(UroToday.com) The 2026 GU ASCO annual meeting featured a urothelial carcinoma session and a presentation by Dr. Raj Satkunasivam discussing results from ADVANCED-2, assessing interim efficacy and safety data in BCG-unresponsive participants with high-grade non-muscle invasive bladder cancer. Although patients with BCG-unresponsive non-muscle invasive bladder cancer have several emerging therapeutic options, there remains a clinical unmet need to improve efficacy, durability of response, and tolerability while obviating the need for radical cystectomy.
TARA-002 is a lyophilized biological preparation for intravesical instillation containing inactivated cells of Streptococcus pyogenes (Group A, type 3) Su strain, and rapidly enters cancer cells, activating TLR2 and NOD2 to trigger the innate immune response, inflammation, and potential immunogenic cell death. TARA-002 requires no special handling or thawing and can be rapidly administered via catheter by a healthcare professional in a routine office-based setting. At ASCO GU 2026, Dr. Satkunasivam and colleagues presented the interim safety and efficacy data of TARA-002 from the BCG-unresponsive cohort of the ongoing ADVANCED-2 study.
ADVANCED-2 (Cohort B) is a phase 2, open-label study to evaluate the safety and efficacy of intravesical TARA002 in BCG-unresponsive adults ≥ 18 years with high-grade non-muscle invasive bladder cancer CIS (± Ta/T1). Key exclusion criteria include penicillin allergy, history of ≥ T2 bladder cancer, nodal, or metastatic disease, or concomitant prostatic or upper tract urothelial involvement. TARA-002 is delivered intravesically for 2 hours and includes induction (6 weekly doses), reinduction (if persistent disease at 3 months), and maintenance (through 24 months):
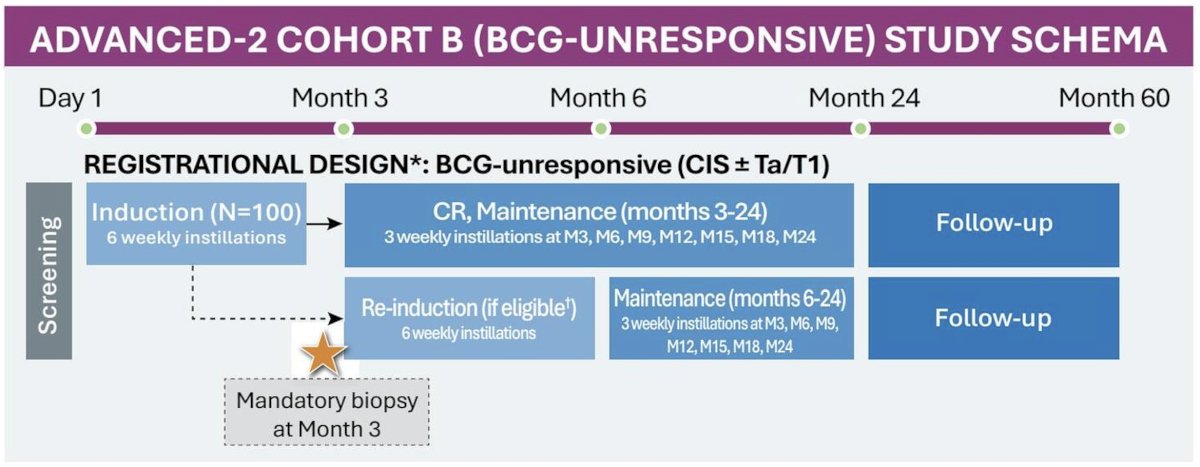
Response is assessed every 3 months for 2 years, and a biopsy is mandated at month 3. Long-term follow-up is conducted up to 60 months, and safety is monitored throughout the study. The primary endpoint is complete response at any time, defined by the absence of any high-grade recurrence. The key secondary endpoint is duration of response.
To date, 43 BCG-unresponsive participants have been enrolled; the majority of participants were White (81.4%, 35 of 43), and male (72.1%, 31 of 43), with a median age of 75 years (range: 47 to 92). TARA-002 demonstrated a 65.7% (23 of 35) complete response at any time in evaluable participants. The 6-month complete response was 68.2% (15 of 22), and the 12-month complete response was 33.3% (5 of 15):

Among initial responders, 100% (7 of 7) maintained their response through month 6, 80% (4 of 5) through month 9, and 100% (2 of 2) through month 12. Among the initial non-responders who underwent re-induction, 61.5% (8 of 13) converted to a complete response by month 6, 71.4% (5 of 7) responders maintained the complete response through month 9, and 100% (3 of 3) through month 12:

The majority of treatment-related adverse events were grade 1 and transient, with the most common including dysuria, bladder spasm, and micturition urgency. There were no participants who experienced grade 3+ treatment-related adverse events, drug-related serious adverse events, or drug-related treatment-emergent adverse events leading to withdrawal or death:

Dr. Satkunasivam concluded his presentation discussing results from ADVANCED-2 with the following take-home points:
- In participants with BCG-unresponsive high-risk non-muscle invasive bladder cancer with CIS ± Ta/T1, TARA-002 appears to be well tolerated and demonstrated encouraging efficacy, supporting ongoing accrual of the ADVANCED-2 study
- Re-induction therapy successfully salvaged a significant proportion of initial non-responders, resulting in high conversion rates and durable responses
Presented by: Raj Satkunasivam, MD, MS, FRCSC, Houston Methodist Hospital, Houston, TX
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 26 – Sat, Feb 28, 2026.