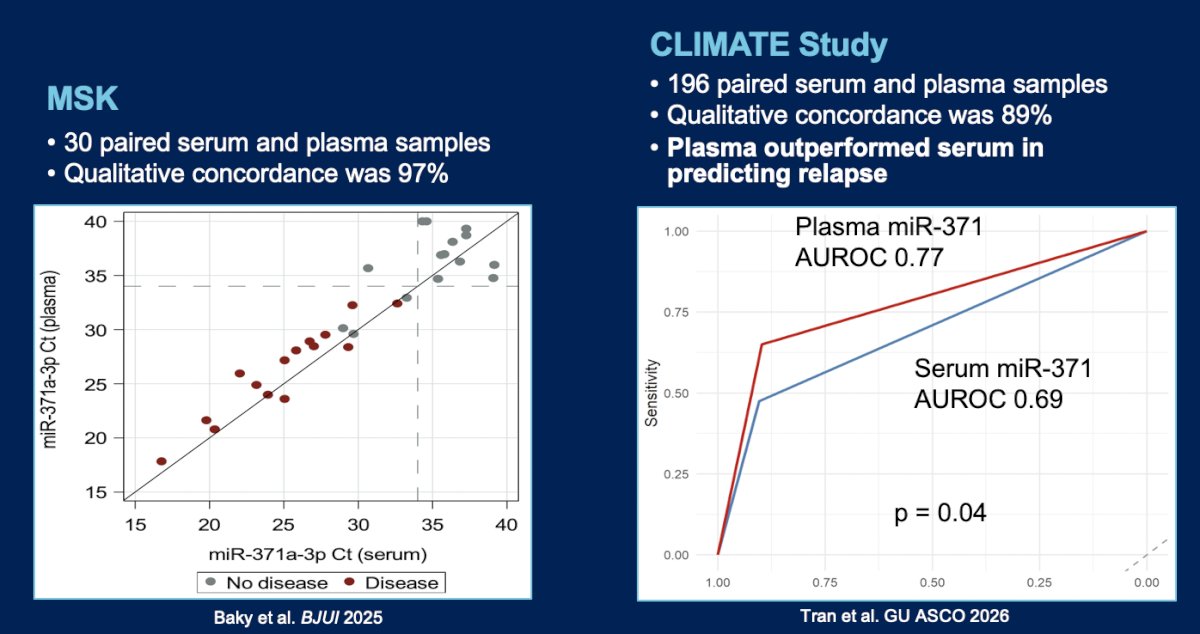
In CLIMATE, patients from 12 sites in Australia and New Zealand, ≥18 years of age, with histologically confirmed CS1 testicular germ cell tumor, no evidence of metastases, and planned for active surveillance, were enrolled ≤6 weeks post-orchiectomy. Plasma and serum were collected at baseline (≤6 weeks post-orchiectomy) and every 3 months for 24 months and at recurrence. The primary objective was to determine the positive predictive value of baseline post-orchiectomy miR-371 in predicting recurrence, and the secondary objective was to compare the performance of serum versus plasma miR-371. CLIMATE enrolled 200 patients from 2021 to 2025, with a median age of 33 years (range: 22-78). There were 196 patients who had assays run on baseline samples prior to data cutoff and were included in this analysis. Orchiectomy histology included 117 (60%) pure seminoma and 79 (40%) non-seminoma. With a median follow-up 18.9 months, there were 40 (20%) recurrences, with a median time to recurrence of 4.2 months (range: 1.1-17.7). Assays using plasma performed better than serum (AUC 0.77 versus 0.69), which was corroborated in a small study from Dr. Funt’s group at Memorial Sloan Kettering Cancer Center:
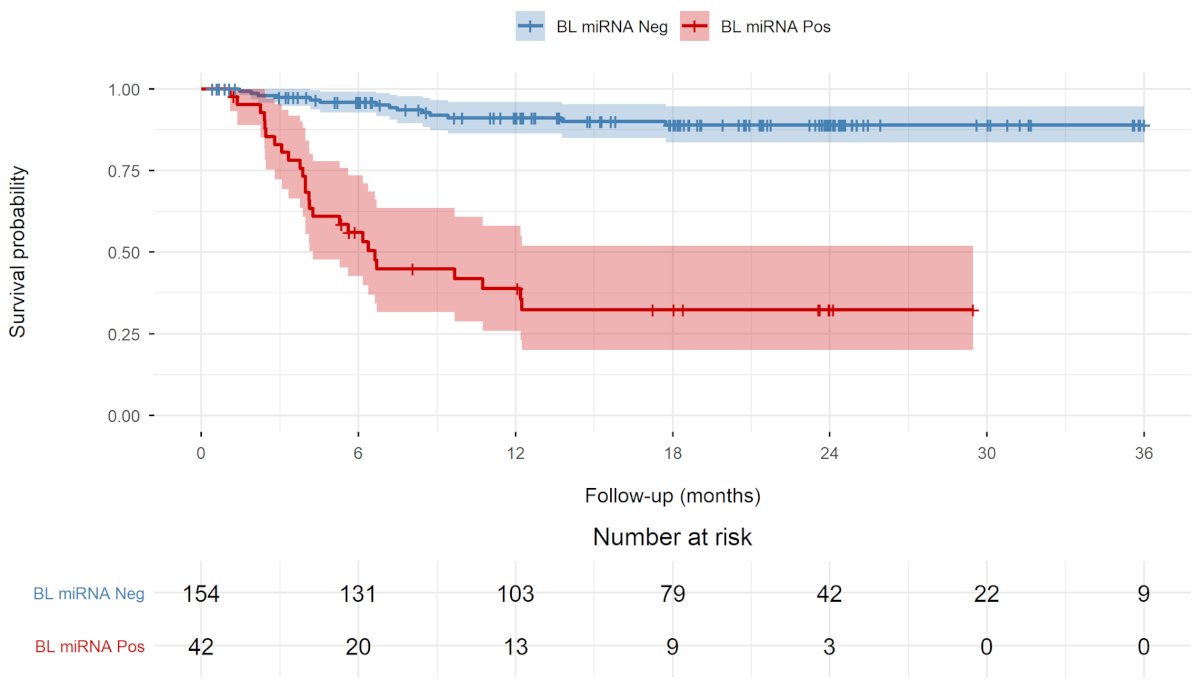
Detectable baseline miR-371 was associated with significantly poorer recurrence-free survival compared to undetectable miR-371 (HR 10.3, 95% CI 5.3 – 19.8; p < 0.001; 24-month recurrence-free survival 32% versus 89%):
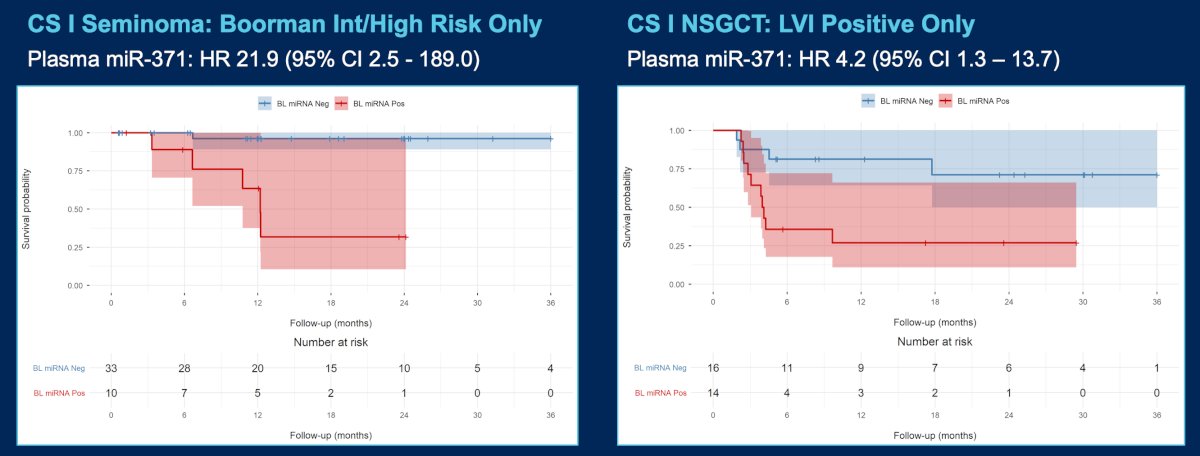
When looking at histology in the groups classified as high risk for relapse based on features in the primary tumor, miR-371 still performed well in distinguishing relapses from non-relapsing patients:
Dr. Funt provided the following conclusions for the CLIMATE (ANZUP 1906) study:
- This was a prospective evaluation of plasma, post-orchiectomy miR-371 as a marker of minimal residual disease specifically for the CSI testicular germ cell tumors
- These results suggest that miR-371 positivity was a strong predictor of relapse and outperformed current risk stratification strategies
- This is an interim analysis with somewhat limited follow-up (18.0 months)
- We are eagerly awaiting the serial sample data
- Does miR-371 relapse predate clinical relapse?
- There is questionable reproducibility in other cohorts, given shorter than expected time to recurrence
- Validation efforts (AGCT1531 and SWOG 1823) are ongoing
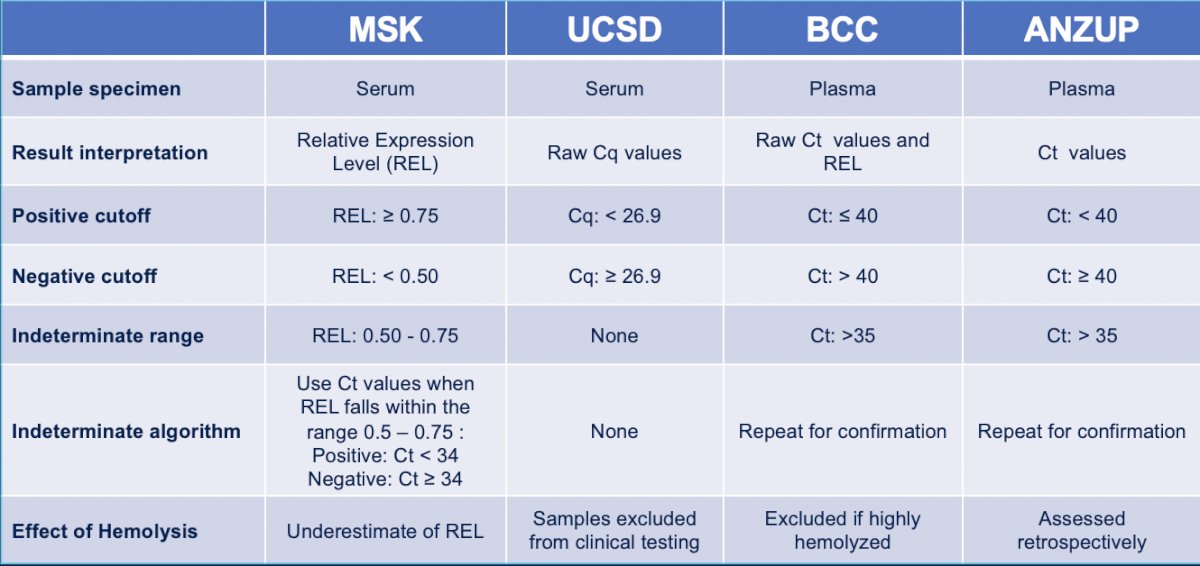
Is miR-371 ready to be used in informing adjuvant interventions in patients with CSI testicular germ cell tumors? Dr. Funt says no, given that there are too many unanswered questions. One question is: is variability in miR-371 measurement a barrier? These assays are being run at multiple institutions, and the methodology in terms of analyte and cutoff is widely variable:
Second, is ctDNA better than miR-371 for minimal residual disease detection in CSI testicular germ cell tumors? Notably, there is a lot less data supporting the use of ctDNA in this disease compared to other tumor types, and ctDNA is more costly, requires a tumor, and takes more time to get results. However, ctDNA is currently widely available as a commercial test.
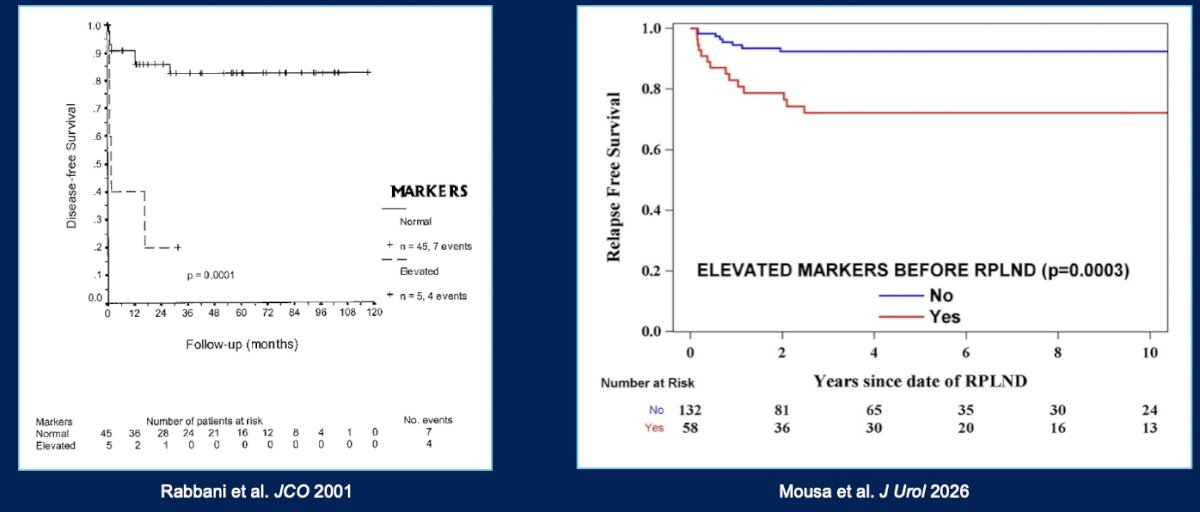
Third, what does miR-371 positivity mean for recurrence patterns? We are much less likely to cure patients with rising markers with surgery alone, given our historical experience of RPLDN in patients with rising AFP and HCG:
Fourth, what will having another blood test do to patient anxiety levels, and how do we ensure access and equity? Without question, Dr. Funt notes that we need to understand what the introduction of a new test will have on patient decision making and anxiety levels, and work on how to ensure access/equity in its implementation.
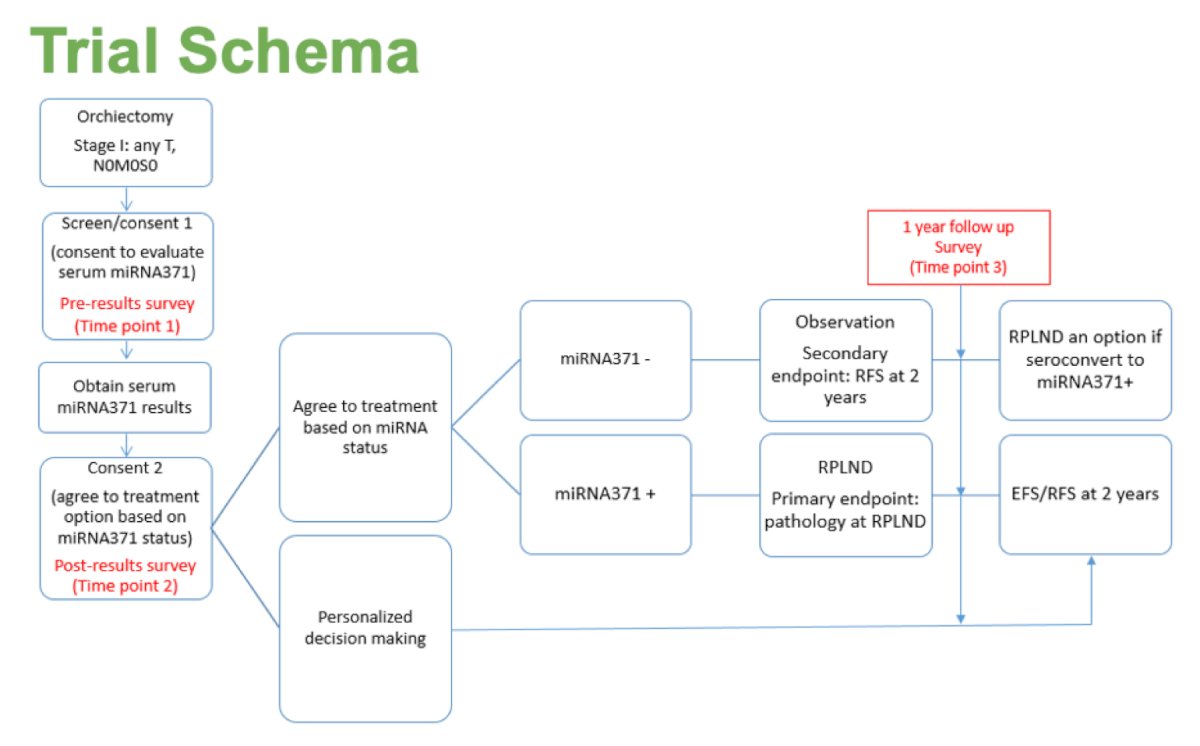
Is miR-371 ready for use in interventional trials? Dr. Funt says yes, particularly based on the CLIMATE results, noting plasma post-orchiectomy miR-371 positivity correlated strongly with 2-year recurrence-free survival. One specific intervention trial is the CLARITY trial, with the following trial schema:
Dr. Funt concluded his discussant presentation with the following take-home points:
- The CLIMATE study demonstrated that plasma miR-371 positivity after orchiectomy can meaningfully risk-stratify patients with CS I testicular germ cell tumors
- There are too many questions/barriers to support its routine use in the clinic today
- Variable testing methodology
- Unclear natural history of miR-371-positive disease
- Potential patient anxiety and access issues
- No data to guide when or how to intervene
- The data from CLIMATE and other studies justify the timely design of interventional trials
Presented by: Samuel A. Funt, MD, Memorial Sloan Kettering Cancer Center and Weill Cornell Medical College, New York, NY
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 26 – Sat, Feb 28, 2026.