(UroToday.com) The 2026 GU ASCO annual meeting featured a kidney cancer session and a presentation by Dr. Jiwei Huang discussing fruquintinib + serplulimab as first line therapy in metastatic or unresectable non-clear cell RCC. Despite recent advancements, non-clear cell RCC remains a significant therapeutic challenge with a poor prognosis, thus innovative therapeutic strategies are urgently needed. Dr. Huang and colleagues previously reported promising anti-tumor activity of the combination of fruquintinib (a small-molecule VEGFR inhibitor) and serplulimab (anti–PD-1 antibody) as first line therapy in metastatic or unresectable non-clear cell RCC patients. At ASCO GU 2026, Dr. Huang presented the updated efficacy and safety data.
This study was designed to enroll 39 treatment-naïve patients (aged 18–80 years, ECOG performance status 0–1) with metastatic or unresectable non-clear cell RCC. All patients received fruquintinib (5 mg daily, orally, 2 weeks on/1 week off) + serplulimab (4.5 mg/kg, IV, Q3W):
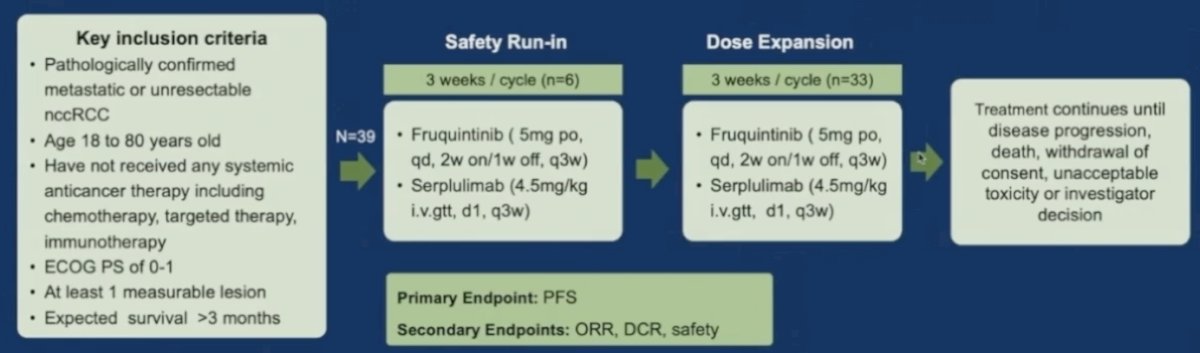
The primary endpoint was progression free survival per RECIST 1.1, while secondary endpoints included objective response rate, disease control rate, and safety.
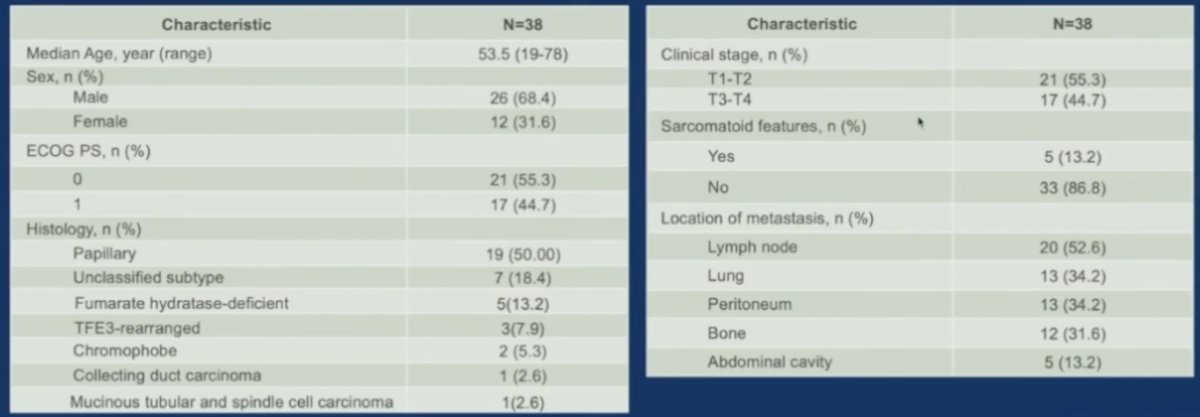
As of September 30, 2025, 38 patients were enrolled across 3 centers. The median age was 53.5 years (range 19–78), with 68.4% male, and 44.7% had an ECOG performance status of 1. Histological subtypes included papillary (50.0%), unclassified (18.4%), fumarate hydratase-deficient (13.2%), TFE3-rearranged (7.9%), chromophobe (5.3%) and rare variants (5.2%). Sarcomatoid features were observed in 5 patients. The most frequent metastatic sites were lymph nodes (52.6%), lungs (34.2%), and the peritoneum (34.2%):
With a median follow-up of 10 months (95% CI: 9.2–15.9) for progression free survival, the median progression free survival was not reached, and the 9-month progression free survival rate was 87.3%. Among the 36 efficacy evaluable patients, 1 achieved complete response, 18 achieved partial response, and 16 had stable disease, yielding an objective response rate of 52.8% (95% CI 36.5–69.1) and a disease control rate of 97.2% (95% CI 85.5–99.9):
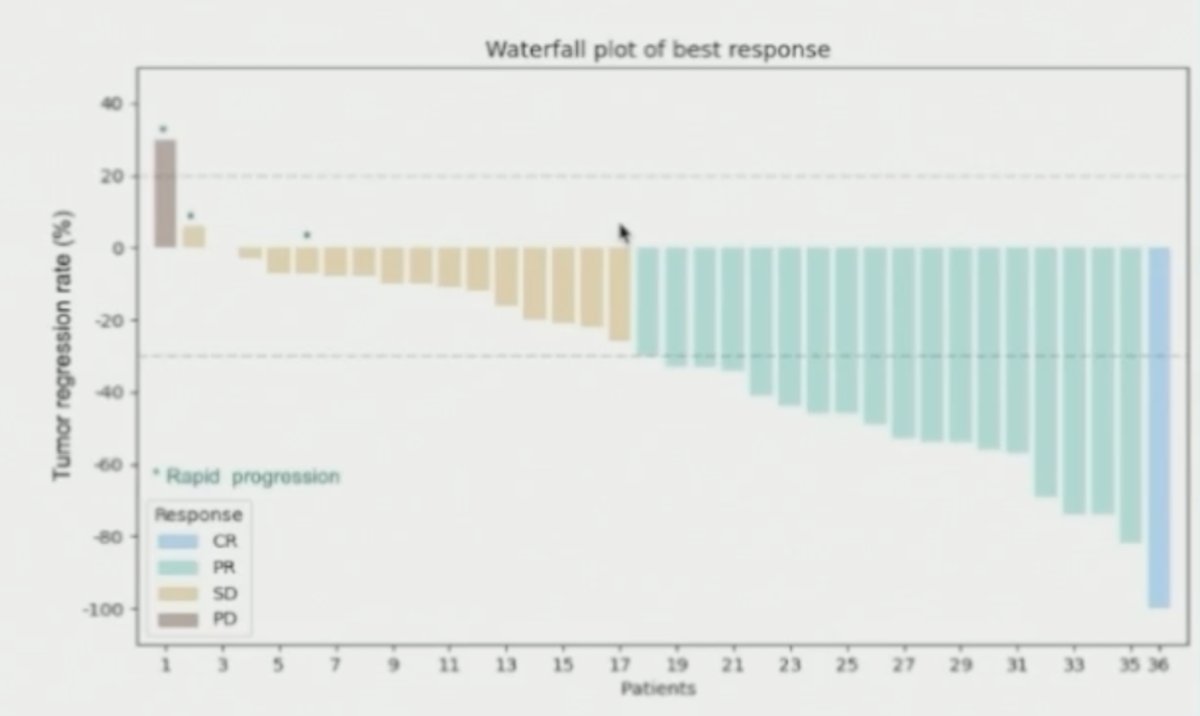
Three patients experienced rapid progression (progressing within 4 months in this study), all with sarcomatoid differentiation. There were 94.7% patients that experienced at least one treatment related adverse event of any grade, with the most common (≥15%) treatment related adverse events being rash (28.9%), proteinuria (26.3%), hypertension (26.3%), hypothyroidism (21.1%), increased ALT or AST (21.1% each), fever (18.4%) and increased blood creatinine (15.8%):
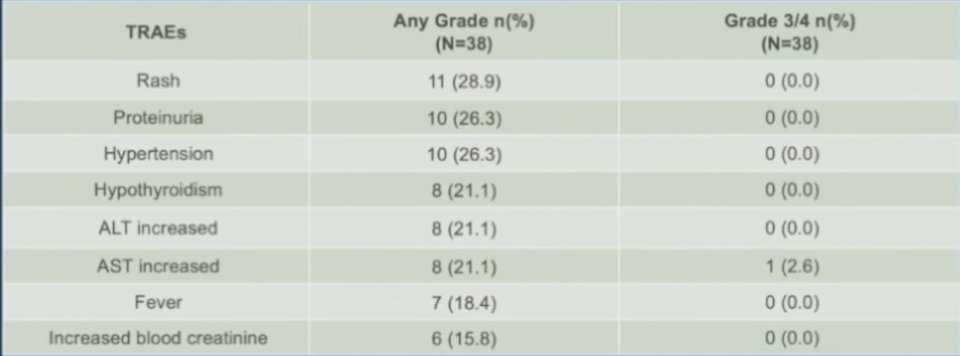
The majority of these events were grade 1 or 2, except for one patient who experienced a grade 3 increased AST. No serious adverse events or adverse events leading to permanent discontinuation of medication were observed during the study period, and no treatment related adverse events resulting in death were reported.
Dr. Huang noted several limitations for this trial:
- Immature data: for cancers like RCC that may progress slowly, longer follow-up is needed to obtain reliable survival data
- Lack of control group: a single arm study makes it difficult to determine the true effect of the intervention, and cannot rule out the influence of the natural disease course
- Insufficient biomarker data: There may be a lack of biomarker analysis that could predict treatment response
Dr. Huang concluded his presentation discussing fruquintinib + serplulimab as first line therapy in metastatic or unresectable non-clear cell RCC with the following take-home points:
- The combination of fruquintinib and serplulimab showed promising anti-tumor activity with acceptable tolerability as first-line treatment for metastatic or unresectable non-clear cell RCC
- This novel combination therapy has the potential to become a valuable therapeutic option for this challenging disease
Presented by: Jiwei Huang II, MD, RenJi Hospital, Shanghai Jiao Tong University, Shanghai, China
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026.