(UroToday.com) The 2026 GU ASCO annual meeting featured a urothelial carcinoma session and a presentation by Dr. Aaron C. Zhang discussing the effect of censorship in the interpretation of outcomes of enfortumab vedotin + pembrolizumab in the EV-302 phase 3 randomized clinical trial.
The EV-302 trial is a pivotal phase 3 trial that evaluated the role of the combination of enfortumab vedotin + pembrolizumab versus standard chemotherapy as a first-line treatment for locally advanced (unresectable) or metastatic urothelial carcinoma. The trial demonstrated a significant survival advantage for enfortumab vedotin + pembrolizumab,1 however questions may arise regarding disproportionately high rates of treatment discontinuation in the chemotherapy arm for reasons unrelated to adverse events or progression (33% versus 10% with enfortumab vedotin + pembrolizumab, p < .01).
Censoring occurs when subjects are lost to follow-up or drop out of a study due to reasons independent of survival, which in turn affects survival analysis and may bias the results. The original trial protocol specified that progression-free survival follow-up should be censored at the time of initiation of subsequent therapy; a later amendment states that maintenance therapy should not interrupt progression-free survival recording. This potentially introduces informative censoring specifically for the progression-free survival endpoint. Kaplan Meier analyses assume that censored individuals have the same risk of experiencing the event as those who remain under observation at the same time point. With censorship, Kaplan-Meier estimates may no longer provide an accurate reflection of true survival probabilities. As such, Dr. Zhang and colleagues aimed to investigate potential imbalances in censoring between trial arms across different subgroups: (i) the overall population, (ii) PD-L1-high expression, (iii) PD-L1-low expression, (iv) cisplatin-eligible patients, and (v) cisplatin-ineligible patients.
For this analysis, the investigators performed a multistep analysis to assess the impact of differential dropout on trial outcomes. First, Kaplan–Meier curves were reconstructed from published data to estimate time to event outcomes. Second, a reverse Kaplan–Meier analysis was conducted to evaluate censoring patterns in the overall population and key subgroups (PD-L1 expression; cisplatin eligibility). Third, simulation models were employed to test whether informative censoring could negatively impact the survival benefit of enfortumab vedotin + pembrolizumab.
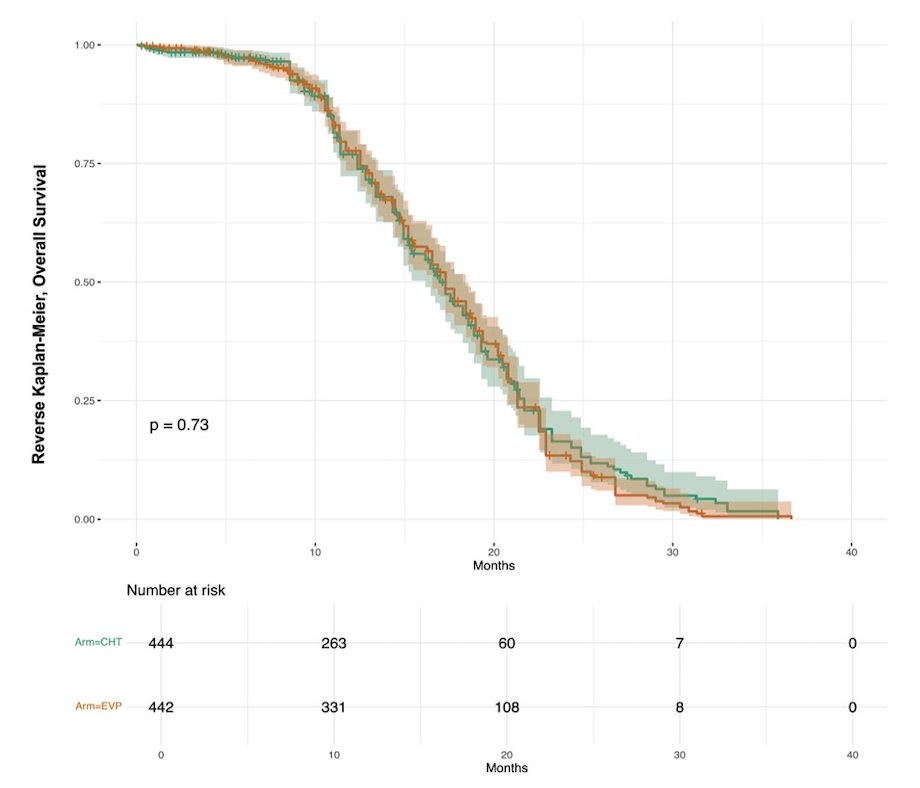
Reverse Kaplan Meier analysis showed similar censoring patterns through the study period between the chemotherapy and enfortumab vedotin + pembrolizumab treatment arms in the EV-302 trial for overall survival:
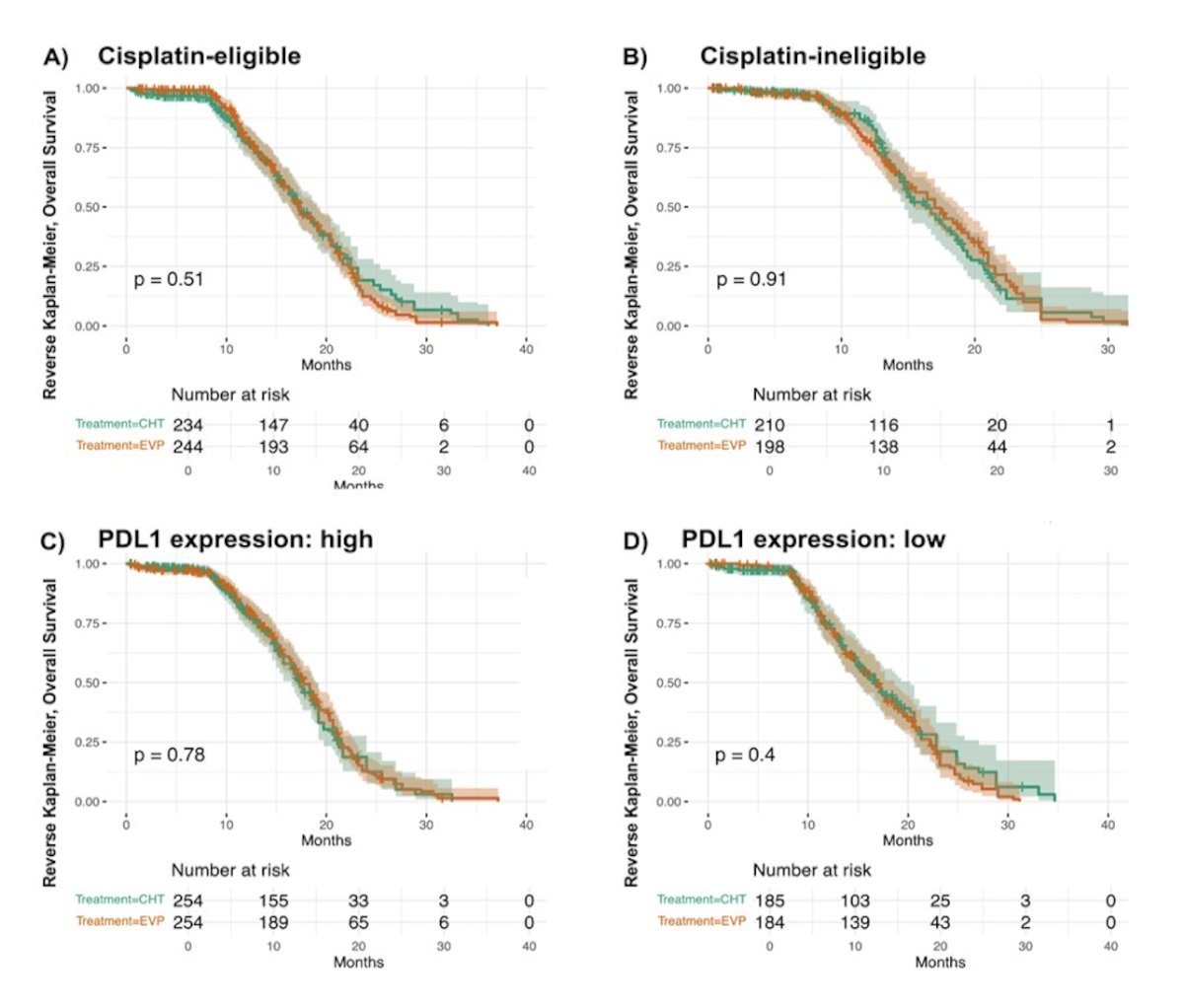
Reverse Kaplan Meier analysis for subgroups also revealed comparable censoring patterns between the enfortumab vedotin + pembrolizumab and chemotherapy treatment arms in all subgroups:
However, when comparing censoring distribution for progression-free survival between enfortumab vedotin + pembrolizumab and chemotherapy, the reverse Kaplan Meier analysis revealed a significant difference in censoring patterns. The chemotherapy arm showed a higher probability of earlier censoring compared to enfortumab vedotin + pembrolizumab (p < 0.01), suggesting potential imbalance between trial arms due to treatment discontinuation: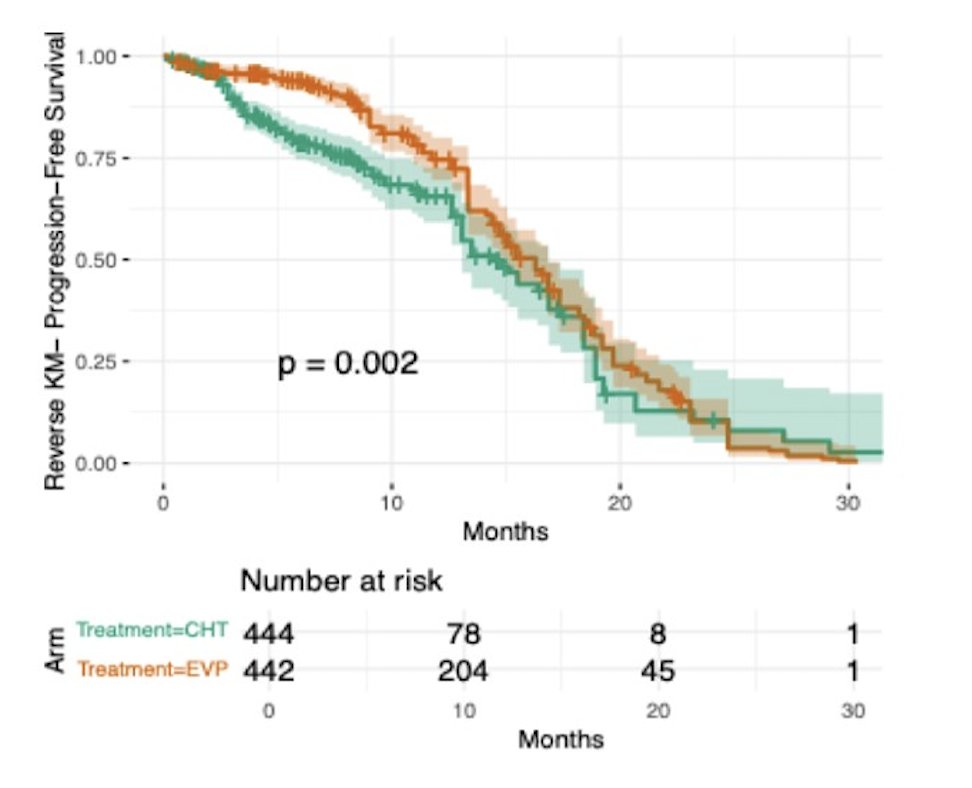
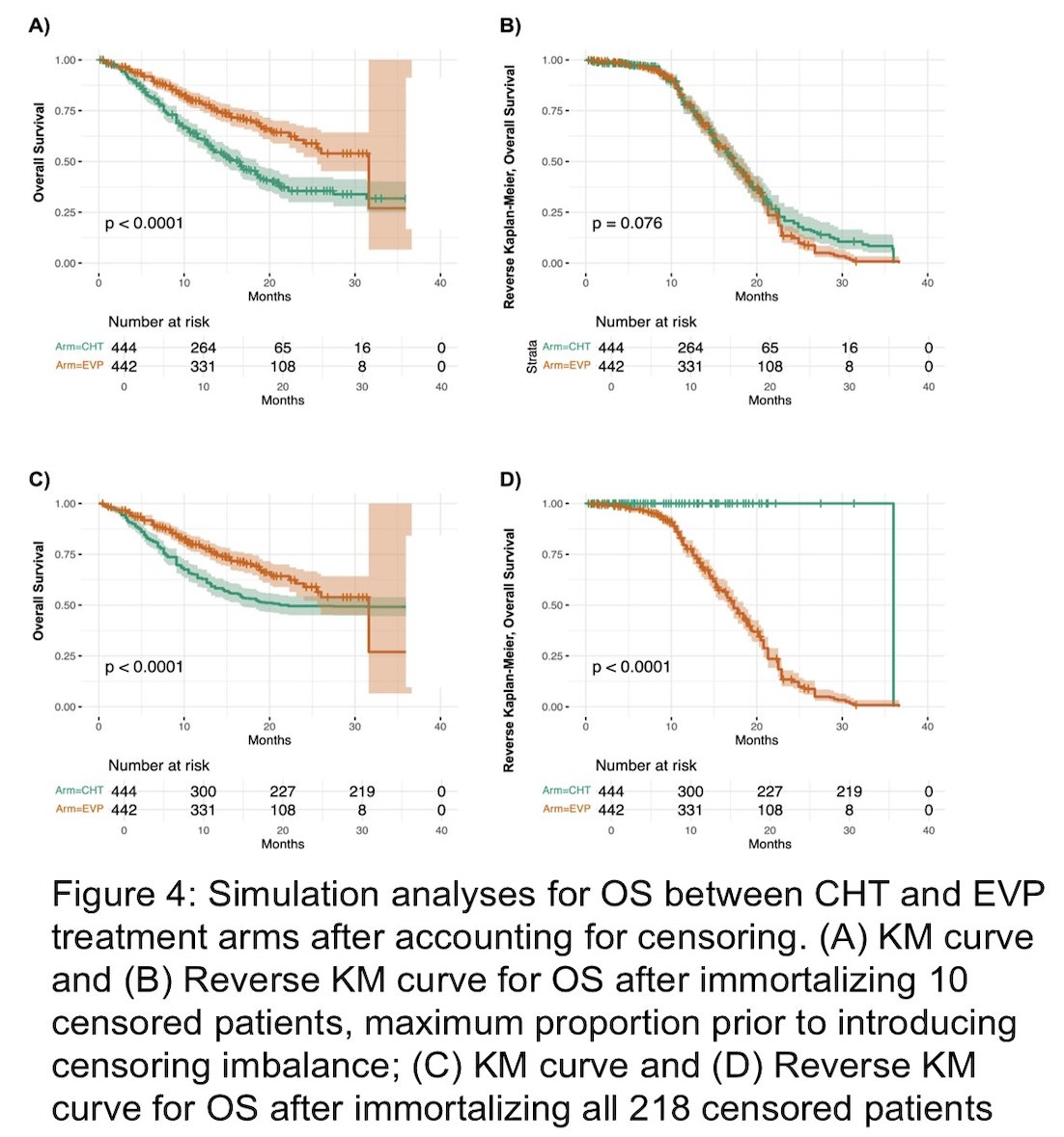
Reverse Kaplan Meier with artificial immortalization of 10 censored patients in the chemotherapy arm, representing the maximum proportion of censored individuals immortalized without introducing censoring imbalance, resulted in a significant separation of survival curves, favoring the enfortumab vedotin + pembrolizumab arm (p < 0.01). A more extreme scenario where all 218 censored patients were treated as immortalized (assuming maximal survival advantage) resulted in markedly important apparent survival in the chemotherapy arm. Despite this, enfortumab vedotin + pembrolizumab still demonstrated superior overall survival, and the comparison remained statistically significant (p < 0.01), underscoring the robustness of the treatment effect:
Dr. Zhang concluded his presentation discussing the effect of censorship in the interpretation of outcomes of enfortumab vedotin + pembrolizumab in the EV-302 phase 3 randomized clinical trial with the following take-home points:
- Reverse Kaplan Meier curves for overall survival revealed balanced censoring patterns between enfortumab vedotin + pembrolizumab and chemotherapy arms, both in the overall cohort and across key clinical subgroups, suggesting that censoring was not a major confounder for overall survival outcomes in the EV-302 trial
- In the EV-302 trial, censoring influenced progression-free survival and overall survival differently because of protocol-defined follow-up. While progression-free survival is widely used as an early indicator of treatment activity, it is particularly vulnerable to informative censoring
- While reverse Kaplan–Meier analysis is a validated method to assess censoring distribution, it does not account for unmeasured confounders or reasons behind patient dropout
- Despite a higher discontinuation rate in the chemotherapy arm, the overall survival benefit of enfortumab vedotin + pembrolizumab in the EV-302 trial remains robust and unaffected by censoring bias
Presented by: Aaron C. Zhang, MD, University of Cincinnati, Cincinnati, OH
Reference: