(UroToday.com) The 2026 GU ASCO annual meeting featured a kidney cancer session and a presentation by Dr. Razane El Hajj Chehade discussing an international multicenter study assessing adjuvant pembrolizumab in non-clear cell renal cell carcinoma (RCC) after nephrectomy. KEYNOTE-564 demonstrated that adjuvant pembrolizumab improves outcomes after nephrectomy for clear cell RCC.1
However, whether this benefit extends to non-clear cell RCC patients remains uncertain. Dr. El Hajj Chehade and colleagues evaluated the association between adjuvant pembrolizumab and outcomes in patients with non-clear cell RCC who underwent nephrectomy in a multicenter study.
This was a retrospective multicenter cohort study at six international institutions. Eligible adults had non-clear cell RCC treated with nephrectomy and were classified by receipt of adjuvant pembrolizumab. The primary endpoints were disease-free survival, defined as the time from nephrectomy to the first radiographic or clinical recurrence, and overall survival, defined as the time from diagnosis to death or last follow-up. Survival functions were estimated with the Kaplan–Meier method and compared between groups using the log-rank test.
Among 90 non-clear cell RCC patients, 15 (17%) received adjuvant pembrolizumab, and 75 (83%) were observed. The median age at diagnosis was 56.0 years (IQR 44.0–63.0; mean 52.9 ± 13.1) and 62.0 years (IQR 52.0–71.0; mean 59.6 ± 14.7), respectively: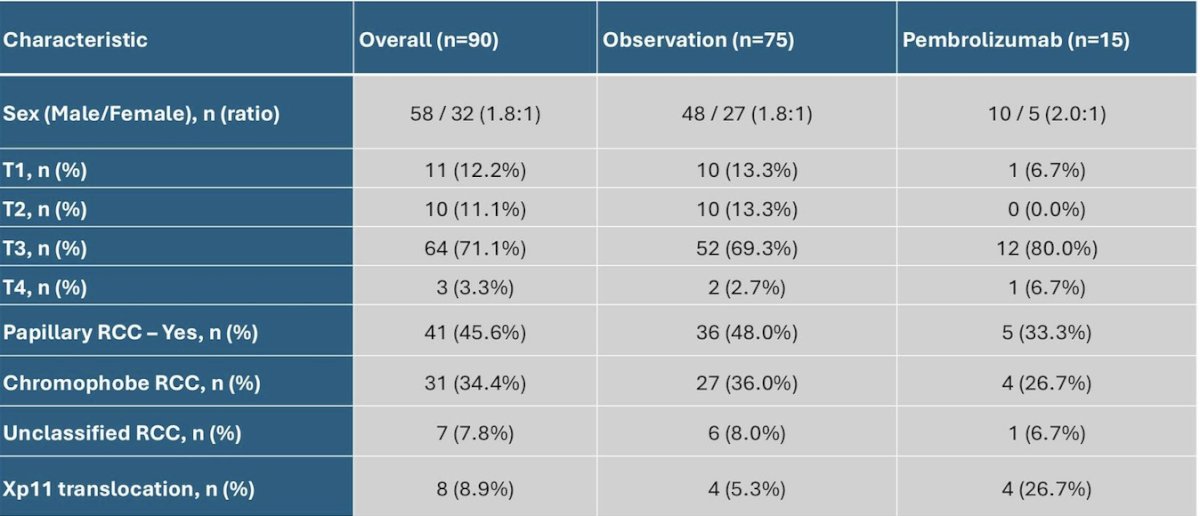
Recurrence occurred in 7/15 (46.7%) with pembrolizumab and 25/75 (44.6%) with observation. There was no significant difference in median disease-free survival (p = 0.75) or overall survival (p = 0.89) between groups. Median disease-free survival was 90.7 months (95% CI, 27.2–NR) with pembrolizumab versus 41.9 months (95% CI, 39.4–NR) with observation. The median overall survival was not reached (95% CI, 65.1–NR) with pembrolizumab versus 52.4 months (95% CI, 44.4–NR) with observation:

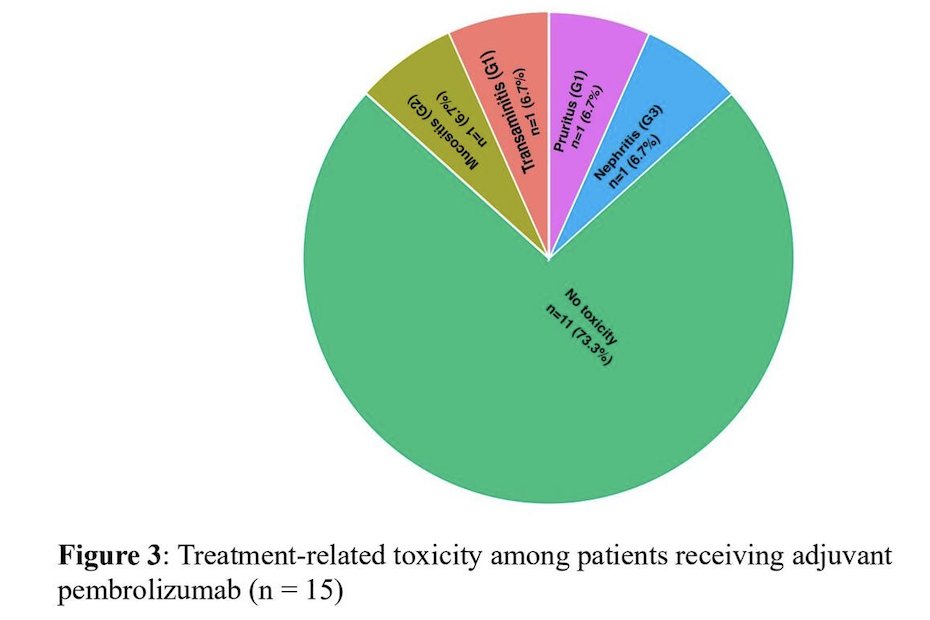
Treatment-related adverse events were observed in 26.7% (4/15) of patients, comprising three grade 1 events and one grade 3 event:
Dr. El Hajj Chehade concluded this presentation discussing an international multicenter study assessing adjuvant pembrolizumab in non-clear cell RCC after nephrectomy with the following take-home points:
- In this descriptive retrospective six-center cohort of non-clear cell RCC post-nephrectomy, adjuvant pembrolizumab did not demonstrate a disease-free survival or overall survival advantage over observation
- A larger multi-institutional cohort is in progress to refine effect estimates using richer clinical detail, with adjusted analyses and prespecified subgroup assessment
Presented by: Razane El Hajj Chehade, MD, Dana Farber Cancer Institute, Boston, MA
References:
- Choueiri TK, Tomczak P, Park SH, et al. Adjuvant Pembrolizumab after Nephrectomy in Renal-Cell Carcinoma. N Engl J Med. 2021 Aug 19;385(8):683-694.
- Choueiri TK, Tomczak P, Park SH, et al. Overall Survival with Adjuvant Pembrolizumab in Renal-Cell Carcinoma. N Engl J Med. 2024 Apr 18;390(15):1359-1371.