(UroToday.com) The 2026 GU ASCO annual meeting featured a kidney cancer session and a presentation by Dr. Neeraj Agarwal discussing a biomarker analysis from the phase 2 LITESPARK-013 study of two different belzutifan doses in participants with advanced clear cell RCC. Based on results of the phase 3 LITESPARK-005 study, the HIF-2α inhibitor belzutifan is approved at a dose of 120 mg QD for patients with previously treated advanced RCC after prior immune checkpoint and antiangiogenic therapies1 The LITESPARK-013 study showed similar efficacy and safety between 200 mg and 120 mg (approved dose) doses of belzutifan in patients with pretreated advanced clear cell RCC.2 At ASCO GU 2026, Dr. Agarwal and colleagues reported exploratory biomarker analyses (including HIF-2α IHC, RNAseq, and whole exome sequencing) from this study.
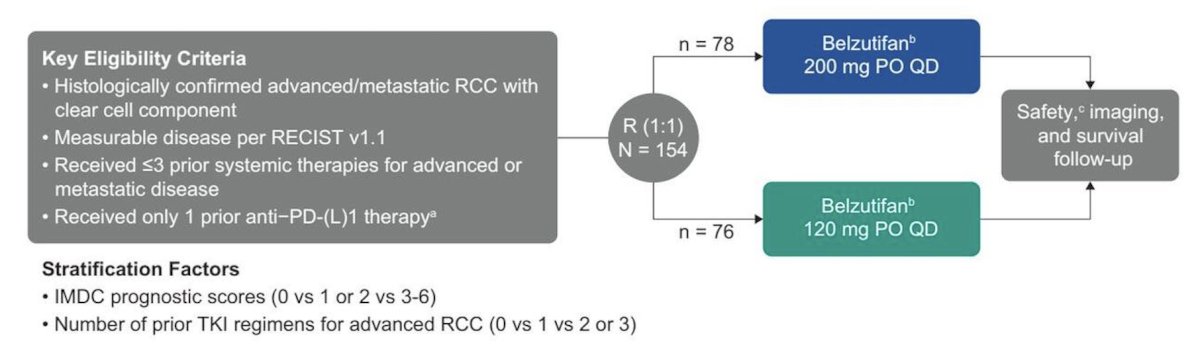
Patients with advanced clear cell RCC whose disease progressed after 1-3 prior systemic therapies (including an anti–PD-[L]1 therapy) were randomly assigned 1:1 to belzutifan 200 mg or 120 mg daily:
Treatment arms were pooled for biomarker analyses. The association of HIF-2α tumor proportion score (IHC D6T8V) and H-score (sum of each percentage multiplied by its corresponding intensity [0, 1+, 2+, 3+]) with clinical outcomes (objective response rate, progression free survival, overall survival) was tested at prespecified multiplicity-adjusted α = 0.05. Associations of RNAseq-based HIF-2α co-expression and HIF-2α cancer cell scores, glycolysis, angiogenesis, and other HIF-2α–related genes and signatures were tested at prespecified multiplicity-adjusted α = 0.10. Associations for molecular subtypes3 were tested at nominal α = 0.05. DNA mutations were evaluated by whole exome sequencing.
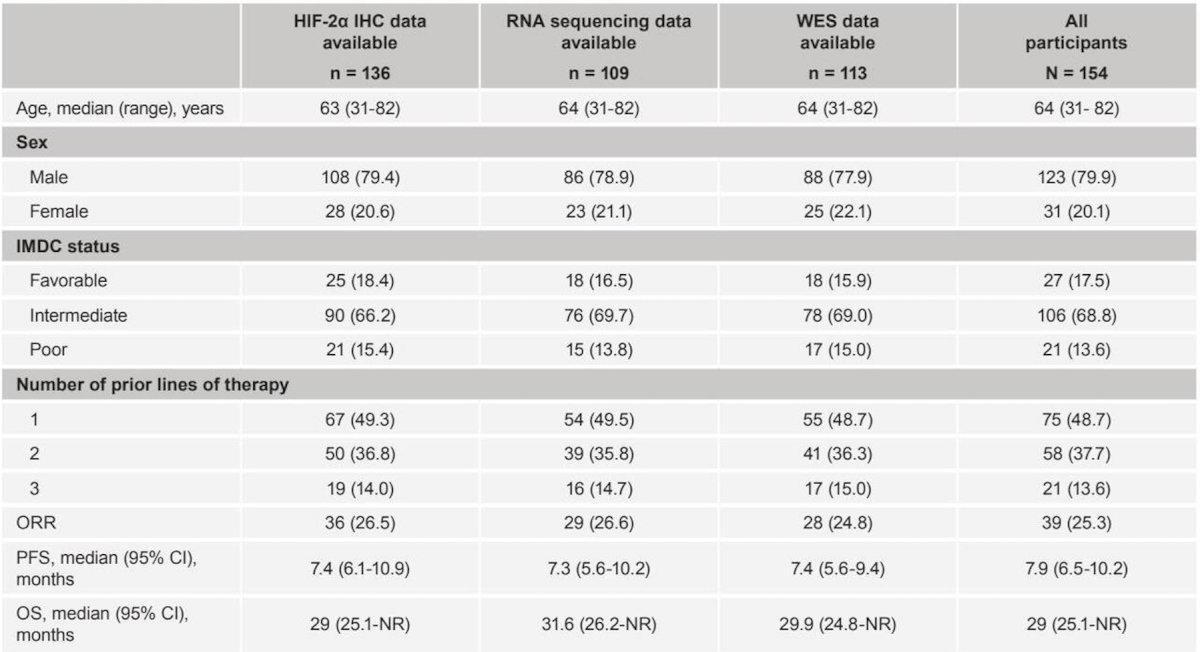
Among 154 patients, HIF-2α IHC was evaluable in 136 (88.3%) patients, RNA sequencing in 109 (70.8%) patients, and whole exome sequencing in 113 (73.4%) patients. The baseline characteristics of these patients are as follows:
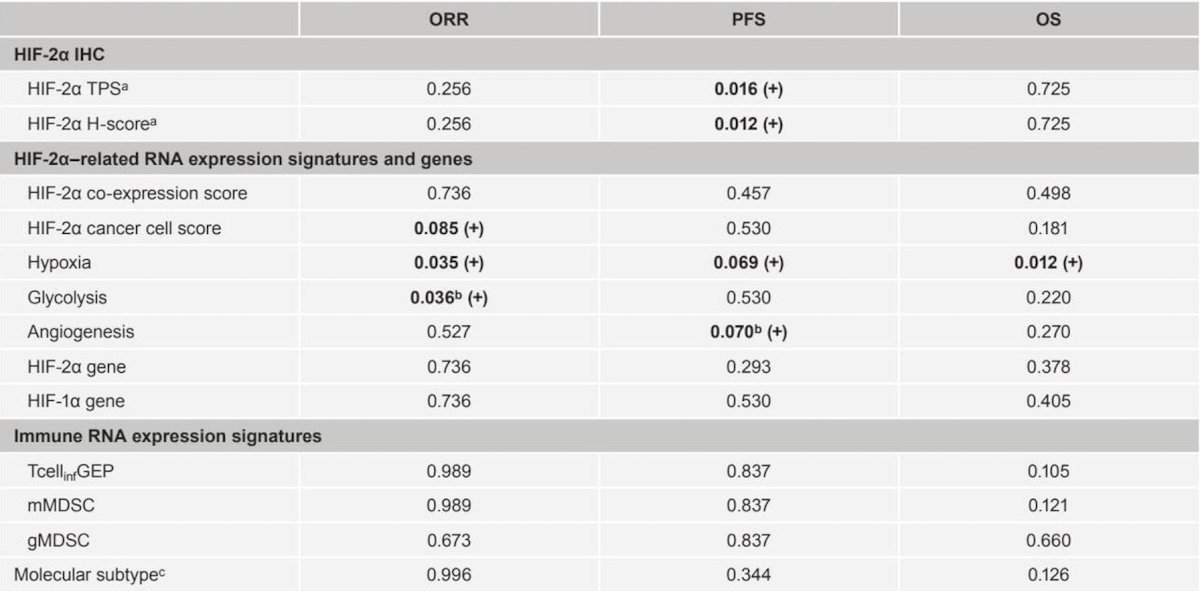
HIF-2α tumor proportion score and H-score were positively associated with progression free survival (p = 0.016 and 0.012, respectively), but not objective response rate or overall survival. HIF-2α cancer cell score was positively associated with objective response rate (p = 0.085), but not progression free survival or overall survival. No associations with clinical outcome were observed for HIF-2α co-expression score. Glycolysis and angiogenesis were positively associated with objective response rate (p = 0.036) and progression free survival (p = 0.070), respectively, but these were no longer significant after adjustment for other signatures:
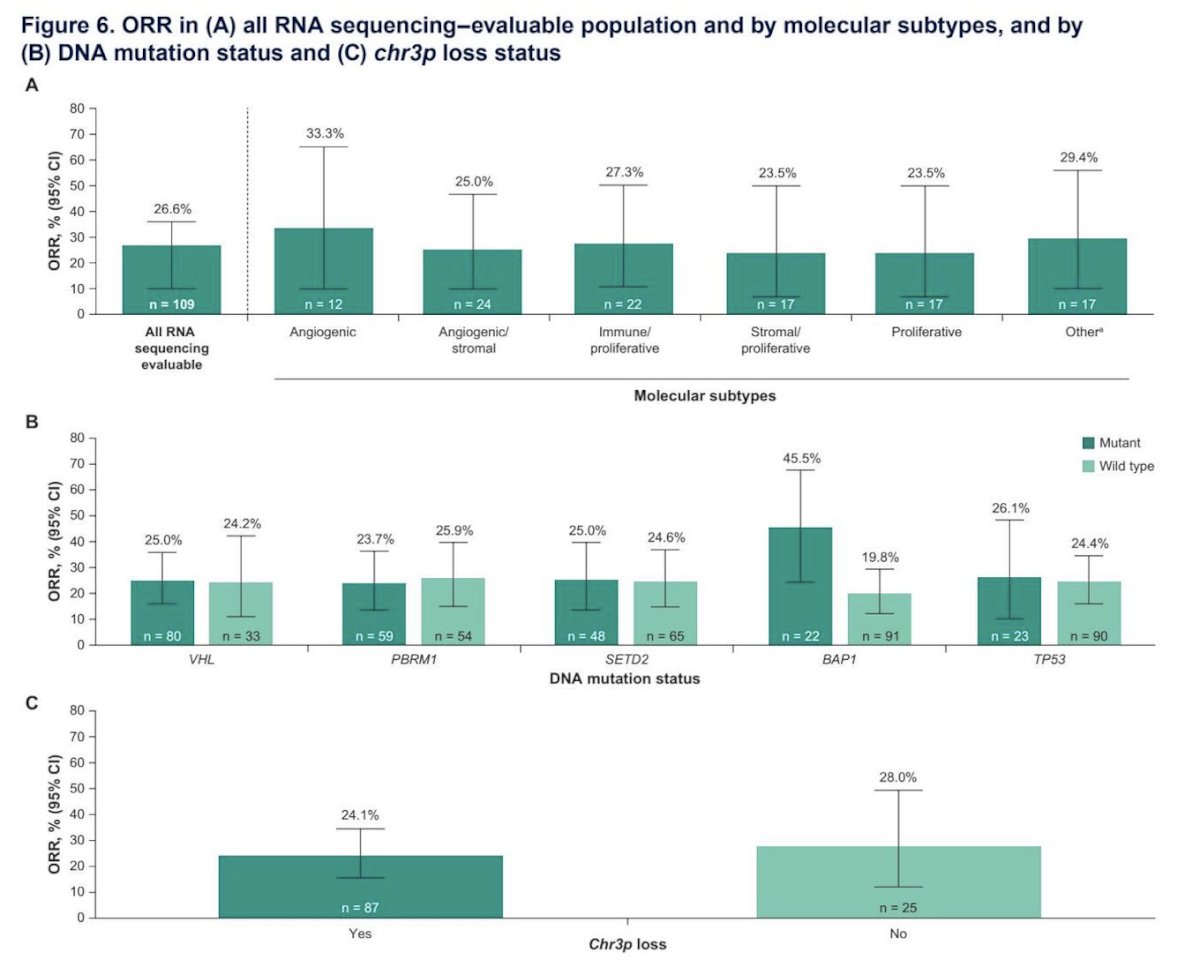
Objective response rate was consistent across molecular subtypes and by DNA mutation status, with a notably higher objective response rate in the BAP1 mutant versus wild-type group:
Dr. Agarwal concluded his presentation discussing a biomarker analysis from the phase 2 LITESPARK-013 study of two different belzutifan doses in participants with advanced clear cell RCC with the following take-home points:
- In this first RNA and whole exome sequencing biomarker analysis of belzutifan, HIF-2α TPS, HIF-2α H-score, hypoxia signature score, and BAP1 mutation were potentially associated with ≥1 improved outcome (objective response rate, progression free survival, and/or overall survival) in participants with previously treated advanced clear cell RCC
- The hypoxia signature was positively associated with objective response rate, progression free survival, and overall survival
- BAP1 mutation was potentially predictive of improved objective response rate
- HIF-2α TPS and HIF-2α H-score were only positively associated with progression free survival
- Glycolysis and angiogenesis were positively associated with objective response rate and progression free survival, respectively, but these were no longer significant after adjustment of the hypoxia signature
- Molecular subtypes, other RCC-related signatures, and VHL mutation showed no associations or trends with clinical outcomes
- Hypoxia signature scores were comparable between BAP1-mutant and wild-type tumors, suggesting that BAP1 mutational status and hypoxia signature scores were independent of each other
- Sample sizes were small, and the results of this exploratory analysis should be interpreted with caution
- This analysis establishes a foundation for subsequent research
Presented by: Neeraj Agarwal, MD, Huntsman Cancer Institute, University of Utah, Salt Lake City, UT
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026.
References:
- Choueiri TK, Powles T, Peltola K, et al. Belzutifan versus Everolimus for Advanced Renal-Cell Carcinoma. N Engl J Med. 2024 Aug 22;391(8):710-721.
- Agarwal N, Brugarolas J, Ghatalia P, et al. Randomized phase II dose comparison LITESPARK-013 study of belzutifan in patients with advanced clear cell renal cell carcinoma. Ann Oncol. 2024 Dec;35(12):1148-1156.
- Motzer RJ, Banchereau R, Hamidi H, et al. Molecular subsets in renal cancer determine outcome to checkpoint and angiogenesis blockade. Cancer Cell. 2020 Dec 14;38(6):803-817.