(UroToday.com) The 2026 GU ASCO annual meeting featured a kidney cancer session and a presentation by Dr. Eric Li discussing a multicenter retrospective cohort study assessing the response of venous tumor thrombi in renal cell carcinoma (RCC) to immune checkpoint inhibitor therapy. Approximately 10% of patients with RCC have an associated venous tumor thrombus, the presence of which impacts surgical management and increases perioperative risk.
Historical systemic therapy regimens had limited success in downsizing venous tumor thrombus; the impact of immune checkpoint inhibitors on venous tumor thrombus shrinkage is unknown. The primary objective for this study was to assess venous tumor thrombus shrinkage comparing responses to immune checkpoint inhibitor versus non-immune checkpoint inhibitor regimens.
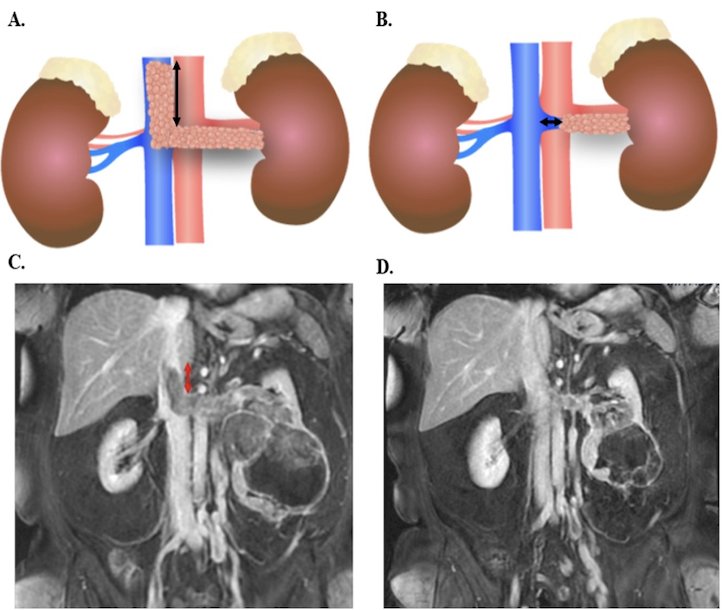
This multicenter retrospective cohort study included patients with RCC and venous tumor thrombus from 2006-2024 who received upfront systemic therapy. Patients were evaluated at tertiary referral centers across Mayo Clinic Rochester, Florida, and Arizona. Systemic therapies were categorized as immune checkpoint inhibitors versus non-immune checkpoint inhibitor regimens. Venous tumor thrombus length was quantified by distance relative to the superior border of the renal vein ostium:
The primary outcome was change in venous tumor thrombus length on serial imaging as measured by absolute length reduction (cm), RECIST version 1.1 criteria, and Mayo venous tumor thrombus level reclassification. Linear mixed-effect models identified associations with venous tumor thrombus shrinkage and clinicopathologic features.
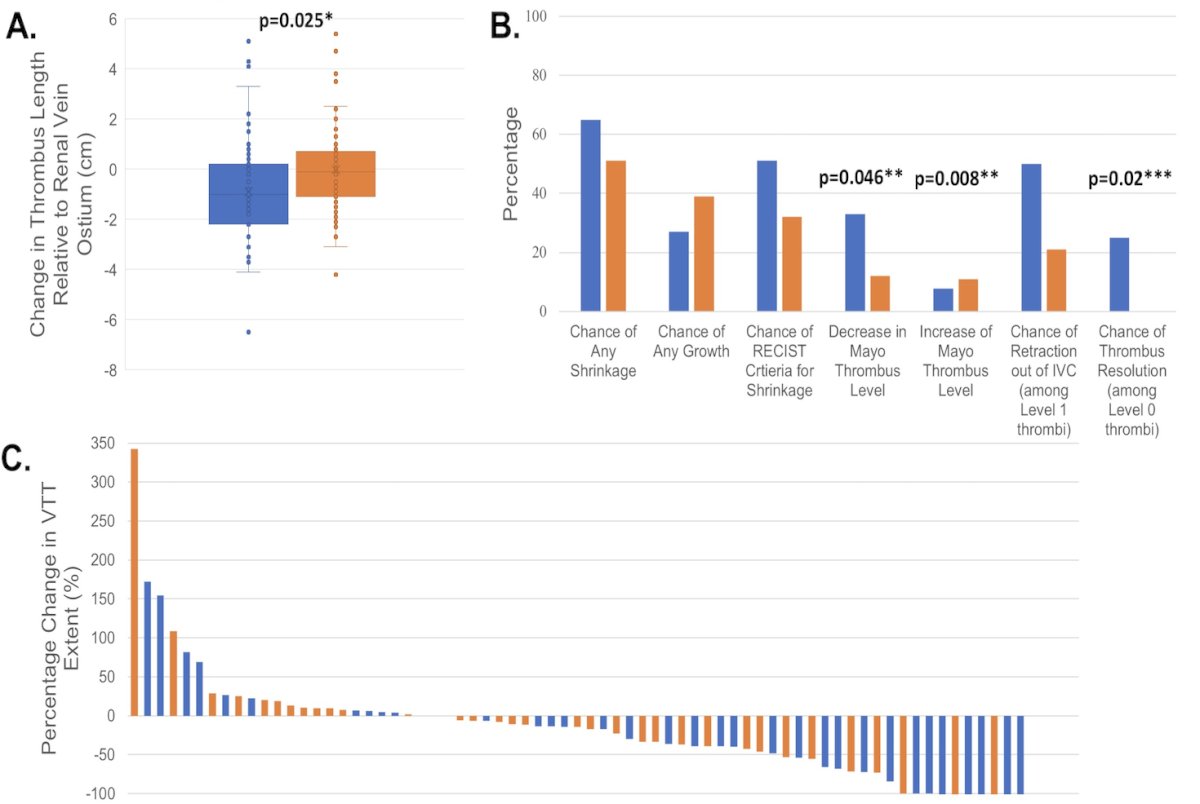
A total of 108 patients with a median age of 65 years (IQR 57-71) were included, of whom 49 (45%) received immune checkpoint inhibitor regimens. Immune checkpoint inhibitor regimens were associated with greater venous tumor thrombus shrinkage (1 cm versus 0.1 cm, p = 0.02), increased RECIST responses (51% versus 32%, p = 0.046), and a higher rate of downstaging per Mayo venous tumor thrombus level (33% versus 12%, p = 0.008) compared to non-immune checkpoint inhibitor regimens:
On multivariable linear mixed-effect model analysis, immune checkpoint inhibitor regimens remained more likely to result in venous tumor thrombus shrinkage compared to non-immune checkpoint inhibitor regimens (-0.12 cm/month, 95% CI –0.24-0.00, p = 0.046). Absence of abdominal lymphadenopathy was also associated with venous tumor thrombus shrinkage (-0.18 cm/month, 95% CI -0.06- -0.30, p = 0.004). Initial Mayo venous tumor thrombus level, IMDC risk, and number of metastatic sites were not associated with venous tumor thrombus shrinkage.
Dr. Li concluded his presentation discussing a multicenter retrospective cohort study assessing the response of venous tumor thrombi in RCC to immune checkpoint inhibitor therapy with the following take-home points:
- Treatment with immune checkpoint inhibitor regimens resulted in venous tumor thrombus shrinkage and Mayo venous tumor thrombus level reduction
- This is a particularly important area of exploration, as radical nephrectomy and tumor thrombectomy carry up to a 40% risk of perioperative major complications
- These data support using immune checkpoint inhibitor regimens for patients with RCC with venous tumor thrombus who are not candidates for upfront surgery, and prioritizing immune checkpoint inhibitor regimens in neoadjuvant clinical trials
Presented by: Eric Li, MD, Mayo Clinic, Rochester, MN