(UroToday.com) The 2026 GU ASCO annual meeting featured a kidney cancer session and a presentation by Dr. George Zhang discussing geographic disparities in the availability of renal cell carcinoma (RCC) clinical trials in the US. Clinical trials for cancer tend to be less available in regions of the US corresponding to high socioeconomic vulnerability,1 however, specific patterns for RCC have yet to be reported. As such, Dr. Zhang and collaborators aimed to evaluate the current county-level distribution of RCC clinical trials in the United States.
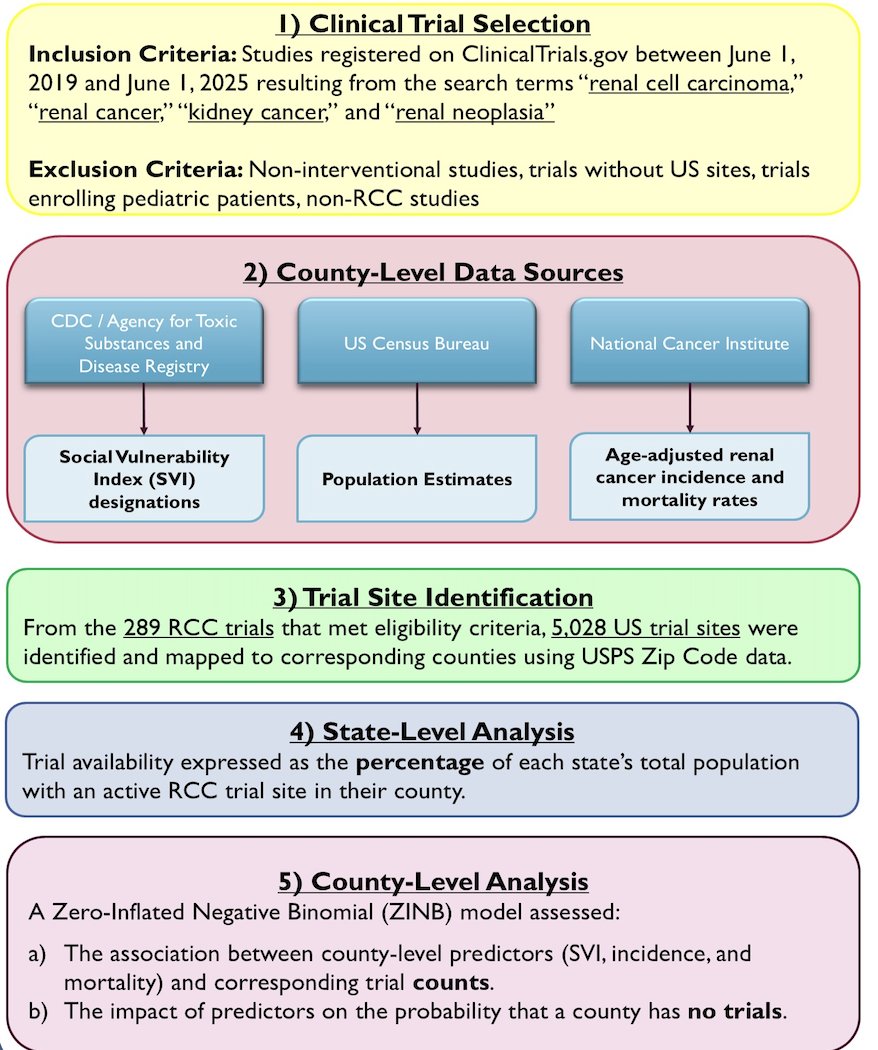
Using ClinicalTrials.gov, they identified all interventional trials between June 1, 2019, and June 1, 2025, enrolling adult patients with RCC. Using US Postal Service data, they recorded every unique county for the zip code listed for each trial. Trial characteristics were summarized descriptively. The investigators used the Centers for Disease Control and Prevention (CDC) Social Vulnerability Index (SVI) designations to reflect county demographics and socioeconomic status. Age-adjusted renal cancer incidence and mortality rates were obtained from the National Cancer Institute (NCI). To account for overdispersion of trial availability and a high proportion of counties with no trials, they used a zero-inflated negative binomial regression model to assess the association between the number of RCC trials per county and corresponding incidence, mortality, and SVI. To account for county size, adjustments were made for trial rates by number of households:
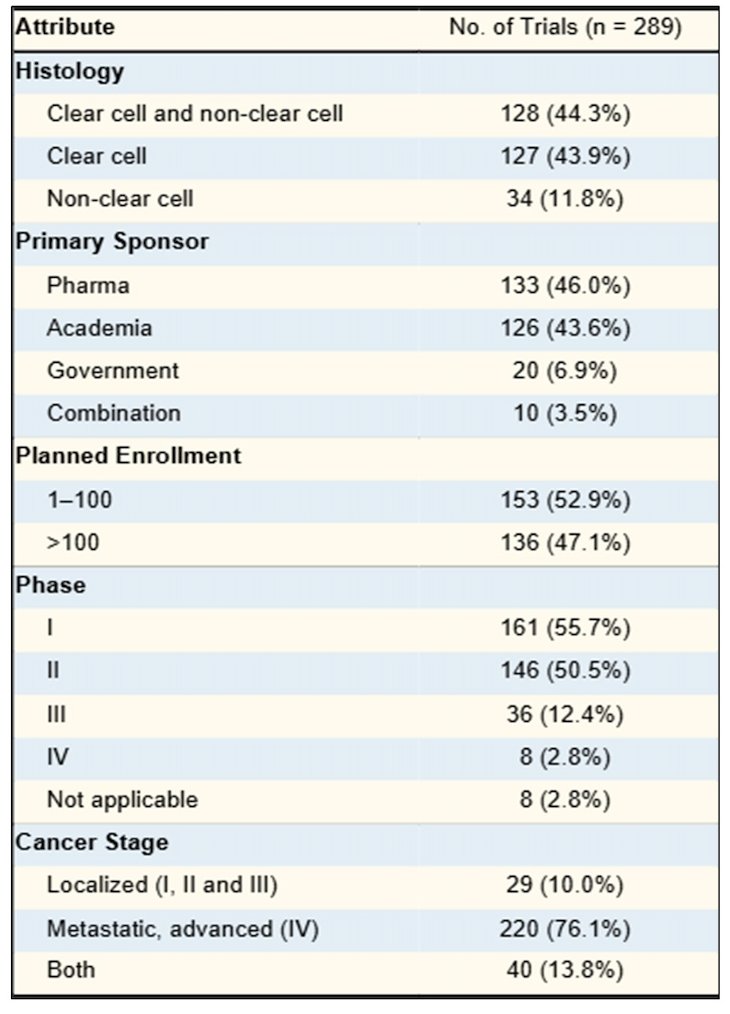
Of 289 eligible trials, 127 (43.9%) enrolled patients with only clear cell RCC and 34 (11.8%) with only non-clear cell RCC. Pharmaceutical companies sponsored the greatest proportion of trials (46.0%), followed closely by academia (43.6%). Most trials (76.1%) enrolled patients with advanced or metastatic disease:
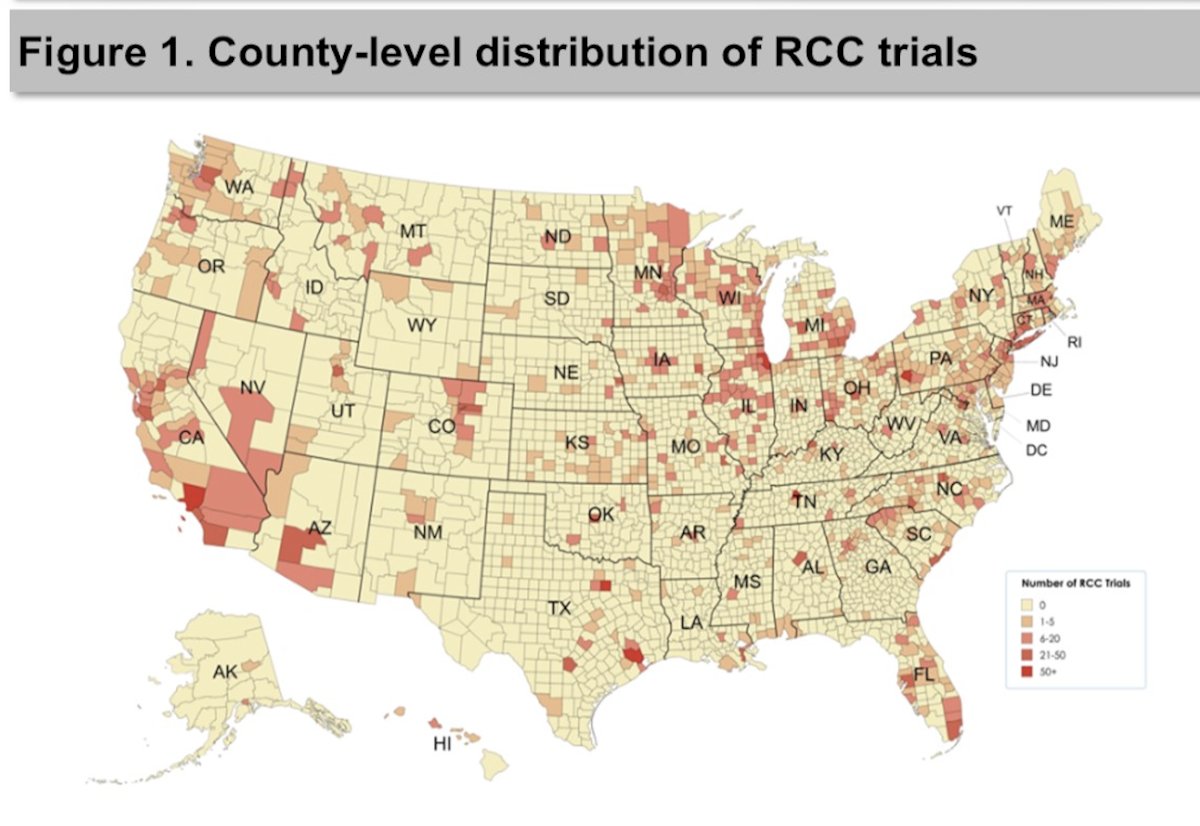
Only 672 (21.4%) of all US counties had at least one clinical trial location, and the baseline odds of a county lacking an RCC trial were high (OR 4.55, 95% CI 2.41-8.58):
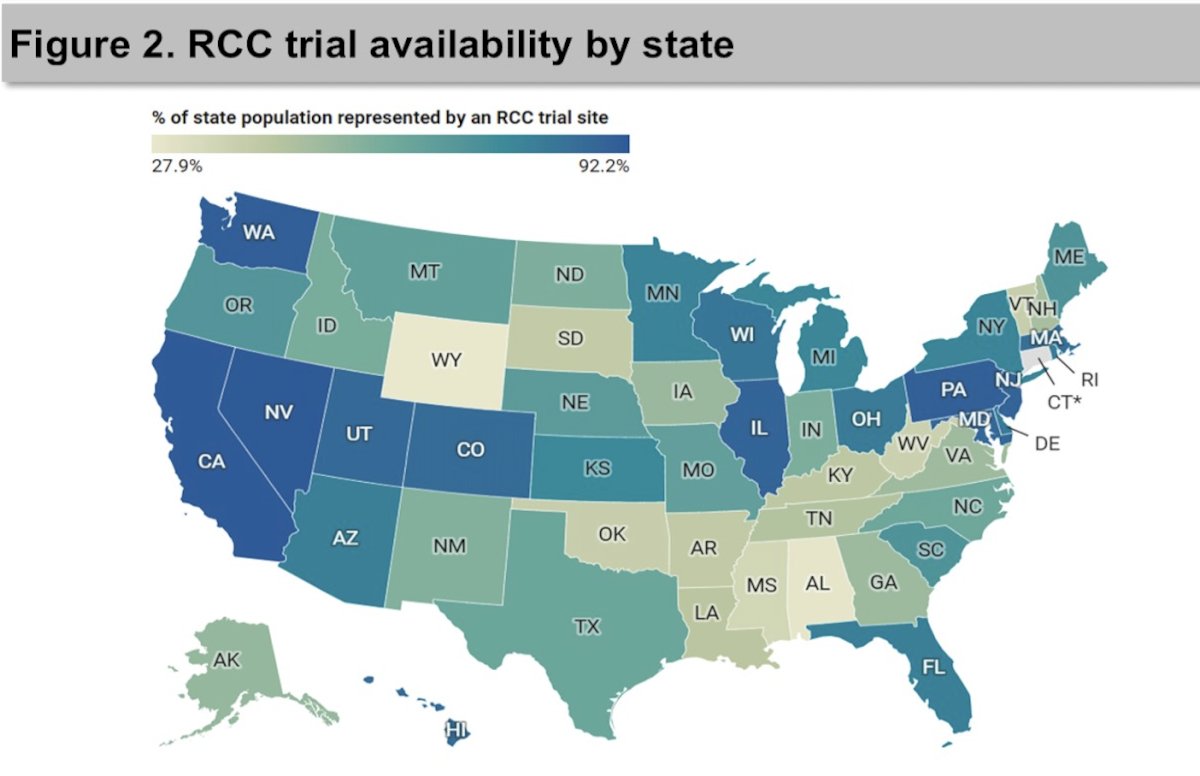
No state had an RCC clinic trial in every county. Nevada (92.2%), California (91.8%, and Washington (90.3%) had the highest proportions of RCC trial representation, whereas Wyoming (27.9%), Alabama (29.2%), and Mississippi (36.2%) had the lowest:
Compared with high-SVI counties (most socially vulnerable), those in the medium-high, low-medium, and low-SVI counties had 1.8-fold (95% CI 1.38-2.36), 2.0-fold (95% CI 1.50-2.58), and 3.1-fold (95% CI 2.29-4.13) higher trial incidence rates, respectively (all p < 0.001):
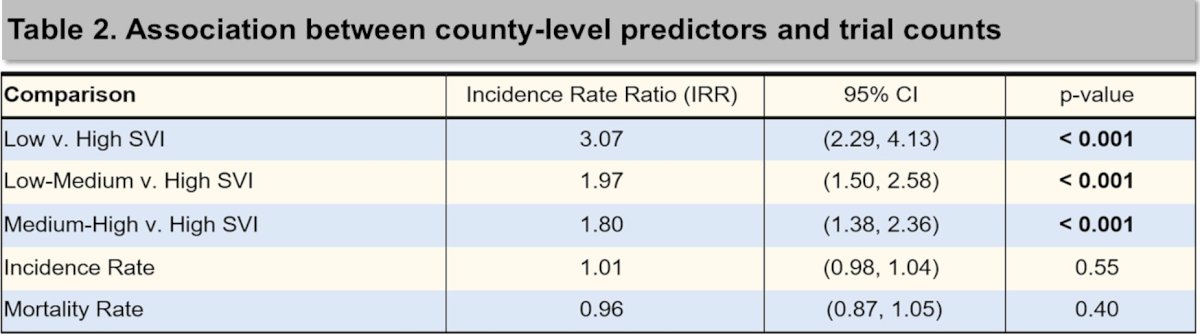
Of the 5,028 US trial sites analyzed, 1,681 (33.4%) were in counties with the lowest renal cancer incidence quintile, while only 254 (5.1%) were in counties with the highest incidence quintile. This pattern held for counties with the lowest and highest mortality quintiles, with 1,508 (30.0%) and 183 (3.6%) trials, respectively.
Dr. Zhang concluded his presentation discussing geographic disparities in the availability of RCC clinical trials in the US with the following take-home points:
- Most US counties lacked RCC clinical trial representation
- Counties with higher social vulnerability had markedly lower RCC clinical trial availability
- Social vulnerability reflects census-derived variables such as socioeconomic status, household composition, disability, minority status, English proficiency, and transportation
- These findings highlight geographic and structural disparities in access to novel RCC therapies within the US, and emphasize the need for trial design and site selection that account for regional vulnerability
Presented by: George Zhang, City of Hope Comprehensive Cancer Center, Duarte, CA
Reference:
- Kirkwood MK, Schenkel C, Hinshaw DC, et al. State of Geographic Access to Cancer Treatment Trials in the United States: Are Studies Located where Patients Live? JCO Oncol Pract. 2025 Mar;21(3):427-437.