(UroToday.com) The 2026 GU ASCO annual meeting featured a urothelial carcinoma trials in progress session and a presentation by Dr. Ananya Choudhury discussing TRAIN, a phase III randomized control clinical trial of radiotherapy with radiosensitization versus intravesical BCG therapy for high-risk non-muscle invasive bladder cancer.
High-risk non-muscle invasive bladder cancer is typically treated with surgery (TURBT) followed by intravesical BCG or radical cystectomy. Induction BCG is given weekly for six weeks, followed by maintenance for up to 3 years. However, up to 50% of patients experience recurrence or progression, and 25% discontinue due to toxicity. Global BCG shortages have further increased recurrence rates and costs. Thus, there is a clear need for alternative treatments to reduce recurrence, progression, cystectomy rates, and mitigate supply issues. The NIHR funded the TRAIN trial (ISRCTN: 16345179) will assess radiotherapy with radiosensitization drugs as an alternative treatment option.
Co-ordinated by the Cancer Research UK Southampton Clinical Trials Unit, TRAIN is a multicenter, two-arm, open-label UK randomized phase III trial comparing usual care (BCG) with radiotherapy (55Gy/20#) and a radiosensitizer in high-risk non-muscle invasive bladder cancer patients who have undergone maximal TURBT and are BCG naïve. Treatment allocation ratio is 1:1, stratified by disease stage and age.
Radiotherapy arm participants receive investigator choice of radiosensitizer (gemcitabine, mitomycin C/fluorouracil or carbogen/nicotinamide) and will receive radiotherapy 55Gy in 20 fractions, treating once daily Monday to Friday over 4 weeks. Participants randomized to BCG (control) will be treated following European Association of Urology guidelines. All participants will be followed for a minimum of two years:
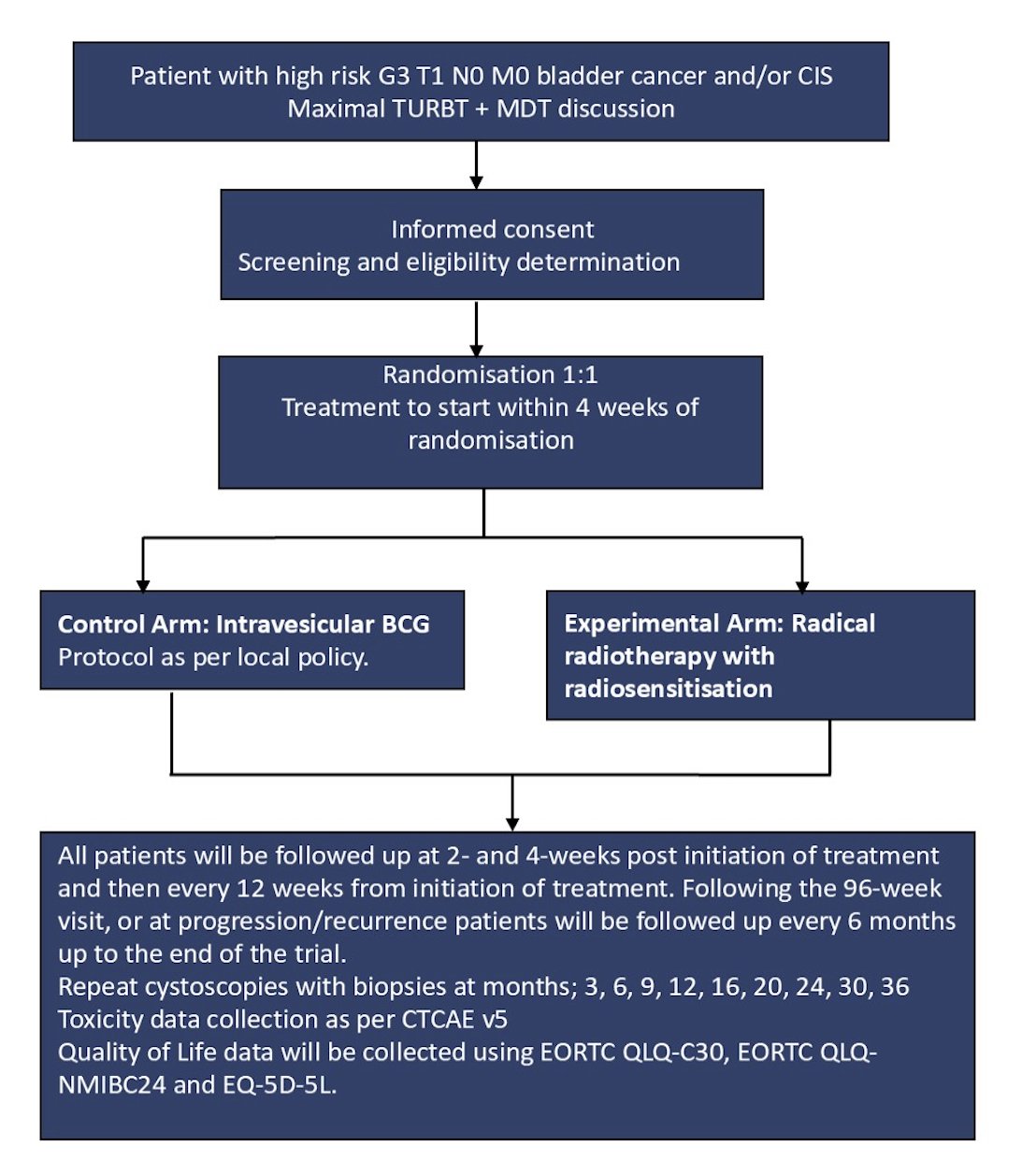
The primary endpoint is event-free survival, defined as time from randomization to any of CIS or high-risk grade 3 non-muscle invasive papillary tumor recurrence, continued presence of high-risk non-muscle invasive bladder cancer even after treatment completion, progression to muscle invasive disease, distant metastatic bladder cancer, cystectomy (for any reason) or death from any cause. Treatment will continue until the patient has either had an event, unacceptable toxicity or withdrawn.
Accounting for 5% drop out, the total sample size of 328 patients (90 events) was calculated using alpha = 0.025 (one-sided), power = 0.9, hazard ratio = 0.5, and a piecewise exponential survival distribution with event rate in the control arm of 10, 20, 25, and 30% at 3, 6, 12 and 24 months. An interim analysis for futility is planned for when 50% of events have occurred. The study will stop if the observed hazard ratio is greater than 0.924.
Secondary endpoints include recurrence-free survival, cancer-specific survival, cystectomy-free survival, progression-free survival, metastasis-free survival, overall survival, treatment fidelity, cost effectiveness, and safety/tolerability.
TRAIN will be run in approximately 12-20 UK secondary care hospitals, randomizing 328 patients:

Presented by: Ananya Choudhury, University of Manchester, Manchester, UK
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 26 – Sat, Feb 28, 2026.
Related content: Revisiting Radiation for Non-Muscle-Invasive Bladder Cancer - Ananya Choudhury