(UroToday.com) The 2026 GU ASCO annual meeting featured a urothelial carcinoma session and a presentation by Dr. Sarah Psutka discussing updated perioperative outcomes from SunRISe-4 assessing neoadjuvant gemcitabine intravesical therapy + cetrelimab or cetrelimab alone in patients with muscle-invasive bladder cancer ineligible for or refusing neoadjuvant cisplatin-based chemotherapy.
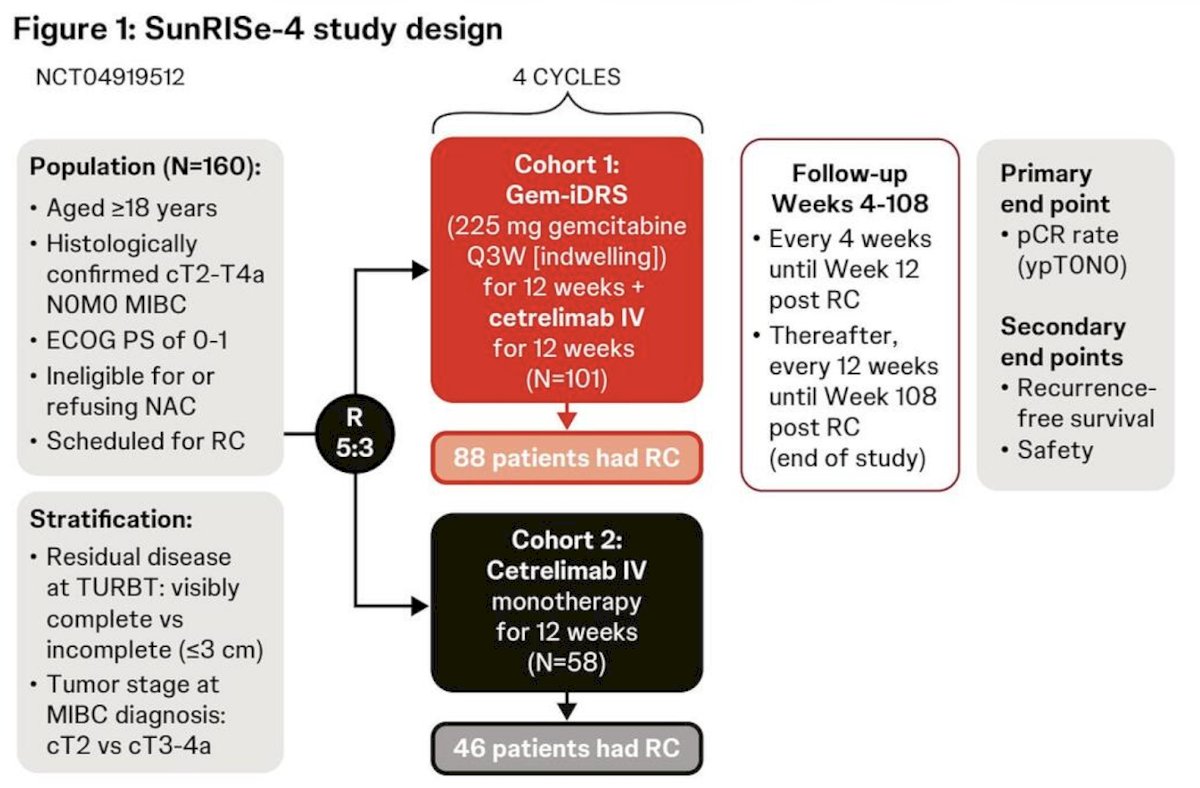
There is a high unmet need for effective neoadjuvant treatments for muscle-invasive bladder cancer that maintain overall health and do not delay or complicate planned radical cystectomy. Gemcitabine intravesical system, previously TAR-200, is a novel intravesical drug-releasing system designed to provide sustained delivery of gemcitabine in the bladder. SunRISe-4 is a randomized phase 2 study evaluating neoadjuvant gemcitabine intravesical system and cetrelimab in patients with muscle-invasive bladder cancer who are ineligible for or refuse neoadjuvant chemotherapy. This analysis from SunRISe-4 evaluated whether neoadjuvant gemcitabine intravesical system + cetrelimab (Cohort 1) or cetrelimab alone (Cohort 2) impacted pre- and post-radical cystectomy surgical, laboratory, or safety outcomes, including clinical declines, delay to radical cystectomy, or increased perioperative complications.
Patients (≥18 years; ECOG performance status 0-1) had histologically confirmed cT2-T4a N0M0 muscle-invasive bladder cancer, were ineligible for or refused neoadjuvant chemotherapy, and planned for radical cystectomy. Patients were randomized 5:3 to receive gemcitabine intravesical system + cetrelimab or cetrelimab alone Q3W for 12 weeks, followed by radical cystectomy (protocol-specified radical cystectomy window: 11-15 weeks):
Perioperative outcomes included time to radical cystectomy, 30- and 90-day post-radical cystectomy morbidity and mortality, and changes in treatments in ECOG performance status, BMI, albumin, creatinine, and hemoglobin. ECOG performance status was recorded on site at baseline and weeks 6 and 36.
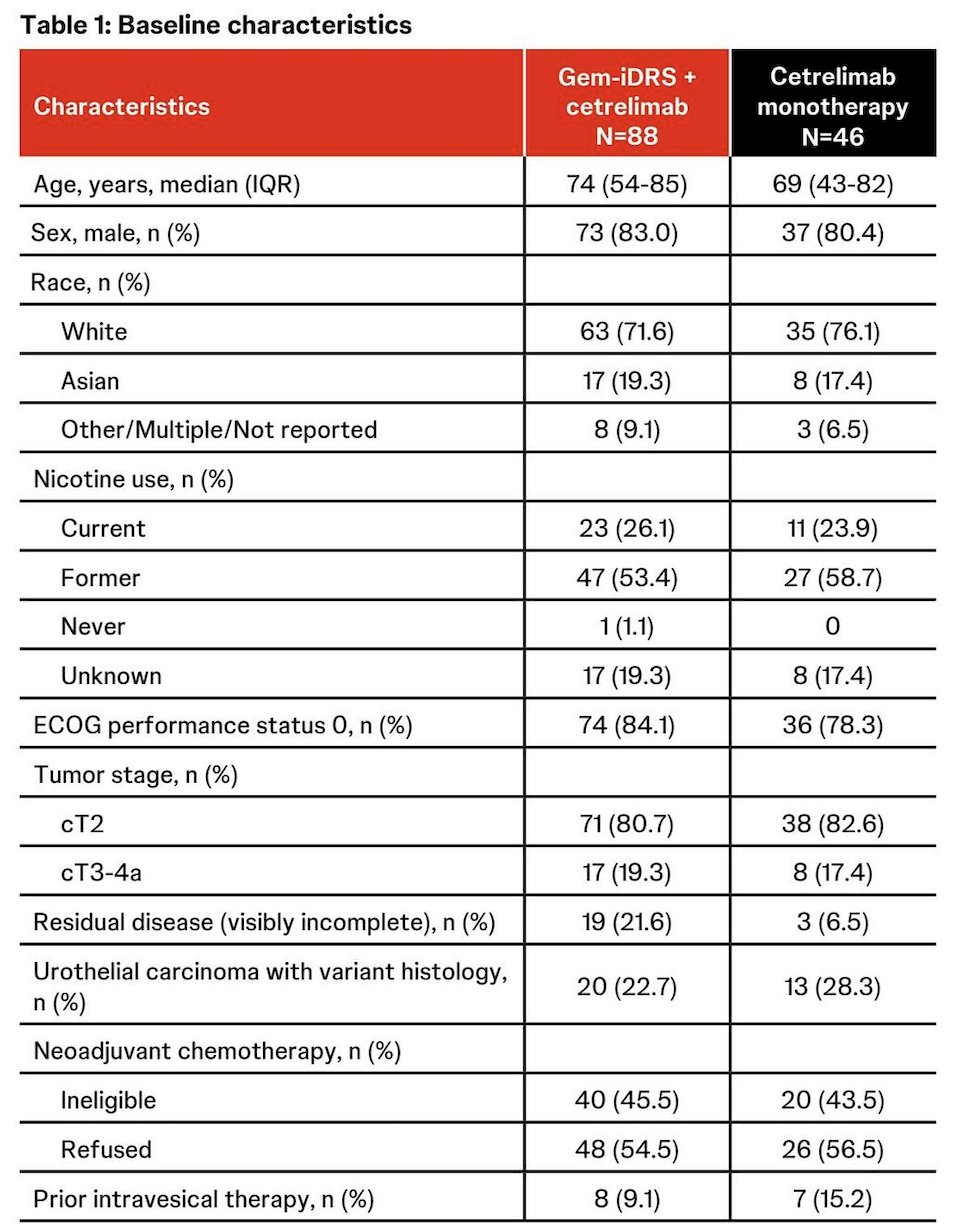
As of May 9, 2025, data cutoff, 134 patients underwent radical cystectomy (Cohort 1: 88; Cohort 2: 46). Demographics and baseline disease characteristics for patients receiving radical cystectomy were balanced across the treatment cohorts:
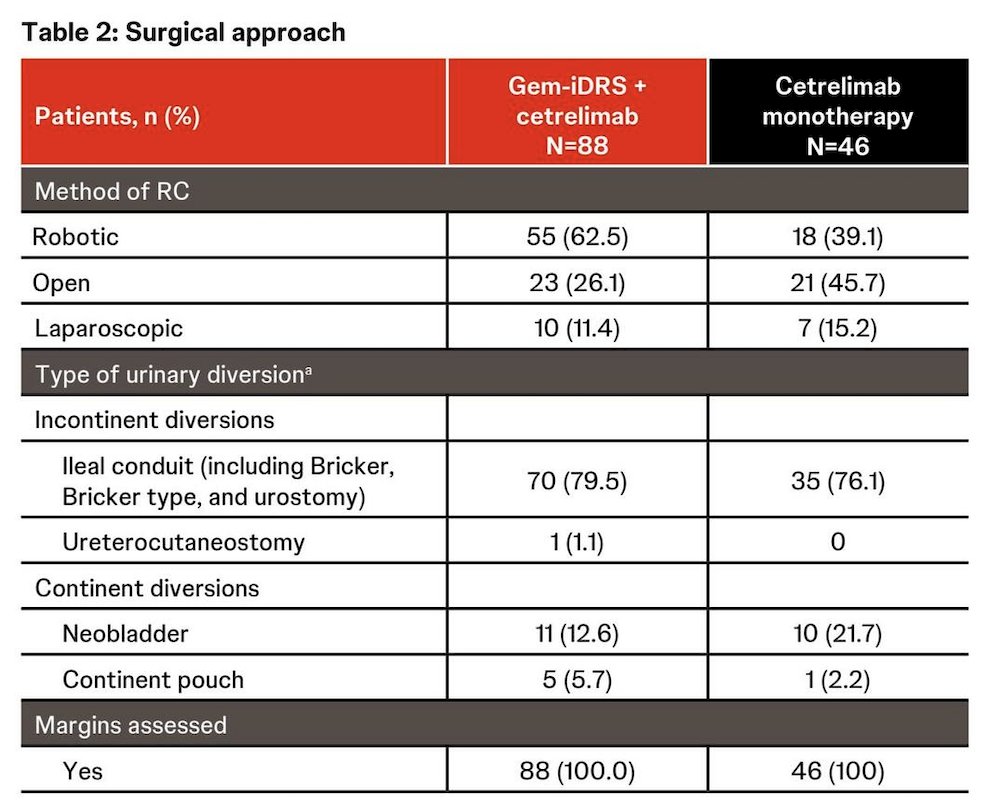
The surgical approach was per physician preference, with ileal conduit being the most frequently used type of urinary diversion in either cohort (79.5% in Cohort 1 and 76.1% in Cohort 2):
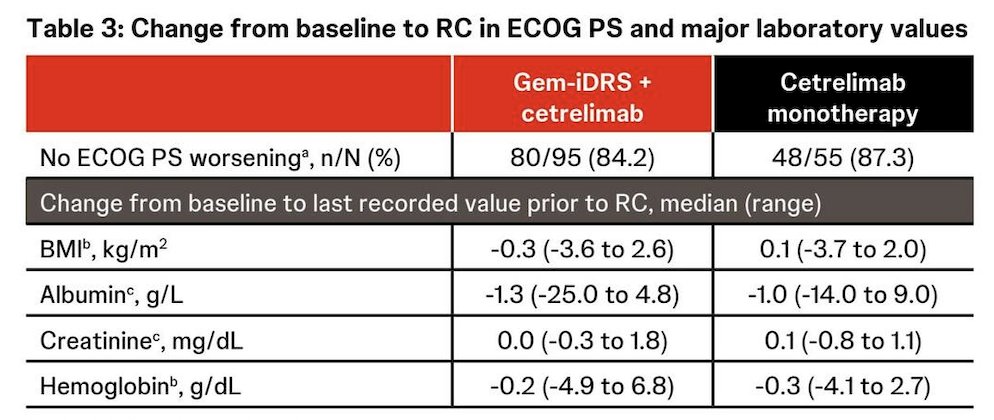
ECOG performance status was preserved in the majority of patients in both cohorts, with no clinically significant changes in ECOG, BMI, albumin, creatinine, and hemoglobin noted on treatment:
The median time from neoadjuvant therapy initiation to radical cystectomy was 13.6 weeks in Cohort 1 and 13.0 weeks in Cohort 2, with most patients having radical cystectomy within the window (Cohort 1: 85.2%; Cohort 2: 84.8%):
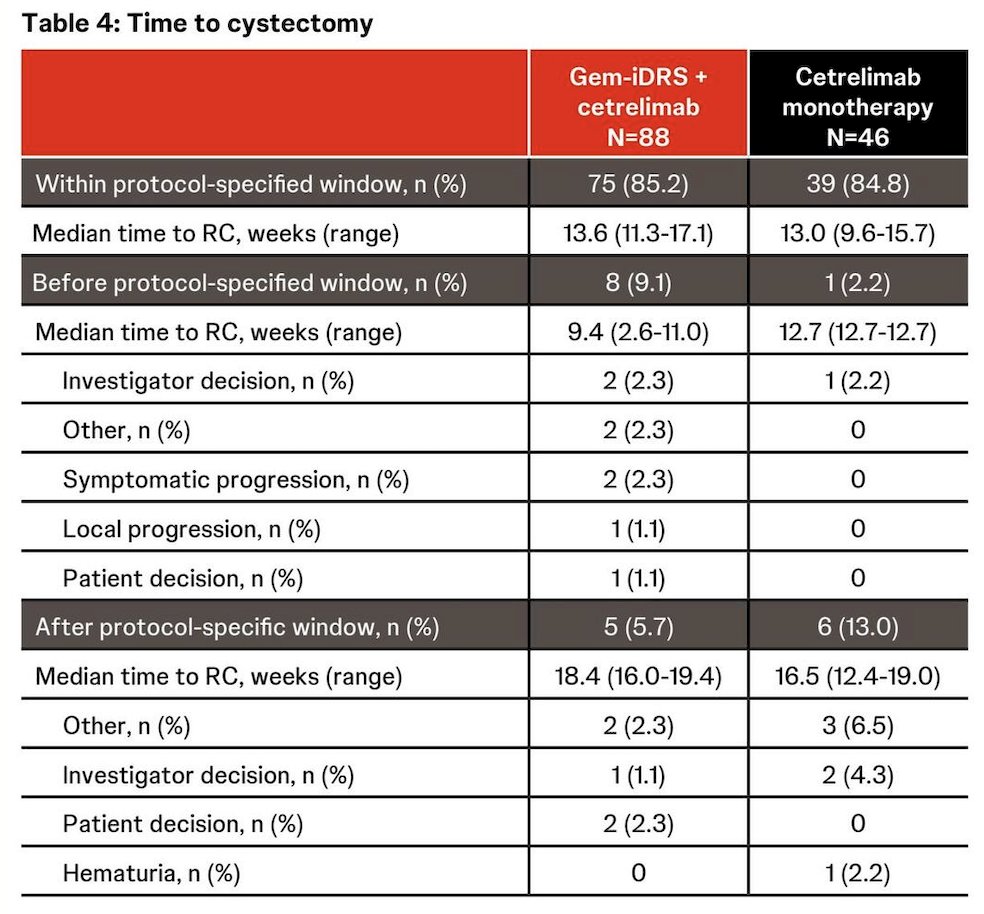
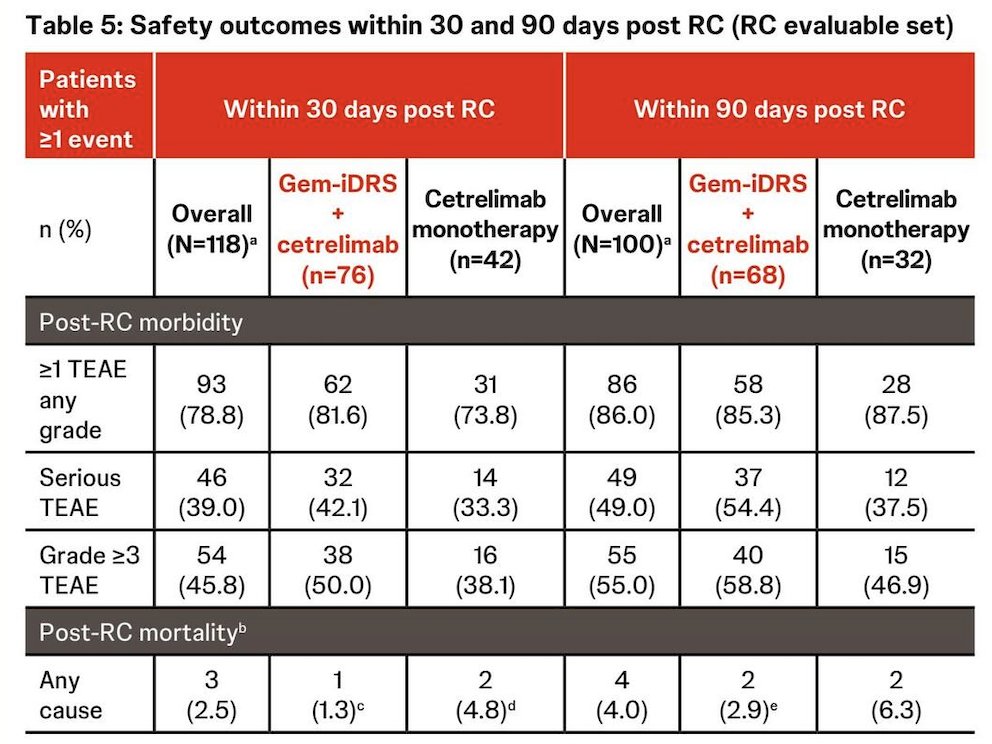
Among 11 patients who had radical cystectomy after the protocol-specified window, only one surgery was delayed because of an adverse event during neoadjuvant treatment (grade 2 hematuria in the cetrelimab monotherapy cohort). Post-radical cystectomy mortality rates at 30 and 90 days were 1.3% and 2.9% (Cohort 1), and 4.8% and 6.3% (Cohort 2), respectively, consistent with historical data:
Dr. Psutka concluded her presentation discussing updated perioperative outcomes from SunRISe-4 with the following take-home points:
- In patients with muscle-invasive bladder cancer ineligible for or refused neoadjuvant chemotherapy, neoadjuvant gemcitabine intravesical system + cetrelimab and cetrelimab alone were not associated with declines in overall health, delays to radical cystectomy, or significant increases in 30- and 90-day post-radical cystectomy morbidity or mortality
- The addition of gemcitabine intravesical system to the checkpoint inhibitor cetrelimab did not worsen safety and post-radical cystectomy morbidity compared with cetrelimab alone
Presented by: Sarah Psutka, MD, MS, FACS, Urologic Oncologist, Associate Professor of Urology, Department of Urology, Fred Hutchinson Cancer Research Center, University of Washington, Seattle, WA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 26 – Sat, Feb 28, 2026.
Related content: SunRISe-4 Examines Neoadjuvant Cetrelimab and Gem-iDRS Prior to Cystectomy in Cisplatin-Ineligible Patients - Sarah Psutka