(UroToday.com) The 2026 GU ASCO annual meeting featured a urothelial carcinoma session and a presentation by Dr. Jan-Jaap Mellema discussing results from the phase 2 Indi-Blade trial assessing induction ipilimumab + nivolumab followed by consolidating chemoradiotherapy as bladder-sparing treatment in stage II/III urothelial carcinoma of the bladder.
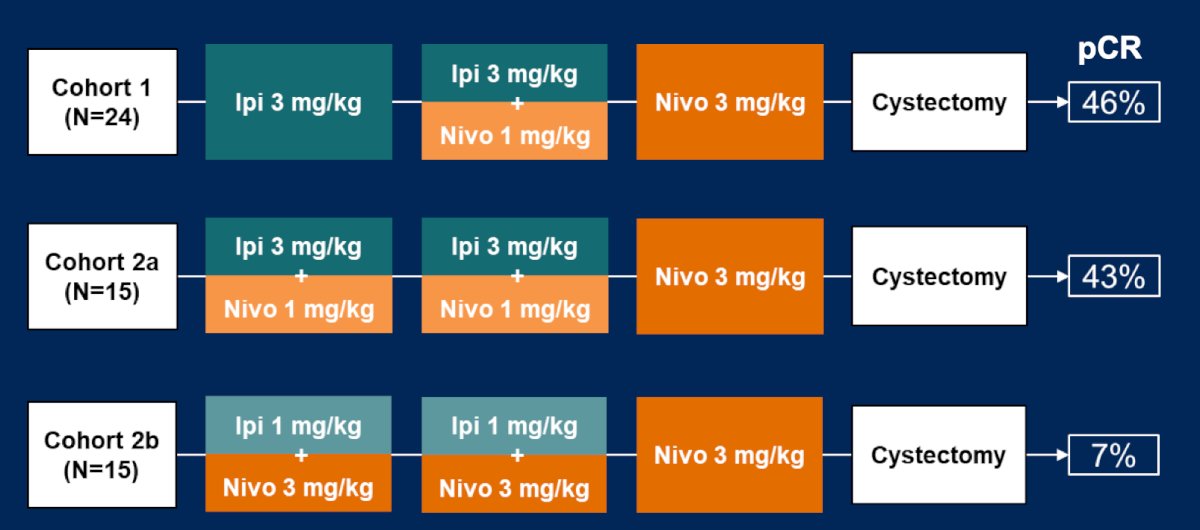
Radical cystectomy remains the most commonly used curative treatment for muscle-invasive bladder cancer, as bladder-sparing options are typically for patients with limited tumors or those unfit for cystectomy. Effective systemic induction therapy could broaden the population eligible for bladder-sparing treatment. The NABUCCO trial1 showed promising pathological complete responses (43-46%) and a 5-year overall survival of 70% using neoadjuvant ipilimumab + nivolumab in stage III muscle-invasive bladder cancer patients:
Dr. Mellema and colleagues hypothesized that induction of immune checkpoint inhibition followed by chemoradiotherapy is an effective bladder-sparing approach in muscle-invasive bladder cancer patients.
Indi-Blade is a multicenter, single-arm, phase-II trial, enrolling cT2-4aN0-2 muscle-invasive bladder cancer patients. Treatment consists of ipilimumab 3 mg/kg (day 1), ipilimumab 3 mg/kg + nivolumab 1 mg/kg (day 22) and nivolumab 3 mg/kg (day 43), followed by standard of care chemoradiotherapy using mitomycin C and fluoropyrimidines, 5FU or capecitabine:
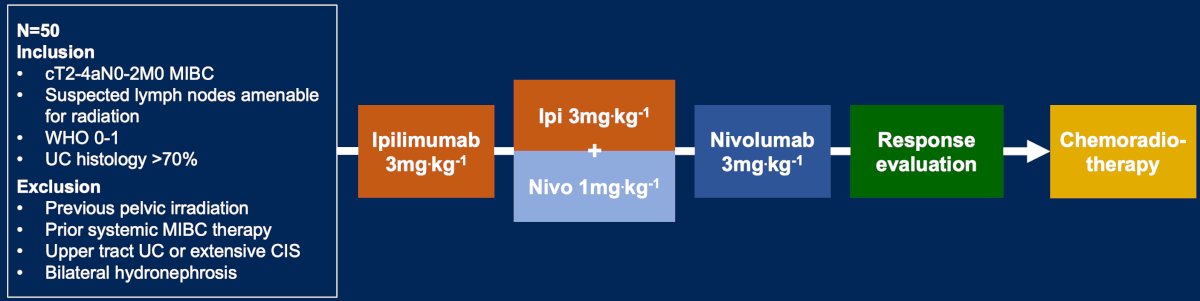
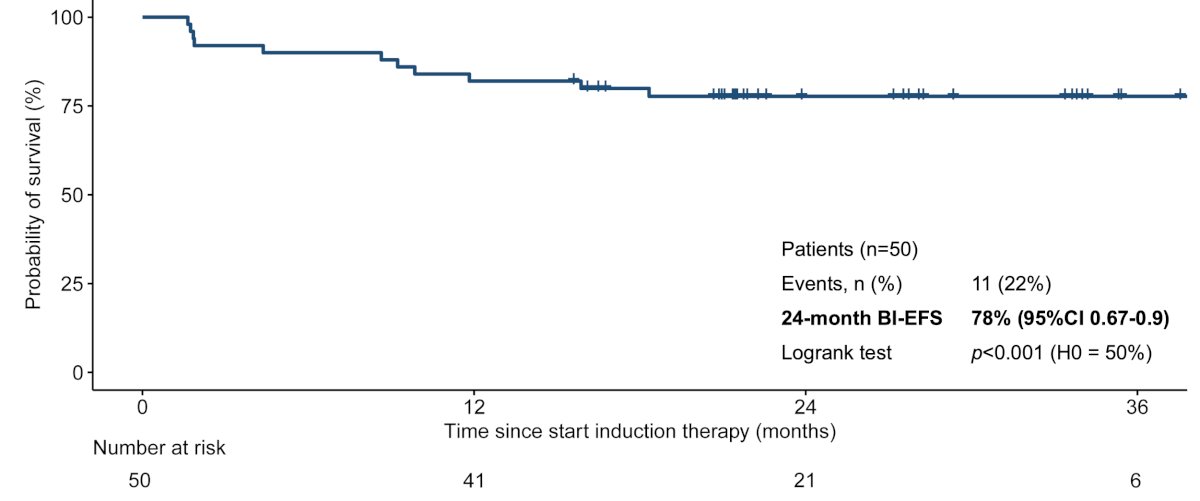
The primary endpoint is two-year bladder intact event free survival, estimated by Kaplan-Meier analysis. Events are defined as muscle-invasive, nodal or distant recurrence, cystectomy, switch to chemotherapy, or death by any cause. With a two-sided alpha of 0.05, a sample size of n = 50 has 81.3% power to exclude an estimated bladder intact event-free survival of 50% (median 24 months), with a target two-year bladder intact event-free survival of 70% (median 46.6 months). Secondary endpoints include overall survival, toxicity, and ctDNA analysis.
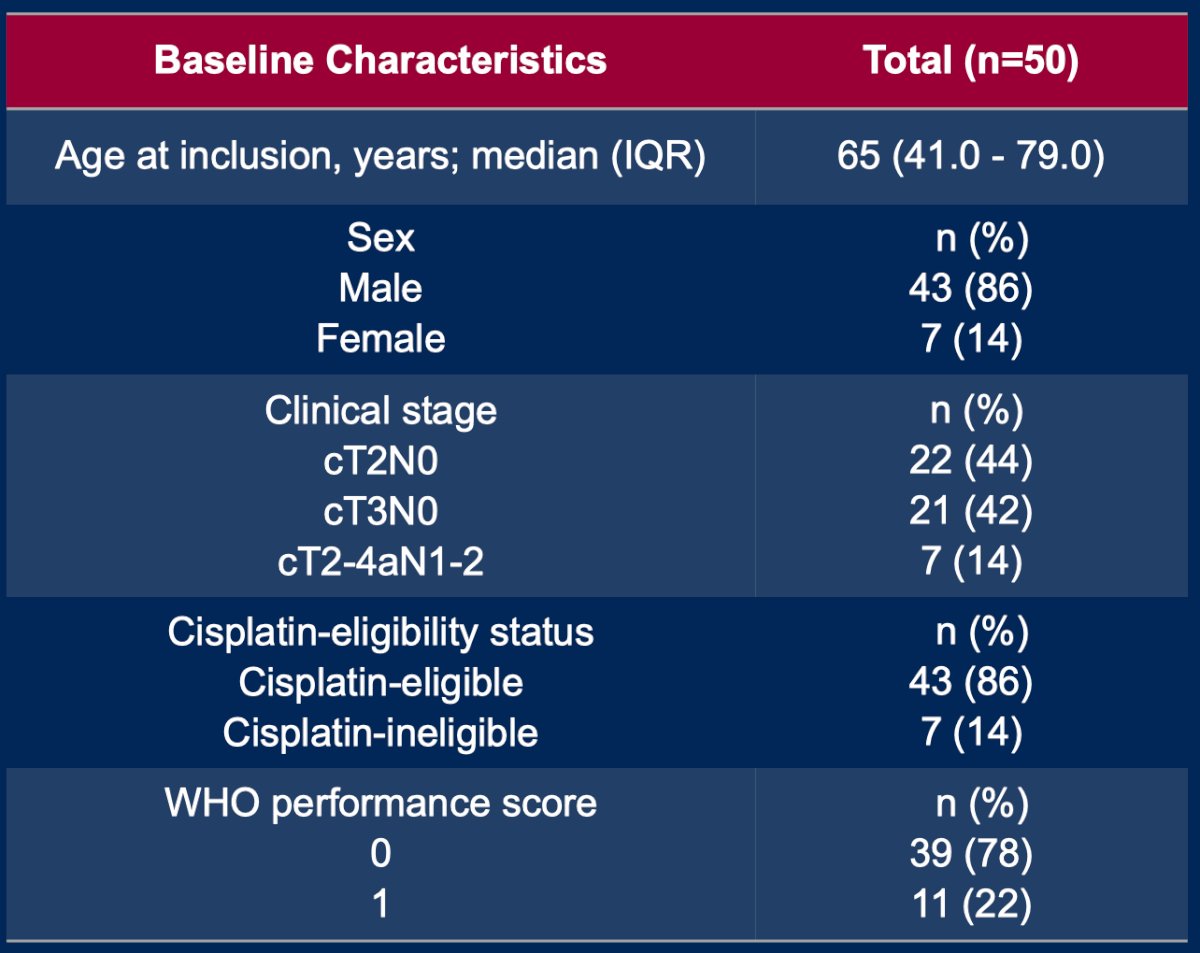
There were 50 patients enrolled between February 2022 and February 2024. Patients had cT2N0 (22; 44%), cT3N0 (21; 42%), and cN+ (7; 14%) muscle-invasive bladder cancer. Overall, 45/50 patients (90%) proceeded to chemoradiotherapy following induction immune checkpoint inhibition:
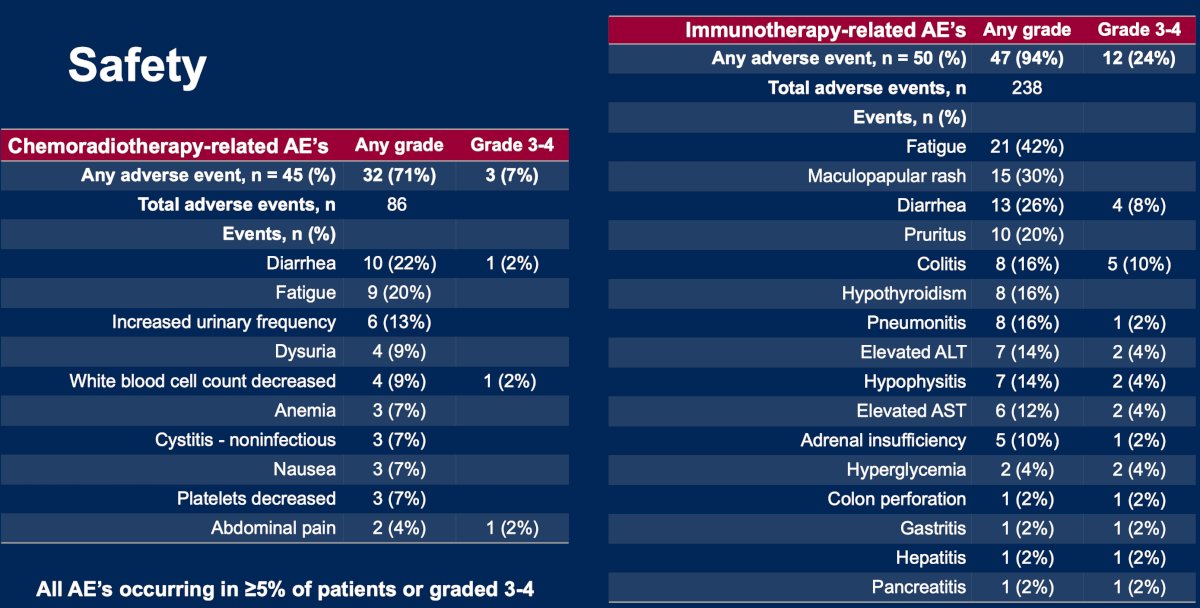
Grade ≥3 immunotherapy-related adverse events occurred in 24% of patients, and grade ≥3 chemoradiotherapy-related adverse events occurred in 7% of patients:
After a median follow-up (data cutoff October 3, 2025) of 28.7 months (IQR 22.6 – 34.7), the primary endpoint of estimated two-year bladder intact event-free survival was met at 78% (95% CI 0.67-0.90; p < 0.001):
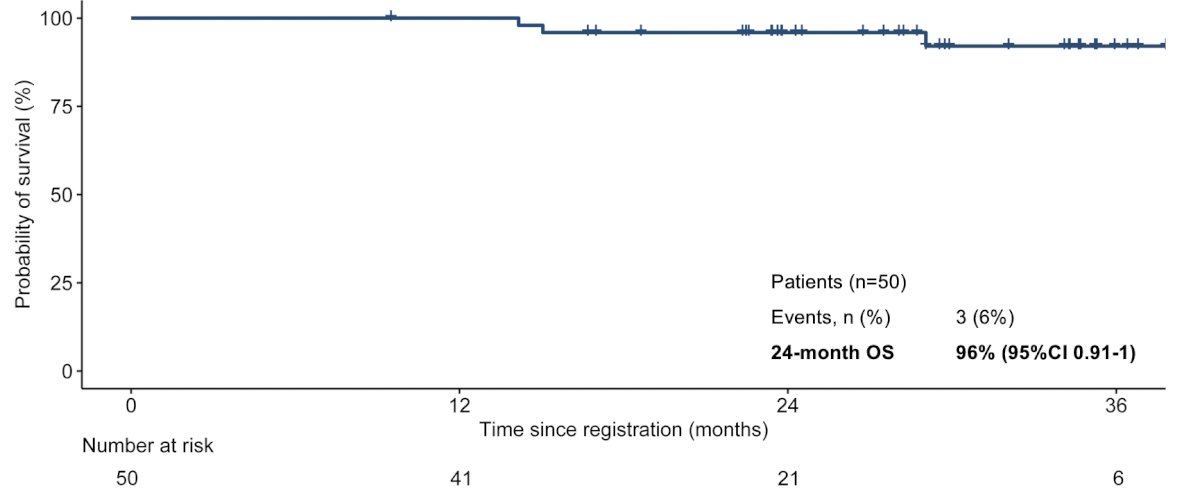
The estimated two-year overall survival was 96% (95% CI 0.9-1.0):
ctDNA positive status was associated with shorter bladder intact event-free survival compared to ctDNA negatives at both baseline (HR 3.59, 95% CI 0.86-15.02; p = 0.08) and after induction of immune checkpoint inhibition (HR 8.33, 95% CI 1.38-50.36; p = 0.02):
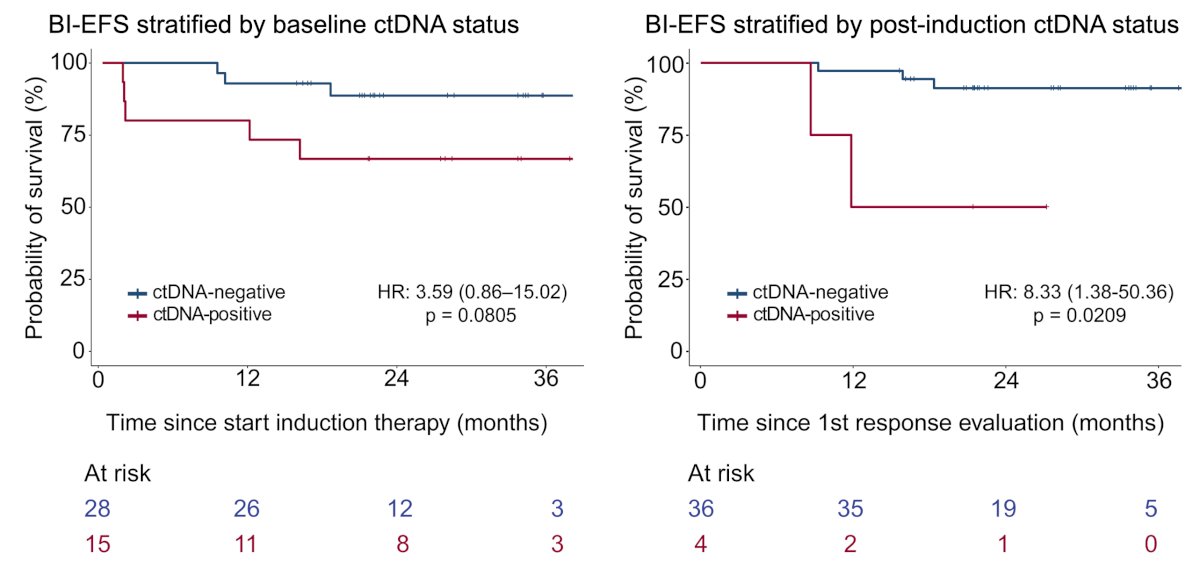
Patients who were ctDNA negative at baseline or post-immune checkpoint inhibition had an 88.6% and 88.4% two-year bladder intact event-free survival, respectively. ctDNA clearance in baseline ctDNA-positive patients occurred in 76.9% (10/13 evaluable patients) post-immune checkpoint inhibition and 91.7% (11/12) post-chemoradiotherapy.
Dr. Mellema concluded this presentation discussing results from the phase 2 Indi-Blade trial with the following take-home points:
- Potent induction combination immune checkpoint inhibition followed by chemoradiotherapy is an effective, bladder-sparing treatment for a broad population of muscle-invasive bladder cancer patients
- Estimated two-year bladder intact event free survival was 78%
- Estimated two-year overall survival was 96%
- No new safety signals were observed
- Absence of ctDNA post-immunotherapy was associated with bladder intact event-free survival (HR 8.3; p = 0.02) and could aid clinical decision-making after systemic induction
Following Dr. Mellema’s presentation, this paper was concomitantly published in Nature Medicine.
Presented by: Jan-Jaap Mellema, Netherlands Cancer Institute, Amsterdam, Netherlands
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 26 – Sat, Feb 28, 2026.
Related content: Indi-Blade Study Tests Ipilimumab-Nivolumab Followed by Chemoradiotherapy in Advanced Bladder Cancer - Michiel Van Der Heijden & Jan-Jaap Mellema
Reference:
- van Dijk N, Gil-Jimenez A, Silina K, et al. Preoperative ipilimumab plus nivolumab in locoregionally advanced urothelial cancer: the NABUCCO trial. Nat Med. 2020 Dec;26(12):1839-1844.