(UroToday.com) The 2026 GU ASCO annual meeting featured a urothelial carcinoma session and a discussant presentation by Dr. Tyler F. Stewart, discussing two abstracts: “Neoadjuvant and adjuvant EV + pembrolizumab for participants with MIBC who are eligible for cisplatin: Randomized, open-label, phase 3 KEYNOTE-B15 study” by Dr. Matthew Galsky and “RC48G001: A phase 2 study of disitamab vedotin in HER2-expressing previously treated advanced urothelial carcinoma” by Dr. Thomas Powles. Dr. Stewart started his discussant presentation by highlighting the KEYNOTE-B15 trial, noting that before this trial, we generally decided if a patient with muscle invasive bladder cancer was a radical cystectomy candidate or better served with bladder preservation. In patients fit for cystectomy, the next decision was whether they were cisplatin eligible or ineligible. If cisplatin eligible, they would be considered for cisplatin-based chemotherapy with immunotherapy or cisplatin based chemotherapy with consideration of adjuvant immunotherapy. If cisplatin ineligible, there may be a consideration for adjuvant immunotherapy based on risk of recurrence or, more recently, based on post-operative ctDNA.
At ESMO 2025, we saw the results of KEYNOTE-905/EV-303, a large phase III study investigating the addition of perioperative enfortumab vedotin + pembrolizumab in patients with muscle invasive bladder cancer who are cisplatin-ineligible. This study demonstrated a marked improvement in both event free survival and overall survival, with impressive pathological complete response rates, subsequently cementing enfortumab vedotin + pembrolizumab as standard of care for patients with muscle invasive bladder cancer planning for radical cystectomy who are cisplatin-ineligible. At ASCO GU 2026, we see the results of KEYNOTE-B15, which tested the combination of enfortumab vedotin + pembrolizumab versus cisplatin + gemcitabine in patients who are cisplatin-eligible:

When KEYNOTE-B15 was designed, cisplatin + gemcitabine was a standard of care, which is the comparator arm for the trial, with no obligation for adjuvant immunotherapy (allowed post-2023). Importantly, this includes 3 months of cisplatin + gemcitabine versus over 6 months of enfortumab vedotin and a year of pembrolizumab. Dr. Stewart notes that it was not long ago when there were discussions about 4 cycles of cisplatin + gemcitabine versus 6 cycles of dose dense MVAC, and now we are discussing 3 months versus 6 months of cytotoxic agents. The primary endpoint in KEYNOTE-B15 is event free survival, which Dr. Stewart emphasizes should be somewhat concerning given that this is a healthy population with curative intent, and historically, we would aim for overall survival to be the primary endpoint in a perioperative study. However, overall survival was a key secondary endpoint.
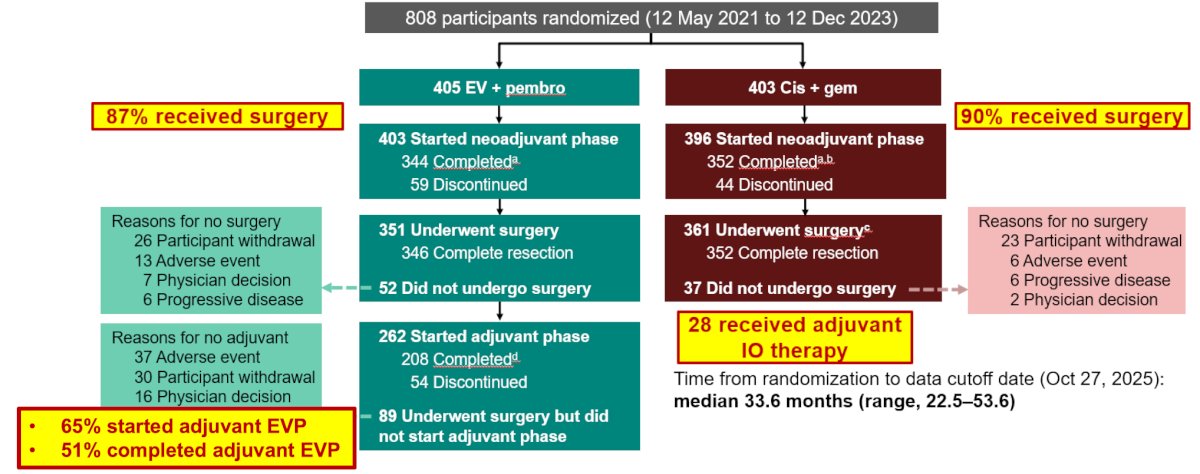
Overall, 87% of patients who received enfortumab vedotin + pembrolizumab and 90% of patients with cisplatin + gemcitabine underwent surgery. Of note, 65% of patients in the enfortumab vedotin + pembrolizumab arm underwent adjuvant (75% of those who received surgery) enfortumab vedotin + pembrolizumab, with 51% completing adjuvant treatment. In the cisplatin + gemcitabine arm, only 28 patients received adjuvant immunotherapy:
The study met its primary endpoint of improving event free survival, with a median not reached (95% CI not reached to not reached) for enfortumab vedotin + pembrolizumab and 48.5 months (95% 43.3 to not reached) for cisplatin + gemcitabine (HR 0.53, 95% CI 0.41-0.70; p < 0.0001). The 12 month event free survival rate for enfortumab vedotin + pembrolizumab was 86.0% versus 75.4% for cisplatin + gemcitabine, and the 24 month rate was 79.4% for enfortumab vedotin + pembrolizumab versus 66.2% for cisplatin + gemcitabine. The median overall survival was not reached in either arm, with the hazard ratio favoring enfortumab vedotin + pembrolizumab: HR 0.65, 95% CI 0.48-0.89; p = 0.0029. The 12 month overall survival rate was 93.1% for enfortumab vedotin + pembrolizumab versus 89.6% for cisplatin + gemcitabine, with a 24 month rate of 86.9% and 81.3%, respectively:
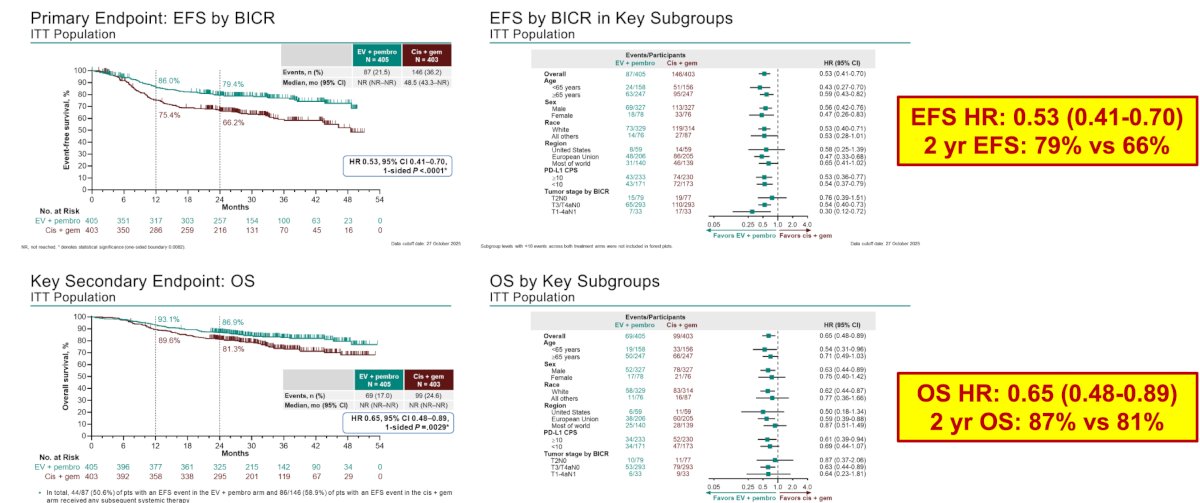
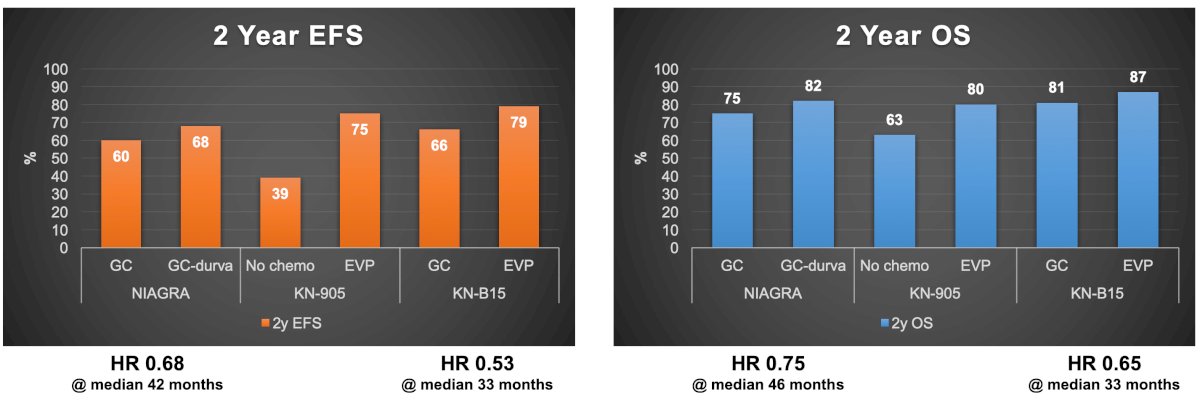
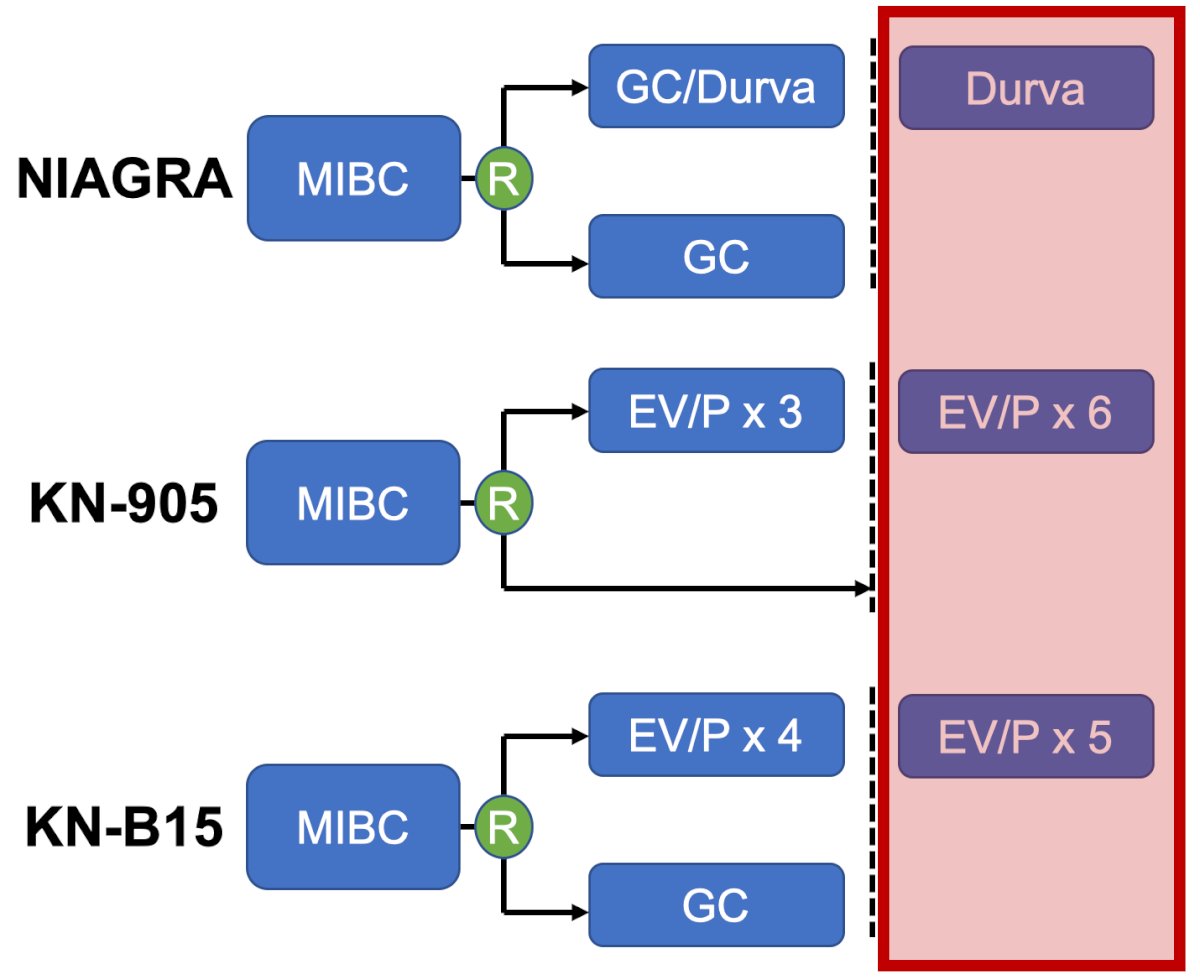
Dr. Stewart notes that when looking at the event free survival Kaplan Meier curve, there appears to be a flattening of the curve, suggesting that perhaps we are curing many of these patients. How do these results compare to other trials? Numerically, the 2 year event free survival and overall survival outcomes are better in KEYNOTE-B15 compared to NIAGARA1 and KEYNOTE-905:
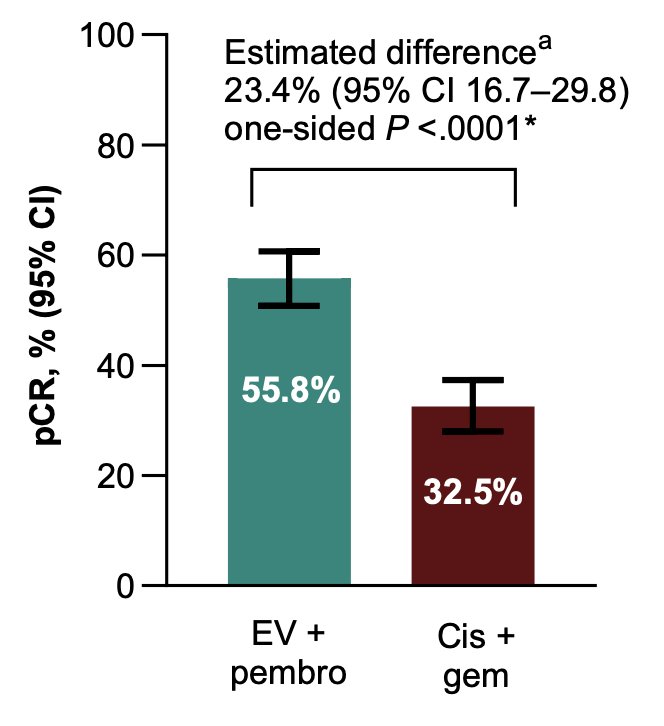
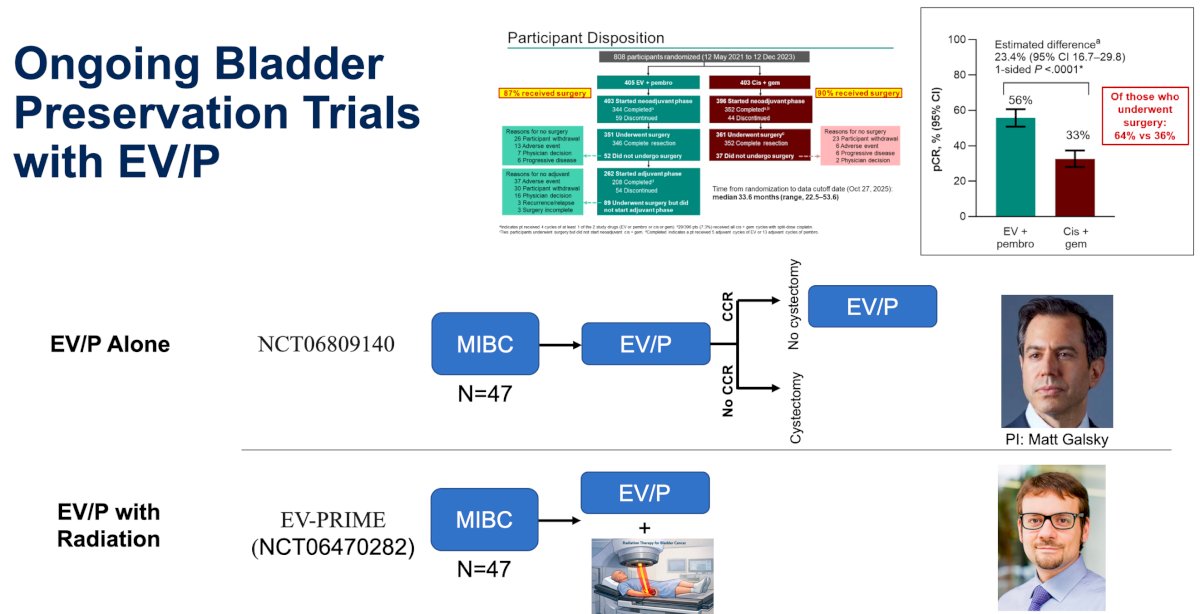
In KEYNOTE-B15, the pathological complete response rate for enfortumab vedotin + pembrolizumab was 55.8% versus 32.5% for cisplatin + gemcitabine, with an estimated difference of 23.4% (95% CI 16.7 – 29.8; p < 0.001), which Dr. Stewart emphasized is one of the best pathologic complete responses we have seen in perioperative trials:
Based on these results from KEYNOTE-B15, enfortumab vedotin + pembrolizumab should be a treatment option for patients with muscle invasive bladder cancer. However, there are some major questions that have been left unanswered:
- Does everyone need systemic therapy?
- Do we have the length of therapy correct?
- How can we use this data to improve bladder preservation?
What is not answered by NIAGARA, KEYNOTE-905, or KEYNOTE-B15 is whether the adjuvant portion of perioperative treatment is necessary:
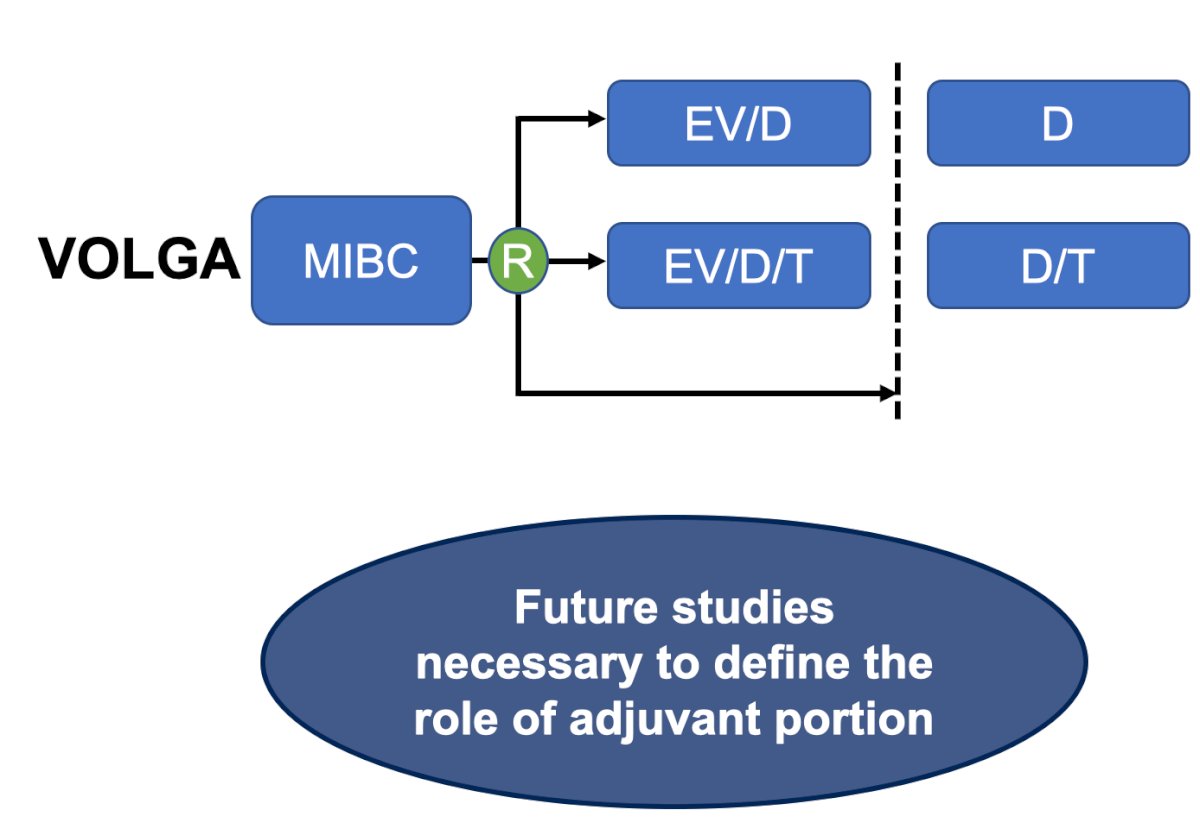
However, the VOLGA trial may give us some insights into the importance of adjuvant therapy. This trial is investigating enfortumab vedotin + pembrolizumab + durvalumab versus enfortumab vedotin + pembrolizumab + durvalumab + tremelimumab in a cisplatin-ineligible cohort, with no enfortumab vedotin + pembrolizumab for either arm in the adjuvant setting. Thus, we may gain insight into the importance (or lack thereof) of adjuvant enfortumab vedotin + pembrolizumab:
Dr. Steward emphasized that the future of bladder cancer is curing patients, while preserving the bladder when appropriate. With pathologic complete response rates of 55-60%, patients and physicians are right to wonder whether radical cystectomy can safely be avoided. There are studies already ongoing and being designed, and until these studies read out, we will be in the Wild West:
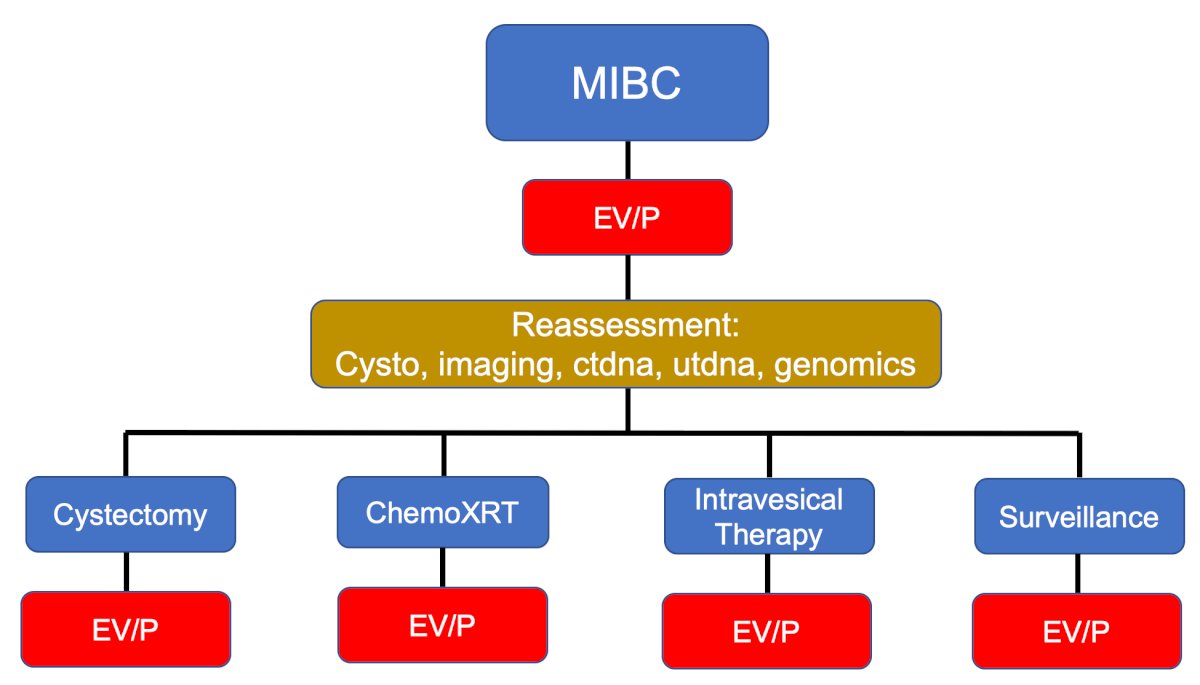
Perhaps, the future of muscle invasive bladder cancer will look like the following algorithm provided by Dr. Stewart:
To conclude his discussion of KEYNOTE-B15, Dr. Stewart asks: Is enfortumab vedotin + pembrolizumab for everyone?
- In a worldwide context, there will be accessibility and cost considerations
- What do we do with histologic variants?
- What happens if patients progress shortly after enfortumab vedotin + pembrolizumab?
- Enfortumab vedotin + pembrolizumab is the new starting point, but it is not the end
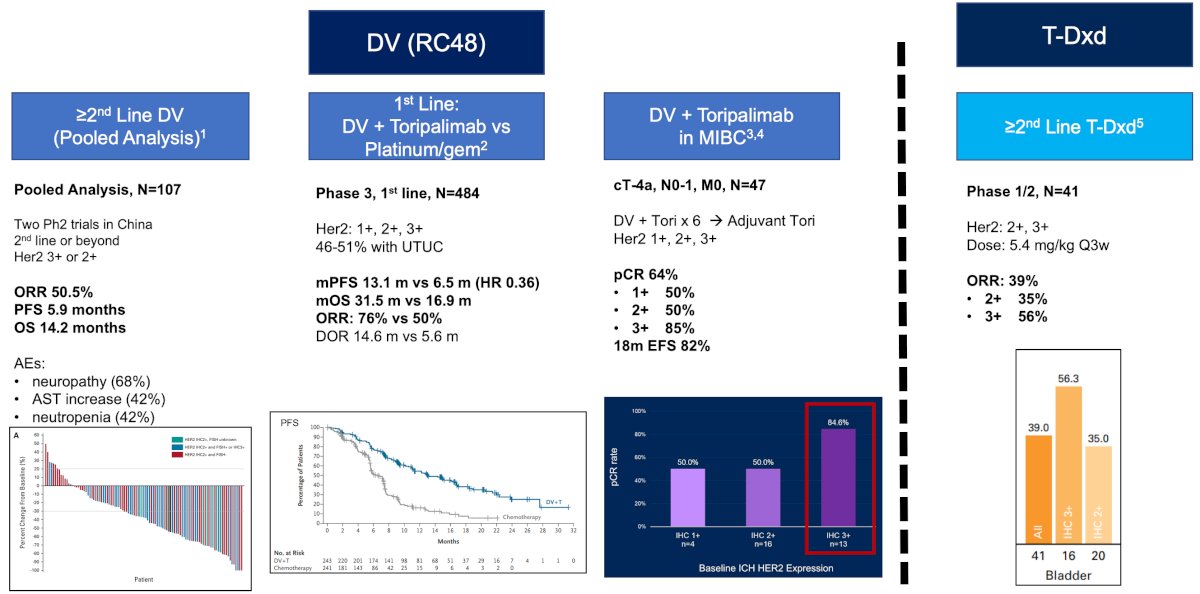
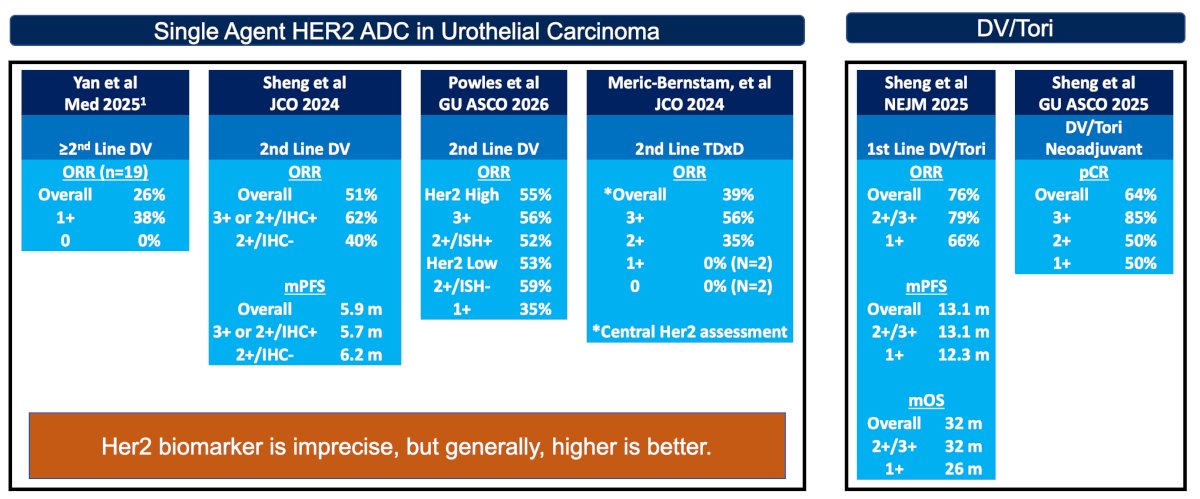
Dr. Stewart then transitioned to discuss the RC48G001 trial. Disitamab vedotin is an antibody drug conjugate that targets HER2 with MMAE payload, and in this context, in the US, trastuzumab deruxtecan is an agent that is currently approved for treatment of HER2-positive (IHC3+) solid tumors that have received prior systemic treatment and have no satisfactory alternative treatment options. Before RC48G001, we have already seen data from China for disitamab vedotin in treatment refractory urothelial carcinoma, front line urothelial carcinoma, and in the muscle invasive bladder cancer setting. Disitamab vedotin had a 50% response rate for HER2+ patients in the treatment refractory setting, and recent data reported for disitamab vedotin + toripalimab in the front line setting showed superior outcomes compared to platinum based chemotherapy [2]:
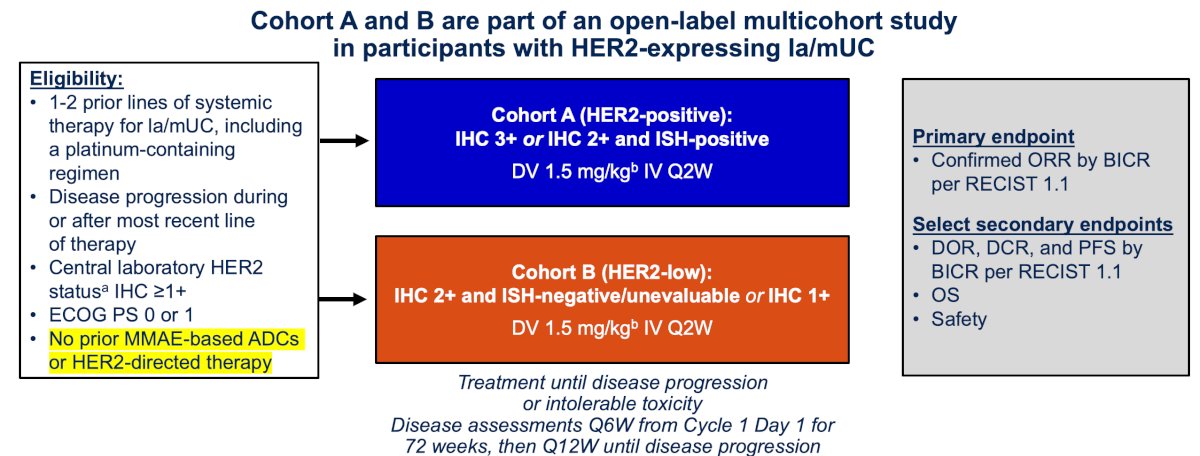
RC48G001 is a global, multicohort, single-arm, open-label, phase 2 study that enrolled patients with locally advanced or metastatic urothelial carcinoma who received 1-2 prior systemic therapies (including a platinum-containing regimen) and exhibited HER2 expression. The two cohorts were as follows:
- Cohort A: HER2-positive locally advanced or metastatic urothelial carcinoma, defined as IHC 3+, or IHC 2+/ISH-positive
- Cohort B: HER2-low locally advanced or metastatic urothelial carcinoma, defined as IHC 2+/ISH-negative or unevaluable, or IHC 1+
Patients received 1.5 mg/kg disitamab vedotin monotherapy IV once per 2-week cycle:
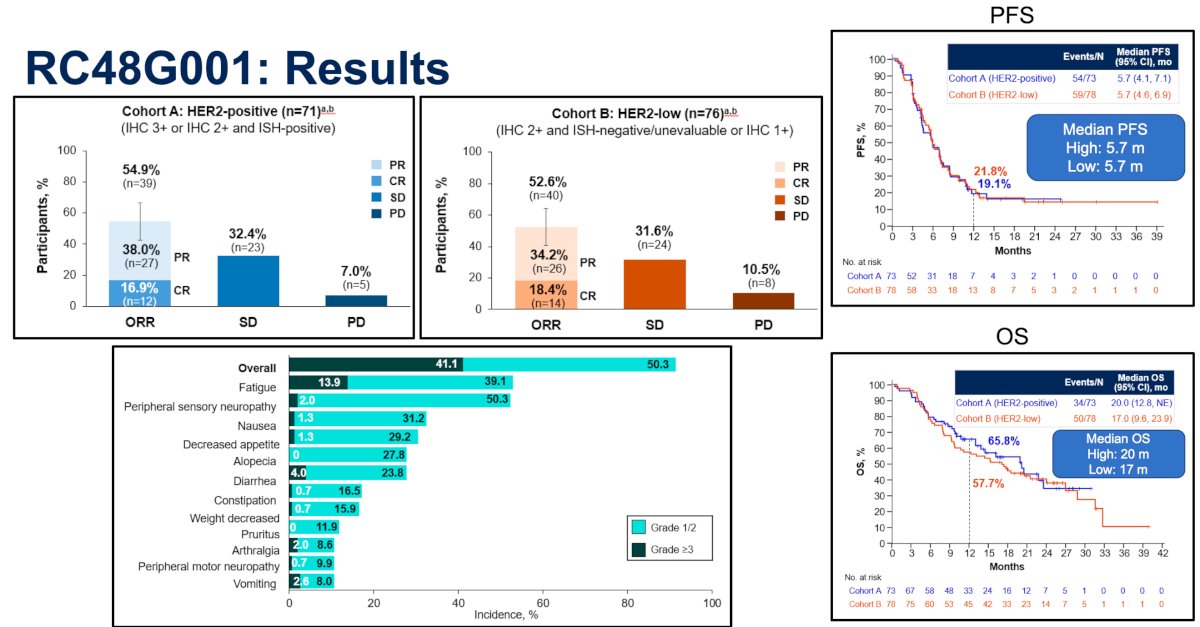
Importantly, prior enfortumab vedotin was not allowed in this study; thus, how these results will be relevant in the post-enfortumab vedotin + pembrolizumab era remains to be determined. The results from RC48G001 are important, as highlighted by Dr. Stewart. Confirmed objective response rate per blinded independent central review was 54.9%, with a complete response rate of 16.9%, in Cohort A, and 52.6%, with a complete response rate of 18.4%, in Cohort B. The median progression free survival by blinded independent central review was 5.7 months in both cohorts, and the median overall survival was 20.0 months and 17.0 months in Cohort A and B, respectively. Grade ≥3 treatment related adverse events occurred in 62 (41.1%) patients, with fatigue (13.9%) being the most common:
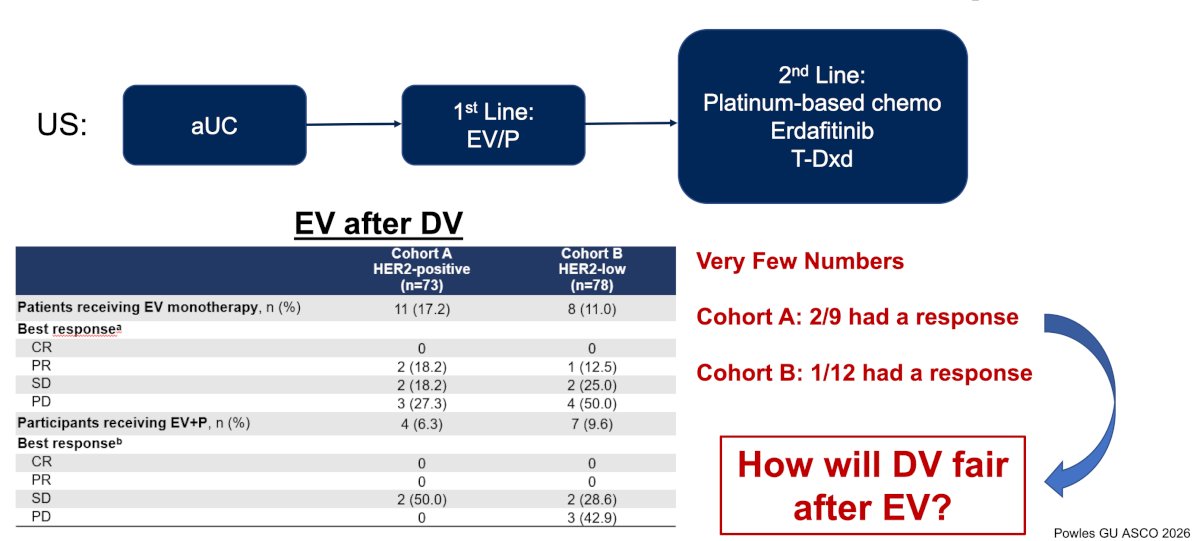
Where does disitamab vedotin fit into the current landscape? To date, we have very little data to guide treatment with an ADC after an ADC failure:
With regards to biomarkers, Dr. Stewart notes that because HER2 in RC48G001 had comparable objective response rates (54.9% versus 52.6%) regardless of expression, it may not be an ideal biomarker. However, across trials, the lower the HER2 IHC biomarker, generally, there is poorer response:
Dr. Stewart concluded his discussant presentation with the following take-home points:
- Enfortumab vedotin + pembrolizumab demonstrated superior event free survival, overall survival, and an impressive pathological complete response rate compared to cisplatin + gemcitabine
- This will be Dr. Stewart’s new standard regimen for all patients with muscle invasive bladder cancer
- Disitamab vedotin appears to be an effective regimen for advanced urothelial carcinoma; however:
- It is unknown how effective this drug will be after enfortumab vedotin
- Clarity around the biomarker is still needed
Presented by: Tyler F. Stewart, MD, Moores Cancer Center, University of San Diego, La Jolla, CA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 26 – Sat, Feb 28, 2026.
References:
- Powles T, Catto JWF, Galsky MD, et al. Perioperative Durvalumab with Neoadjuvant Chemotherapy in Operable Bladder Cancer. N Engl J Med. 2024 Nov 14;391(1):1773-1786.
- Sheng X, Zeng G, Zhang C, et al. Disitamab Vedotin plus Toripalimab in HER2-Expressing Advanced Urothelial Cancer. N Engl J Med. 2025 Dec 11;393(23):2324-2337.