(UroToday.com) The 2026 GU ASCO annual meeting featured a kidney cancer session and a presentation by Dr. Alexandre Faco Jr discussing a head-to-head comparison of pembrolizumab + axitinib versus pembrolizumab + lenvatinib in metastatic renal cell carcinoma (RCC). Immune checkpoint inhibitor-tyrosine kinase inhibitor (IO-TKI) combinations have transformed first-line treatment for metastatic RCC. Pembrolizumab + axitinib and pembrolizumab + lenvatinib have each demonstrated efficacy in randomized trials, but there is no head-to-head data comparing these regimens, leaving clinicians with limited real-world evidence to guide individualized treatment decisions.
For this study, the investigators conducted a retrospective cohort study using the CKCis registry. Patients with confirmed metastatic RCC who received first-line pembrolizumab + axitinib or pembrolizumab + lenvatinib were included. The primary endpoint was progression-free survival, and key secondary endpoints included overall survival and safety.
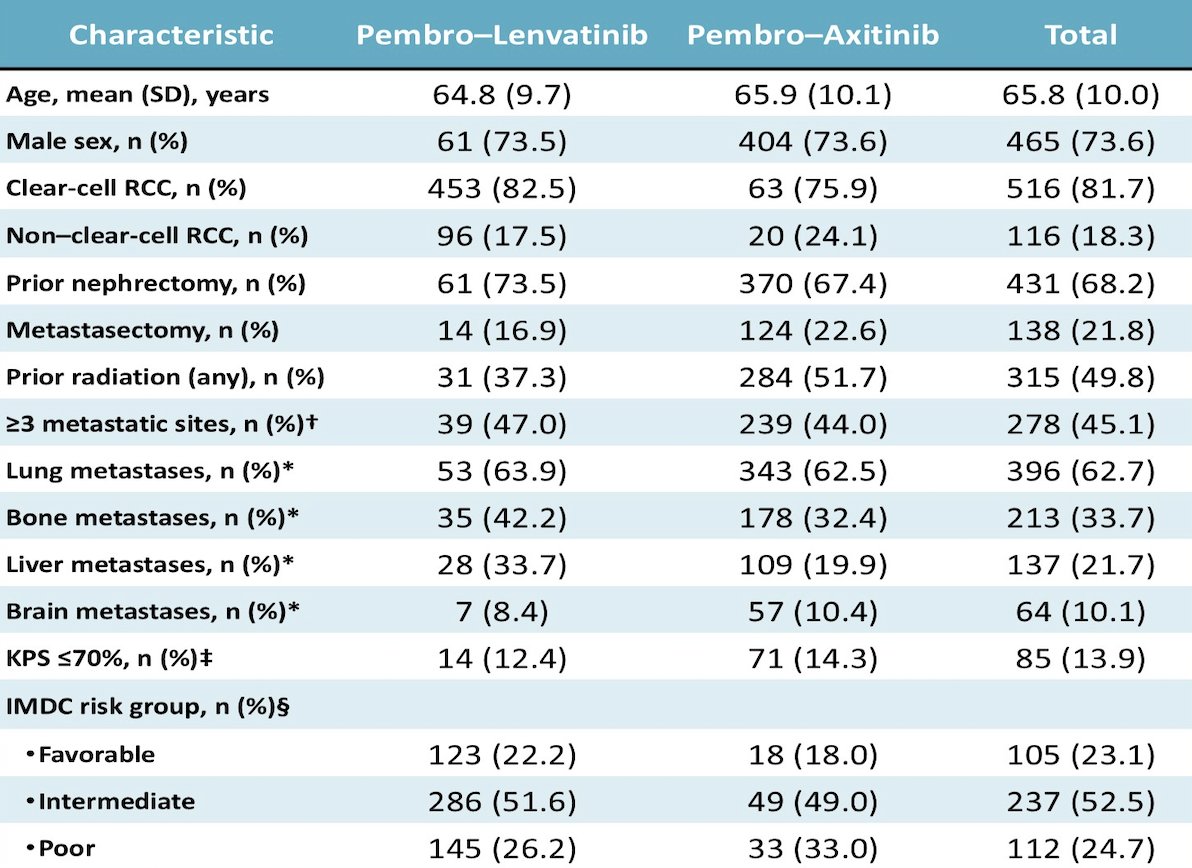
A total of 632 patients were identified, with a median age of 66 years and 73.5% males, including 516 (81.6%) with clear cell and 116 (18.4%) with non-clear cell histology. Of these, 549 (86.9%) received pembrolizumab + axitinib and 83 (13.1%) received pembrolizumab + lenvatinib:
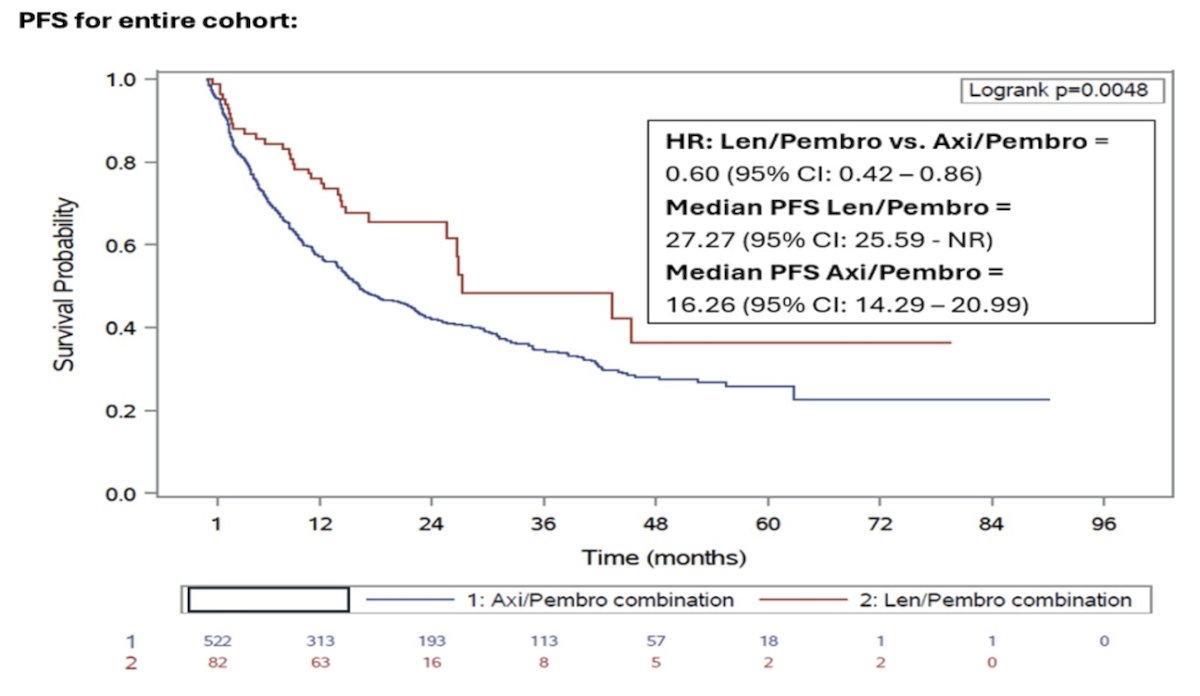
Over a median follow-up of 28.9 months, progression-free survival was improved with pembrolizumab + lenvatinib compared with pembrolizumab + axitinib (HR 0.60, 95% CI 0.42-0.86):
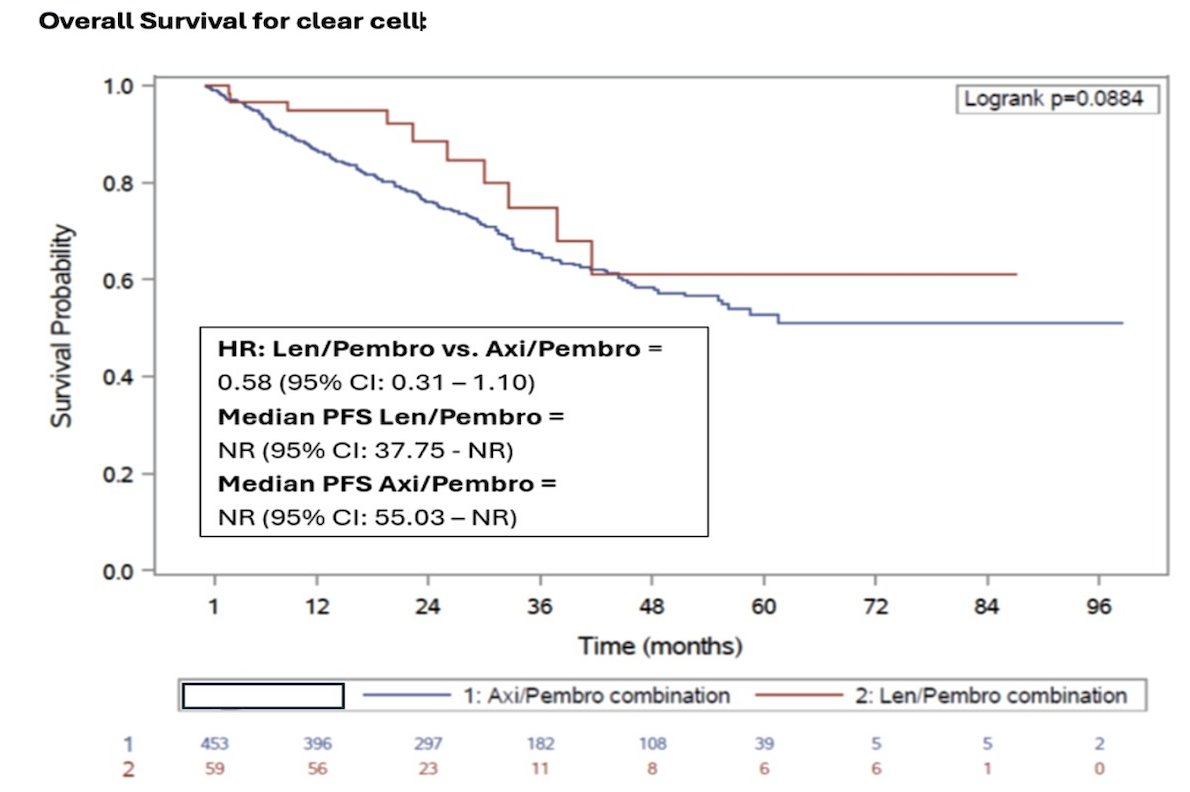
In the clear cell RCC cohort, overall survival favored pembrolizumab + lenvatinib, but this result was not statistically significant (HR 0.58, 95% CI 0.31-1.10):
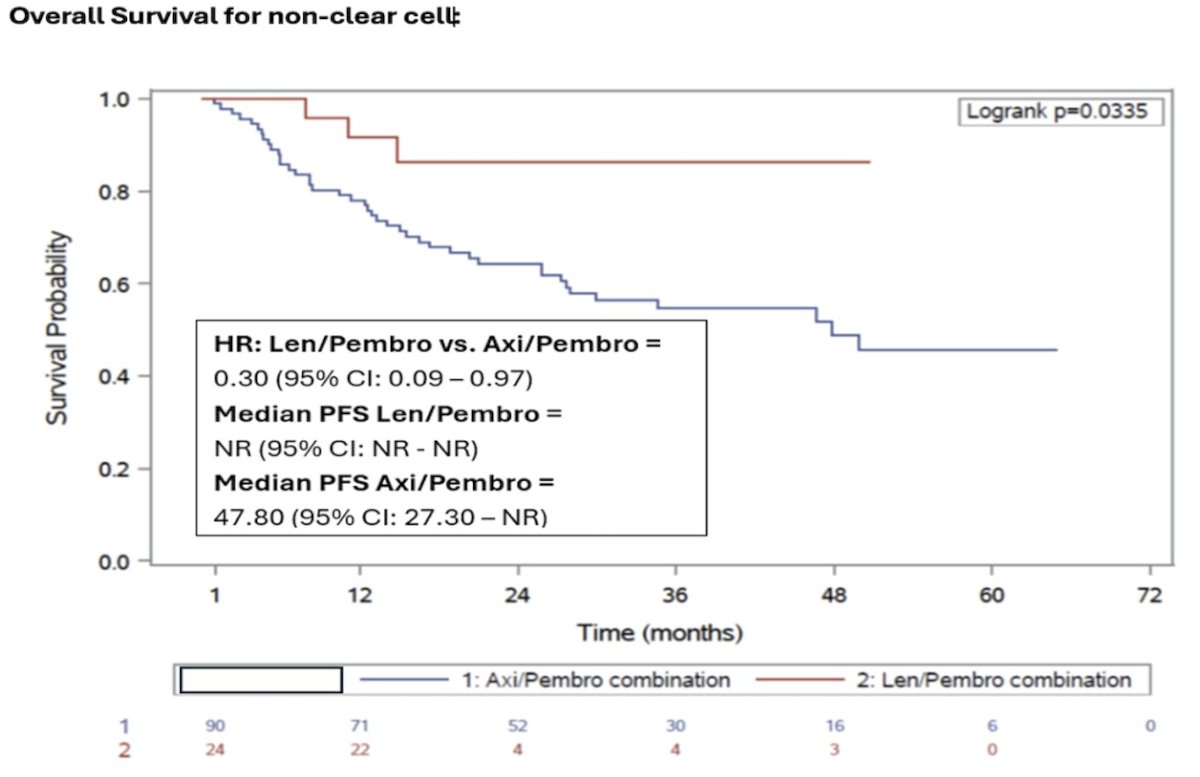
However, for the non-clear cell RCC cohort, overall survival was significantly improved with pembrolizumab + lenvatinib (HR 0.30, 95% CI 0.09-0.97):
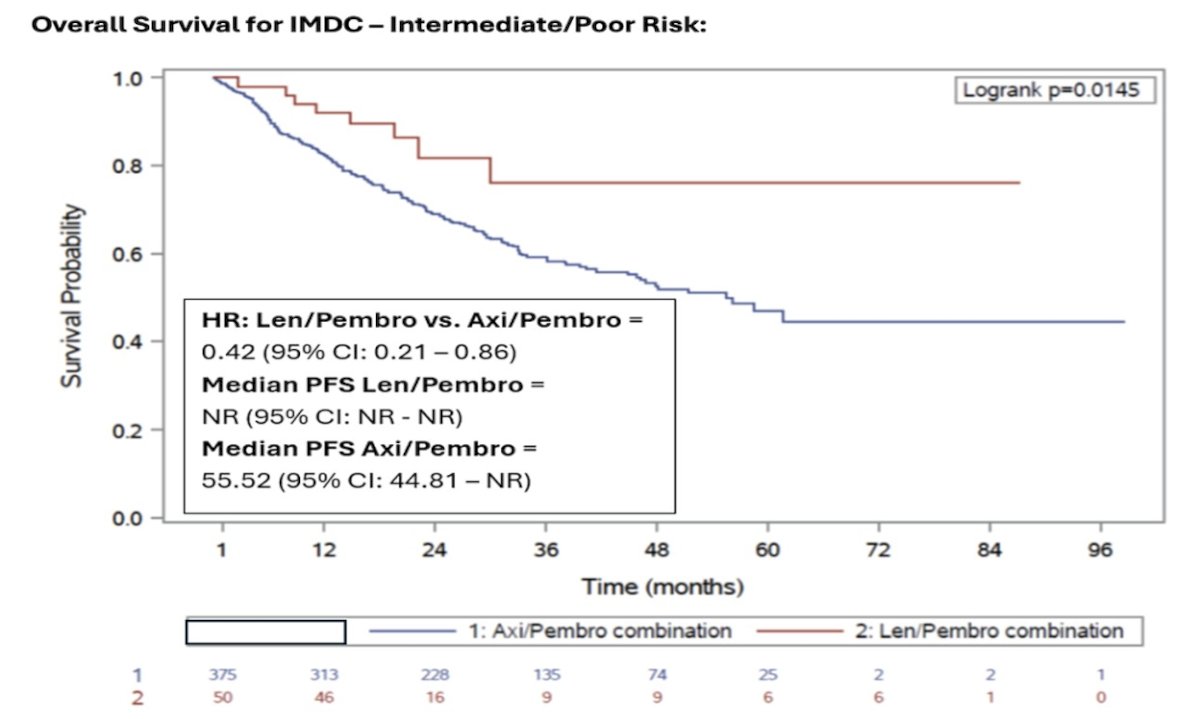
Regarding overall survival by IMDC risk, there was no difference between pembrolizumab + lenvatinib versus pembrolizumab + axitinib for good risk patients (HR 0.93, 95% CI 0.22-3.97), however, for intermediate/poor risk patients, there was a survival benefit with pembrolizumab + lenvatinib (HR 0.42, 95% CI 0.21-0.86):
Multivariable Cox analysis adjusting for age and IMDC risk showed that pembrolizumab + axitinib was associated with an increased risk of death compared with pembrolizumab + lenvatinib (HR 2.15, 95% CI 1.14-4.06; p = 0.019). Dose reductions of the TKI occurred more frequently with pembrolizumab + lenvatinib (50%) than with pembrolizumab + axitinib (35.3%). Both regimens were associated with manageable but frequent toxicities, including fatigue, diarrhea, and anorexia, which were commonly observed with pembrolizumab + axitinib. Pembrolizumab + lenvatinib showed a similar overall profile but a higher rate of grade 3 proteinuria. No grade 5 events occurred.
Dr. Faco concluded his presentation discussing a head-to-head comparison of pembrolizumab + axitinib versus pembrolizumab + lenvatinib in metastatic RCC with the following take-home points:
- In this real-world metastatic RCC cohort, treatment with pembrolizumab + lenvatinib was associated with better progression-free survival and overall survival compared to pembrolizumab + axitinib, but with higher dose modification rates
- These findings align with outcomes observed in pivotal trials and suggest that pembrolizumab + lenvatinib may offer a clinically meaningful benefit in routine practice
- Prospective studies are needed to validate these results and to further explore the balance between efficacy and tolerability among first-line IO-TKI combinations
Presented by: Alexandre Faco Jr, MD, McGill University Health Centre, Montreal, Quebec, Canada