(UroToday.com) The 2026 GU ASCO annual meeting featured a urothelial carcinoma session and a presentation by Dr. Michael Basin discussing the detection of FGFR3 genomic alterations in liquid biopsies from patients with clinically advanced urothelial bladder cancer. FGFR3 pathogenic gain-of-function genomic alterations, including activating short variant mutations, rearrangements/fusions, and amplifications (FGFR2/FGFR3 mutation positive), are associated with the development and progression of urothelial bladder cancer and have emerged as major therapy targets for patients with clinically advanced urothelial bladder cancer.
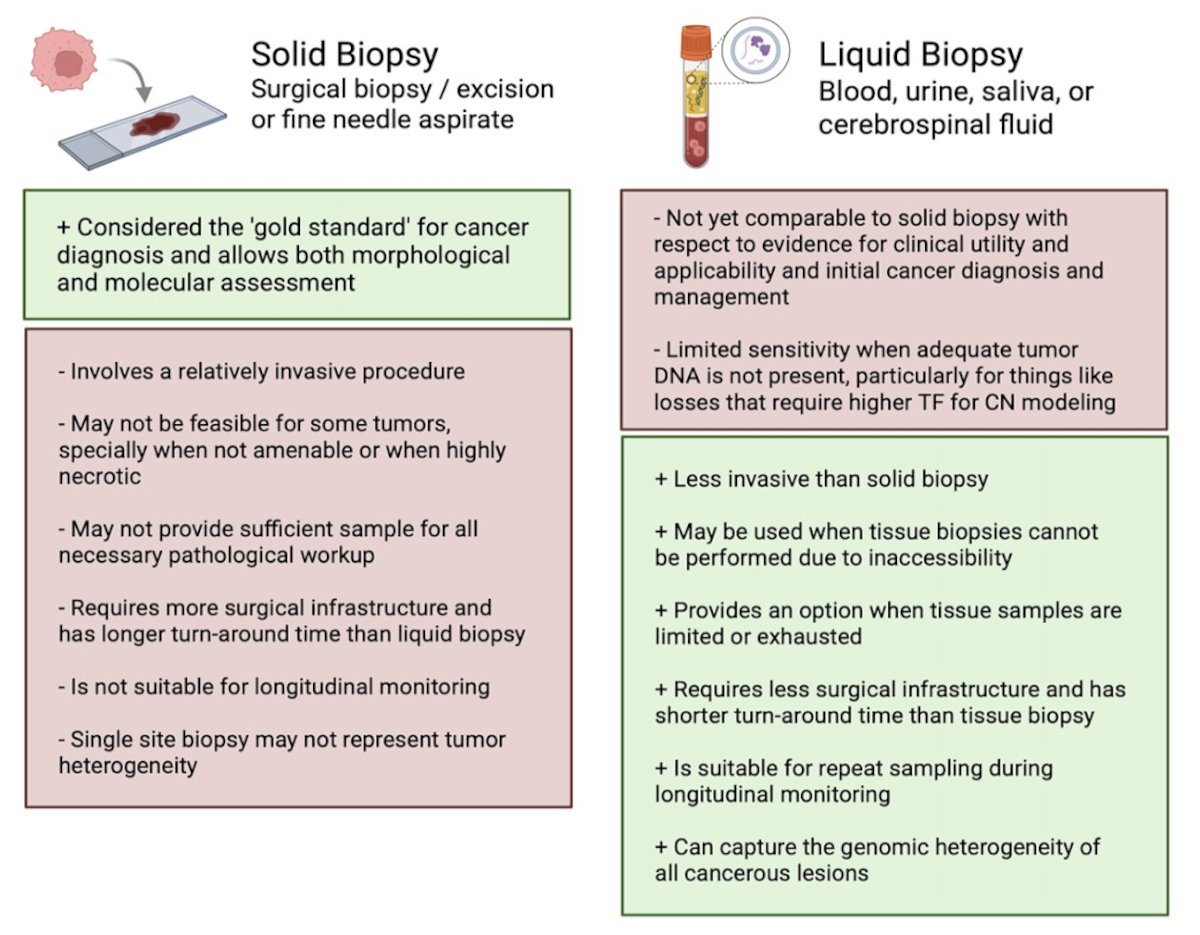
Erdafitinib is an FDA-approved pan–FGFR inhibitor for metastatic urothelial carcinoma harboring susceptible alterations in FGFR2/FGFR3, such as activating mutations or fusion. Conventional genomic testing for FGFR3 typically involves tumor tissue; ctDNA can be a relevant biospecimen for such testing. For this study, Dr. Basin and colleagues queried whether the tumor fraction calculation would impact the ability of FGFR3 genomic alterations to be detected on liquid biopsies.
Hybrid capture-based comprehensive genomic profiling was performed on 10,531 clinically advanced urothelial bladder cancer tissue biopsies using the FoundationOne CDx assay and on 1,637 clinically advanced urothelial bladder cancer liquid biopsies using the FoundationOneLiquid CDx assay. The ctDNA tumor fraction for each liquid biopsy sample was determined using assessments of aneuploidy and variant allele frequencies, as previously described:
For the tissue biopsy group, 1,917 (18.2%) clinically advanced urothelial bladder cancer cases were FGFR3 mutation positive. For the liquid biopsies group, FGFR3 mutation positive detection was increased as the tumor fraction increased, reaching a plateau of 24-25% when the tumor fraction was ≥10%:
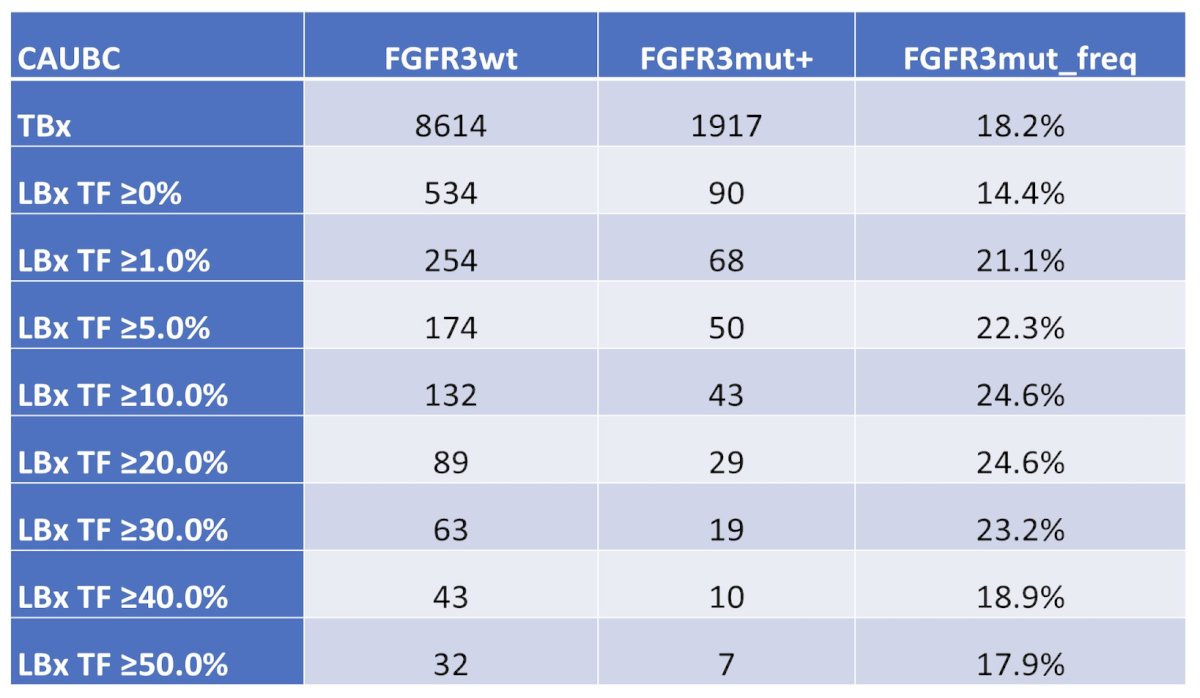
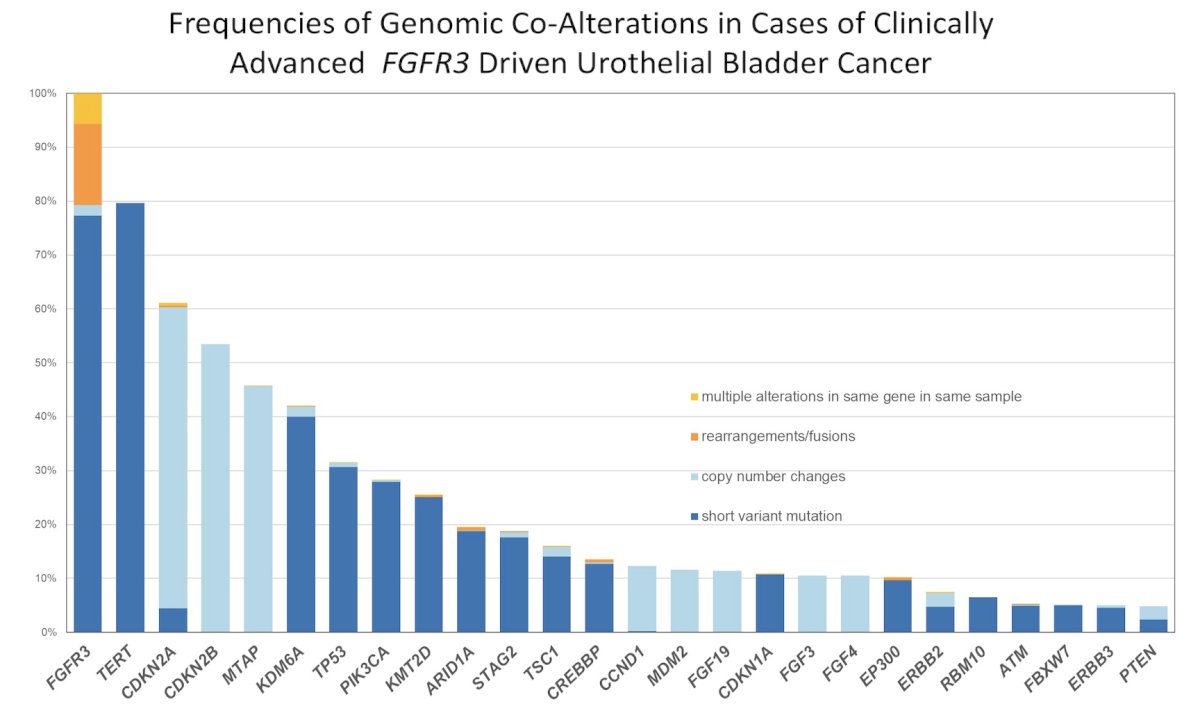
Detection rate at higher tumor fractions actually exceeded the tissue biopsy rate (ie. 24.6% versus 18.2%), indicating that liquid biopsy has the ability to capture tumor heterogeneity across multiple metastatic sites that a single biopsy may miss. The lower detection at tumor fraction <1% (14.4%) compared to tissue (18.2%) suggests that approximately 20-25% of FGFR3 mutation cases may be missed when tumor fraction is low. The majority of FGFR3 alterations were short variant mutations, followed by copy number changes, rearrangements/fusions, and cases with multiple alterations in the same gene. The most common co-occurring alterations included TP53, CDKN2A/B, KMT2D, PIK3CA, ARID1A, and TERT promoter mutations, consistent with the known genomic landscape of advanced bladder urothelial carcinoma:
Dr. Basin concluded his presentation discussing the detection of FGFR3 genomic alterations in liquid biopsies from patients with clinically advanced urothelial bladder cancer with the following take-home points:
- Liquid biopsies emerged as a sensitive method for detecting FGFR3 mutation positive in clinically advanced urothelial bladder cancer, but their sensitivity is dependent on tumor fraction
- Importantly, liquid biopsy tumor fraction may play a major role in comprehensive genomic profiling evaluation, as FGFR3 mutation positive rates using liquid biopsies appear to be as frequently detected in liquid biopsies as in tissue biopsy samples, especially when the liquid biopsy tumor fraction is ≥1%
- However, when tumor fraction levels are < 1%, the FGFR3 mutation-positive status may be missed, FGFR3 testing cannot rely on liquid biopsies in such cases
- Limitations include the retrospective nature, lack of clinical data annotation, possible selection, confounding biases, and lack of matched tissue biopsy and liquid biopsy samples
- These findings have the potential to increase liquid biopsy testing, especially in cases with insufficient tumor tissue available for comprehensive genomic profiling, and raise the question of whether liquid biopsies may be complementary to tissue biopsy
Presented by: Michael Basin, MD, Upstate Medical University, Syracuse, NY