(UroToday.com) The 2026 GU ASCO annual meeting featured a urothelial carcinoma session and a presentation by Andrew J. Murtha discussing ctDNA monitoring of FGFR3-altered metastatic urothelial carcinoma treated with dabogratinib (TYRA-300) in the SURF301 trial. Activating FGFR3 mutations and fusions occur in 10-20% of patients with metastatic urothelial carcinoma. Erdafitinib, a pan-FGFR inhibitor, is an approved targeted therapy for FGFR3-altered metastatic urothelial carcinoma. However, low isoform specificity of erdafitinib can lead to side effects, and dose reductions or interruptions occur due to inhibition of FGFR1/2/4.
Dabogratinib is a highly selective inhibitor of FGFR3 with potentially less off-target toxicity relative to pan-FGFR inhibitors and has shown preclinical activity against FGFR3 gatekeeper mutations. SURF301 (NCT05544552) is a phase 1/2 study in solid tumors testing oral dabogratinib, with a previously reported 55% (6/11) of patients achieving confirmed partial responses at doses of 90 mg daily or above. At ASCO GU 2026, Andrew Murtha and colleagues reported phase 1 results on early ctDNA dynamics in FGFR3-altered patients with metastatic urothelial carcinoma enrolled in SURF301.
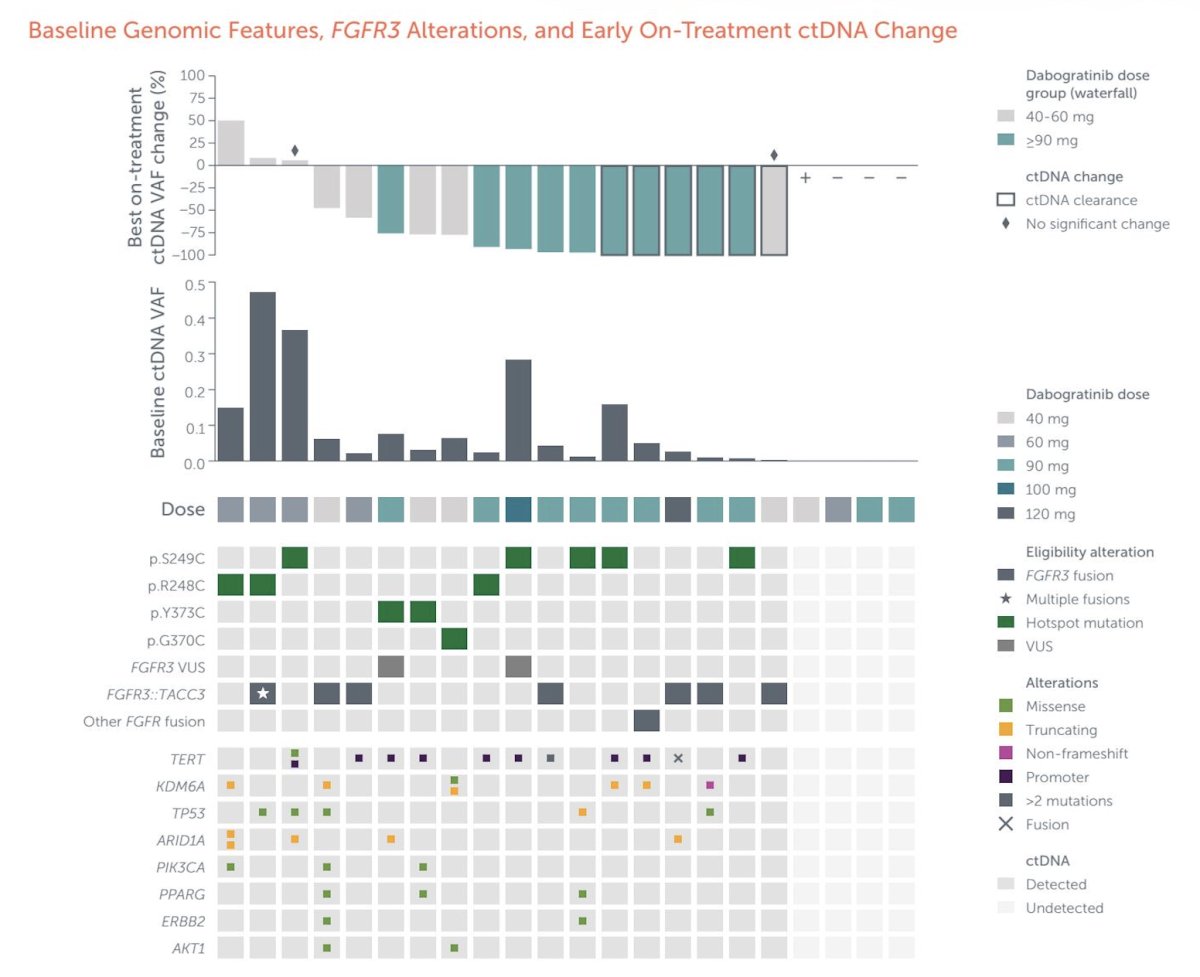
Blood was collected at baseline, cycle 1 day 15 (C1D15), C2D1, and at each disease assessment visit (every 3 months). Plasma cell-free DNA (cfDNA) was sequenced using a custom targeted panel of 78 metastatic urothelial carcinoma genes. Somatic variants were called via an established bioinformatic pipeline, leveraging the same-patient serial samples to boost detection sensitivity. The proportion of tumor-derived cfDNA was estimated using orthogonal approaches and evaluated as an absolute (MTM/mL) and relative measure (ctDNA fraction). On-treatment ctDNA changes from baseline were assessed.
There were 22 metastatic urothelial carcinoma patients that provided blood at baseline and on-treatment. The mean age was 66.7 +/- 8.9 years, and 81.8% had received 2 or more prior lines of therapy. Twelve patients received dabogratinib at ≥ 90mg daily, while 10 received 40-60mg daily. Overall, 18 of 22 patients had ctDNA detected with FGFR3 alterations, including 10 mutations, 7 TACC3 fusions, and 1 patient with both:
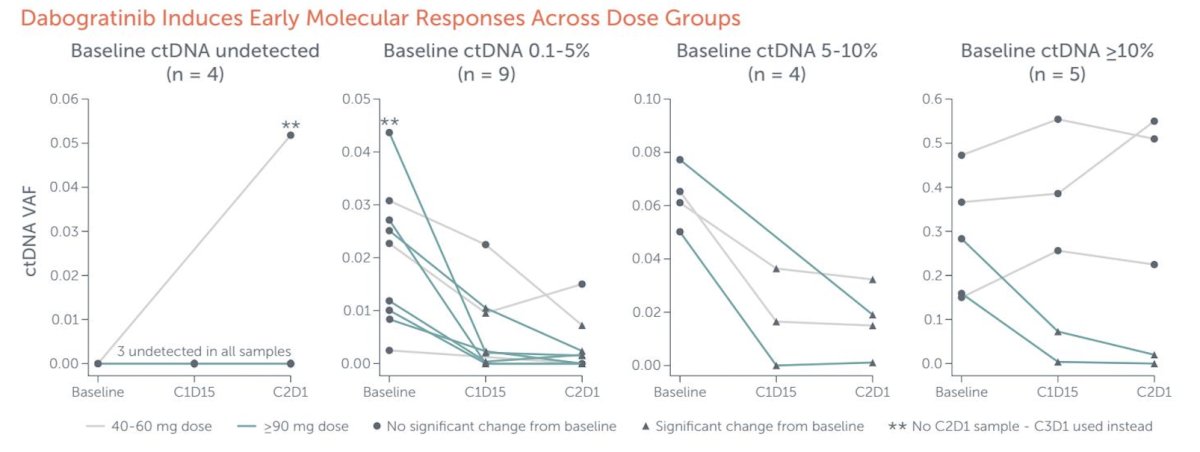
Dabogratinib treatment resulted in significant decreases in ctDNA fraction as early as C1D15 across all dose groups. All patients with 0.1%-10% baseline ctDNA had decreases in ctDNA, independent of dose group. Patients with >=10% ctDNA tended to have poorer ctDNA responses, consistent with high ctDNA being a poor prognostic indicator:
Andrew Murtha concluded his presentation discussing ctDNA monitoring of FGFR3-altered metastatic urothelial carcinoma treated with dabogratinib (TYRA-300) in the SURF301 trial with the following take-home points:
- In the SURF301 trial, oral dabogratinib resulted in rapid decreases of ctDNA in patients with FGFR3-altered metastatic urothelial carcinoma at all doses
- At 40 mg and above, 14 of 18 (78%) participants had molecular responses, and 6 (33.3%) had ctDNA clearance
- Sustained decreases in ctDNA occurred with dabogratinib doses ≥90mg daily in patients with durable partial responses per RECIST v1.1
Presented by: Andrew J. Murtha, University of British Columbia, Vancouver, Canada