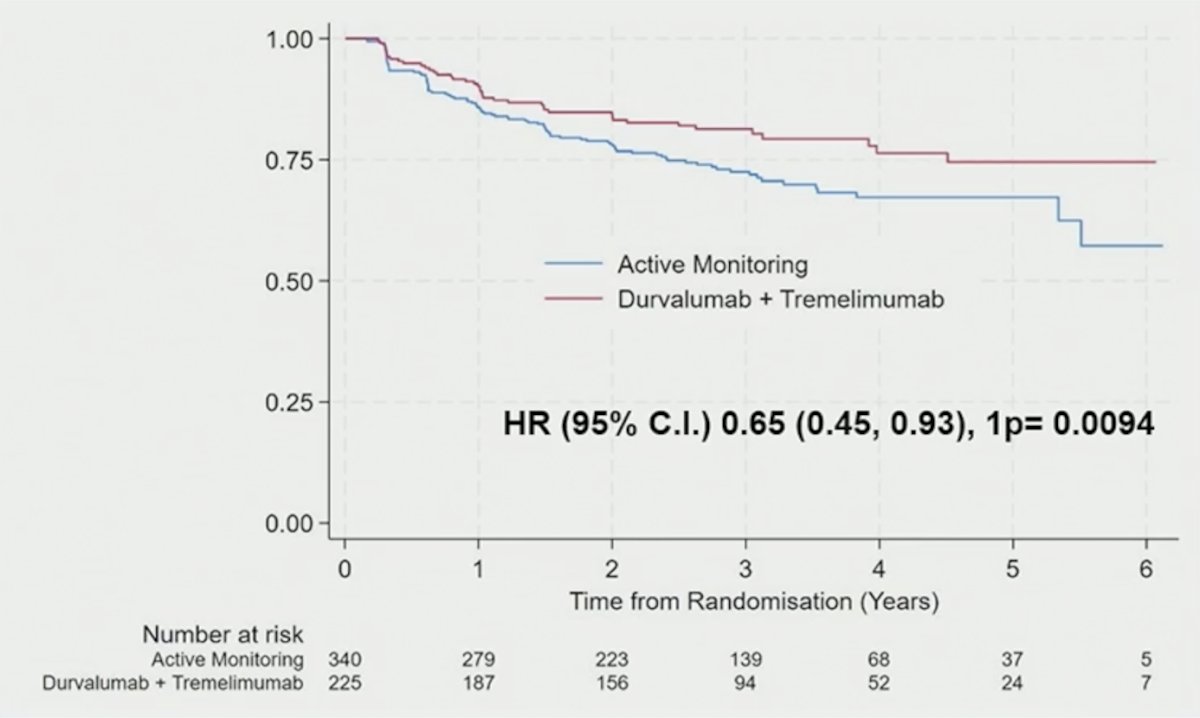
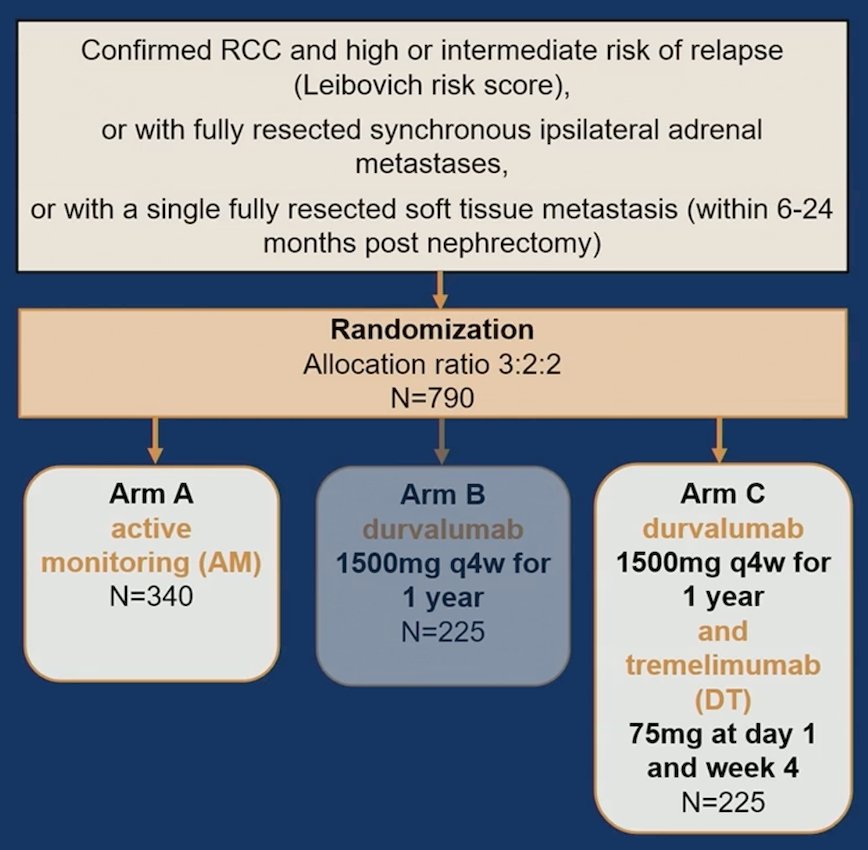
(UroToday.com) The 2026 GU ASCO annual meeting featured a kidney cancer session and a presentation by Dr. Sophie Merrick discussing patient reported outcomes in resected RCC from the RAMPART trial assessing active monitoring versus durvalumab + tremelimumab. Nephrectomy is the standard of care for locoregional RCC, but recurrence risk remains high. Adjuvant durvalumab + tremelimumab given over one year (with tremelimumab at Day 1 and Week 4), improved disease-free survival in patients with resected renal cell carcinoma at intermediate/high risk of relapse in the RAMPART trial:
Evaluating quality of life is key to understanding the overall impact of treatment. The primary quality of life outcome in RAMPART was the change in overall health and quality of life from baseline to 15 months, and no difference was observed between participants assigned durvalumab + tremelimumab versus active monitoring. At ASCO GU 2026, Dr. Merrick presented detailed quality of life outcomes from the comparison of durvalumab + tremelimumab versus active monitoring.
This analysis includes participants randomly assigned (3:2) to active monitoring or durvalumab + tremelimumab, who participated in the optional quality of life sub study and completed the EORTC QLQ-C30 at baseline plus ≥1 follow-up (week 16 or month 15):
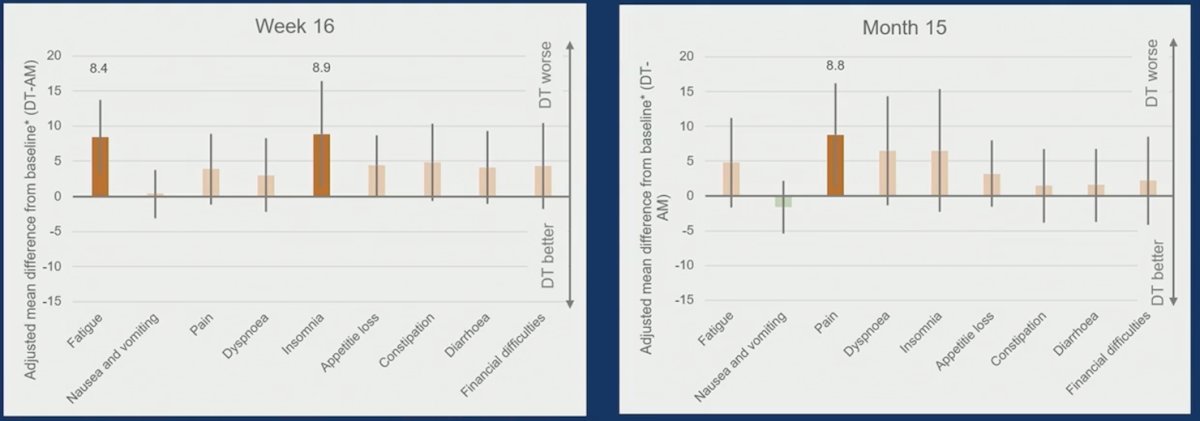
Outcomes assessed include overall health and quality of life (Q29–30) at week 16, five functional domains, eight symptom domains, and financial difficulties at both week 16 and month 15. Clinically meaningful differences were predefined by item and scale.
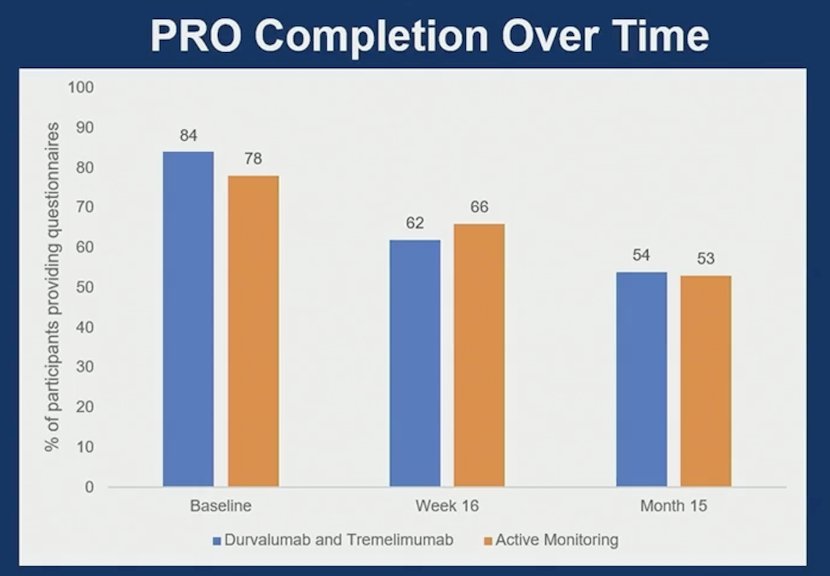
A total of 254 participants were included (150 active monitoring, 104 durvalumab + tremelimumab). Baseline characteristics were similar, with minor differences in sex distribution (male: 68% active monitoring versus 74% durvalumab + tremelimumab) and performance status (0: 80% active monitoring versus 88% durvalumab + tremelimumab; performance status 1: 20% active monitoring versus 12% durvalumab + tremelimumab). Moreover, completion rates over time were similar between arms A and C:
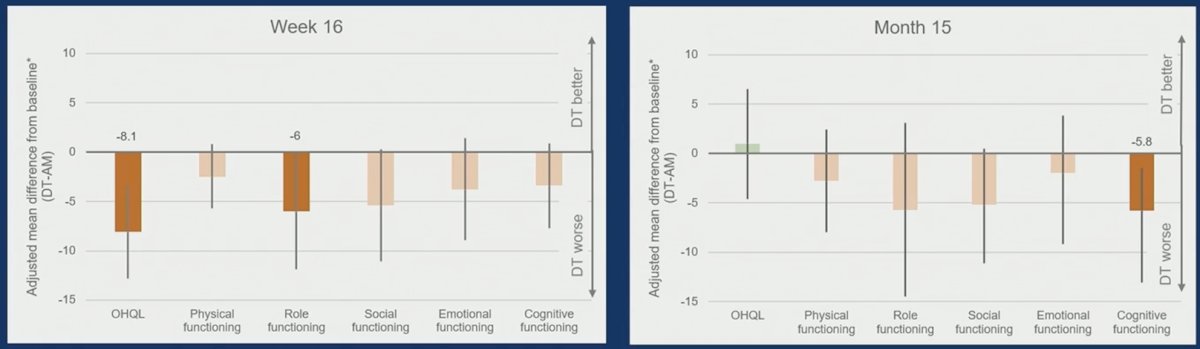
At week 16, scores were worse in those assigned durvalumab + tremelimumab rather than active monitoring for overall health and quality of life (–8.1; 95% CI –12.8 to –3.4; p = 0.0008), role function (–6.0; 95% CI –11.9 to –0.2; p = 0.04), fatigue (8.4; 95% CI 3.2 to 13.7; p = 0.002), and insomnia (8.9; 95% CI 1.3 to 16.4; p = 0.02). All exceeded the minimum threshold for a small clinically meaningful differences (overall health and quality of life 4–<10, role function 6–<19, fatigue 5–<13, insomnia 4–<13). By month 15, scores were worse in those assigned durvalumab + tremelimumab rather than active monitoring for pain (8.8; 95% CI 1.4 to 16.2; p = 0.02) and cognitive function (–5.8; 95% CI –11.5 to –0.2; p = 0.04), both exceeding the predefined thresholds for a small clinically meaningful differences (pain 6–<13, cognitive function 3–<9):
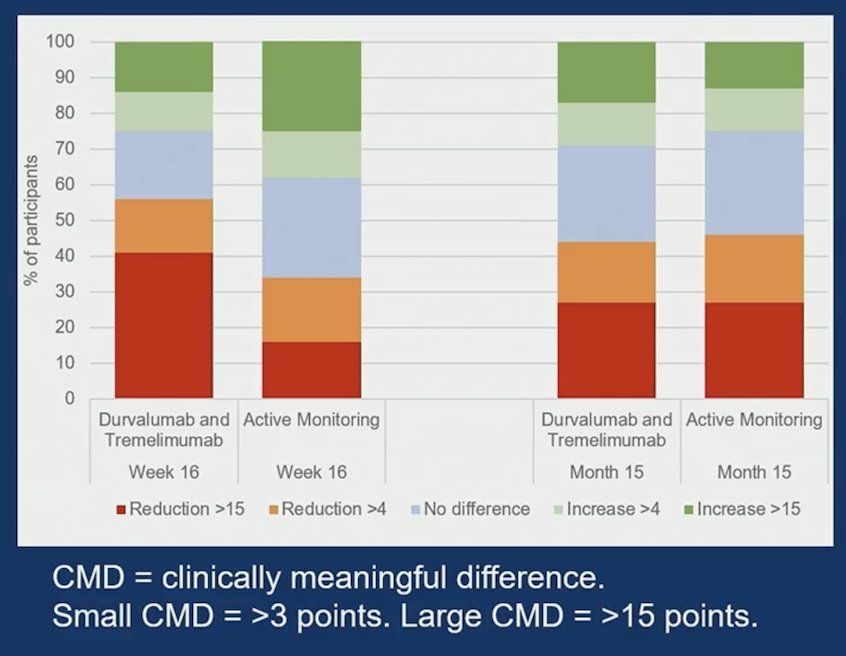
At week 16, a higher proportion of participants in the durvalumab + tremelimumab arm experienced a large clinically meaningful reduction in overall health quality of life (OR 3.7, 95% CI 1.9 – 7.1; p = 0.001), however at month 15, proportions were similar between treatment arms:
Dr. Merrick noted several limitations with this analysis:
- This was an open label trial, which may have influenced responses
- Analyses were conducted in the optional quality of life sub-study population who had completed QLQ-C30 questionnaires
- Analyses are exploratory, with no adjustment for multiple testing
Dr. Merrick concluded her presentation discussing patient reported outcomes in resected RCC from the RAMPART trial assessing active monitoring versus durvalumab and tremelimumab with the following take-home points:
- At week 16, durvalumab + tremelimumab was associated with worse quality of life, with clinically meaningful declines in overall health related quality of life, role functioning, fatigue and insomnia. These early effects appeared to improve by month 15
- At month 15, durvalumab + tremelimumab was associated with new clinically meaningful declines in pain and cognitive function
- These findings should be considered alongside the disease free survival benefit when interpreting the trial results
Presented by: Sophie Merrick, MBCHB, MRCP, MRC Clinical Trials Unit of UCL, London, UK
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026.
Related content: RAMPART Study Investigates Quality of Life Impact of Durvalumab and Tremelimumab in RCC - Sophie Merrick