(UroToday.com) The 2026 ASCO GU Annual Symposium was host to a session on integrating emerging evidence into practice for the management of non-muscle invasive bladder cancer (NMIBC) patients. Dr. Ananya Choudhury discussed optimizing radiation therapy for NMIBC.
NMIBC management continues to evolve as clinicians seek to balance oncologic control, treatment toxicity, and patient quality of life. While intravesical bacillus Calmette-Guérin (BCG) remains a cornerstone of therapy for high-risk disease, significant toxicity, treatment failures, and emerging therapeutic options have prompted renewed interest in alternative bladder-preserving strategies. In this presentation, Dr. Choudhury reviewed the role of radiotherapy in high- and very high-risk NMIBC and discussed how modern radiation approaches may complement or potentially replace traditional management strategies in selected patients.
BCG therapy remains highly effective but is associated with substantial toxicity. Data from nine trials, including 2,820 patients, demonstrated that BCG maintenance therapy improves time to first recurrence compared with mitomycin C, with a statistically significant benefit in recurrence reduction. However, treatment-related toxicity is common. Local adverse events occur frequently, including bacterial cystitis (25.9%), BCG cystitis (47.4%), urinary frequency (31.4%), and macroscopic hematuria (34.5%). Overall, 75.2% of patients experience some form of local toxicity, with treatment delays occurring in 18.3% and discontinuation in 14.8%. Systemic adverse events occur in approximately 39.4% of patients, although severe complications such as BCG sepsis remain rare. These toxicity profiles highlight the clinical challenge of balancing efficacy and tolerability in long-term BCG therapy.1-2

Another important clinical consideration is the morbidity associated with radical cystectomy. Approximately two-thirds of patients undergoing cystectomy experience postoperative adverse events, underscoring the significant perioperative risks associated with this definitive surgical approach. Given the toxicity of both BCG and radical cystectomy, there is growing interest in exploring alternative bladder-preserving strategies.
From a biological perspective, bladder cancer demonstrates radiosensitivity. Experimental studies evaluating bladder cancer cell lines show variability in radiosensitivity across tumor phenotypes; however, NMIBC overall appears responsive to radiation therapy. These observations support the biological rationale for investigating radiotherapy as a potential treatment modality in earlier stages of bladder cancer.3-4

In parallel, several novel systemic agents are being explored in NMIBC. Trials such as POTOMAC, ALBAN, and CREST have investigated checkpoint inhibitor–based combinations and other novel therapies in this disease setting. While these agents show promise, they are associated with high costs and potential immune-related toxicities, raising questions about their long-term clinical and economic sustainability.5-7

Historically, evidence supporting radiotherapy for NMIBC has been limited. An older Medical Research Council (MRC) trial conducted between 1991 and 2003 randomized 210 patients but ultimately proved underpowered and did not demonstrate a statistically significant difference in recurrence outcomes between treatment groups. As a result, radiotherapy did not gain widespread adoption in NMIBC despite its established role in muscle-invasive bladder cancer.⁸

Subsequent meta-analyses evaluating historical radiotherapy studies in NMIBC have similarly been inconclusive. These analyses highlight several methodological limitations including small sample sizes, incomplete data reporting, outdated radiotherapy techniques, and heterogeneous patient populations. Consequently, the available evidence has remained insufficient to define a clear role for radiation therapy in NMIBC management.⁹

More recently, prospective studies have begun to revisit this question using modern treatment approaches. The Hoosier Cancer Research Network GU16-243 ADAPT-BLADDER study evaluated durvalumab-based strategies combined with either BCG or external beam radiotherapy. Among evaluable patients, the combination of durvalumab and BCG demonstrated encouraging complete response rates, reaching 85% at 3 months, 83% at 6 months, and 73% at 12 months. These findings suggest that immune-radiotherapy combinations may offer a promising bladder-preserving strategy.¹⁰

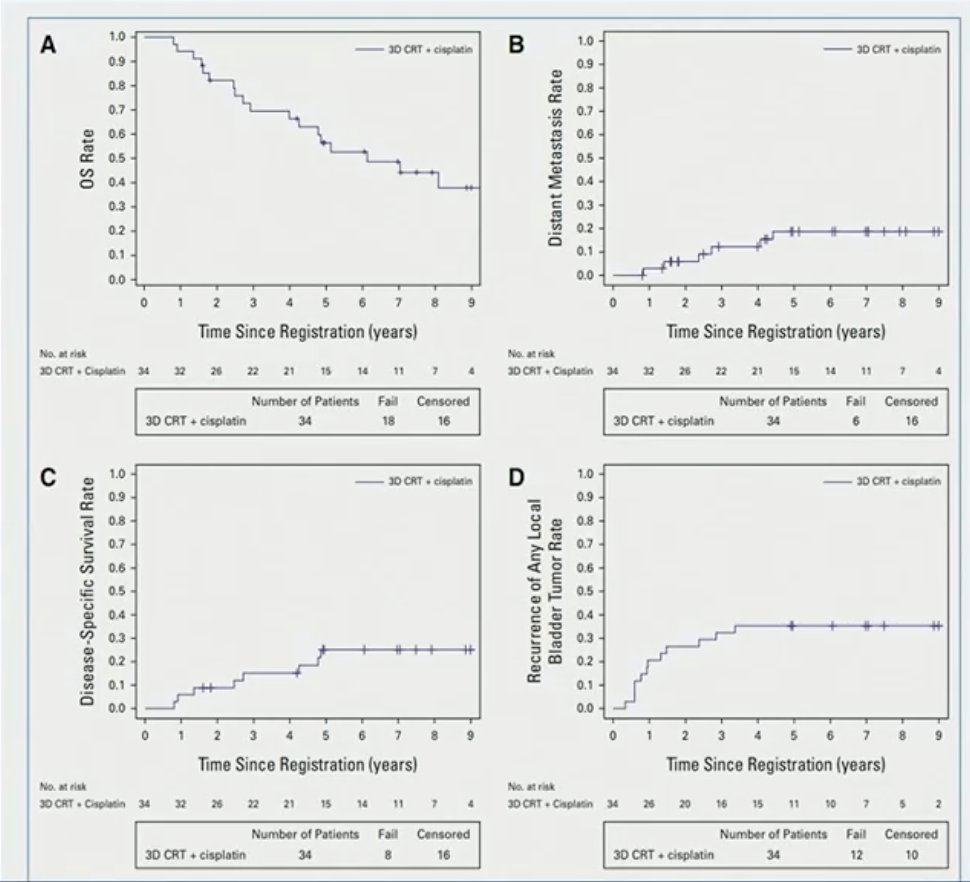
The NRG/RTOG 0926 trial further explored the feasibility of trimodality therapy in high-risk NMIBC. This single-arm phase II study evaluated patients with recurrent or BCG-ineligible T1G3 disease treated with radiotherapy (61.2 Gy in 34 fractions) combined with radiosensitizing chemotherapy (cisplatin or mitomycin C/5-fluorouracil). Among 34 enrolled patients (median age 74 years), the three-year cystectomy-free survival rate was 88%. However, 12 patients experienced local recurrence by three years and 17 patients developed grade ≥3 acute toxicity. These results demonstrate the feasibility of a bladder-preserving chemoradiation approach but also highlight the need for further refinement of treatment strategies.¹¹
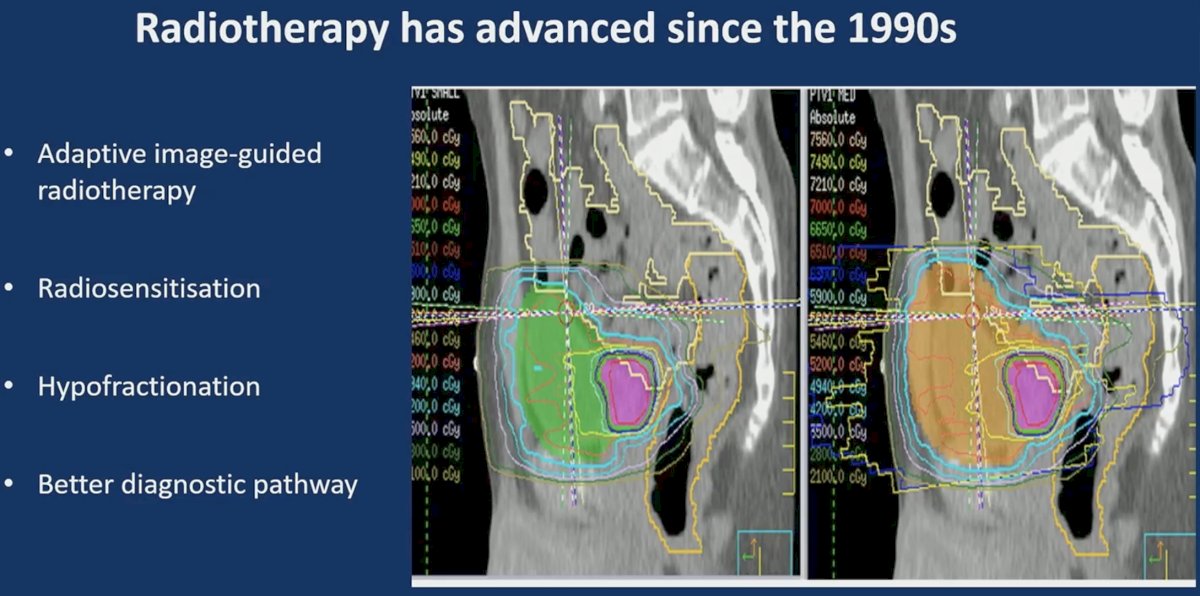
Importantly, radiotherapy techniques have evolved substantially since the early NMIBC studies. Modern radiation oncology incorporates adaptive image-guided radiotherapy, improved radiosensitization strategies, hypofractionated treatment schedules, and improved diagnostic imaging pathways. These technological advances have the potential to enhance both treatment precision and oncologic outcomes while minimizing toxicity.
Evidence from muscle-invasive bladder cancer also supports the value of combining radiotherapy with radiosensitizing agents. Randomized trials such as BC2001 demonstrated that the addition of chemotherapy (mitomycin C and 5-FU) to radiotherapy significantly improves locoregional disease-free survival compared with radiotherapy alone (hazard ratio 0.66, p=0.02). Earlier studies evaluating cisplatin-based radiosensitization similarly demonstrated improved disease control compared with radiation monotherapy.¹²-¹⁴ These data provide a strong rationale for applying radiosensitization strategies to NMIBC treatment paradigms.

Quality-of-life outcomes are another critical consideration. Data evaluating late toxicity using EQ-5D-5L health status scores demonstrate stable or improved quality-of-life metrics following modern radiotherapy approaches, with comparable outcomes across whole bladder radiotherapy (WBRT), standard adaptive radiotherapy (SART), and dose-adaptive radiotherapy (DART) techniques. These findings suggest that contemporary radiation strategies can maintain acceptable long-term patient-reported outcomes.¹⁵

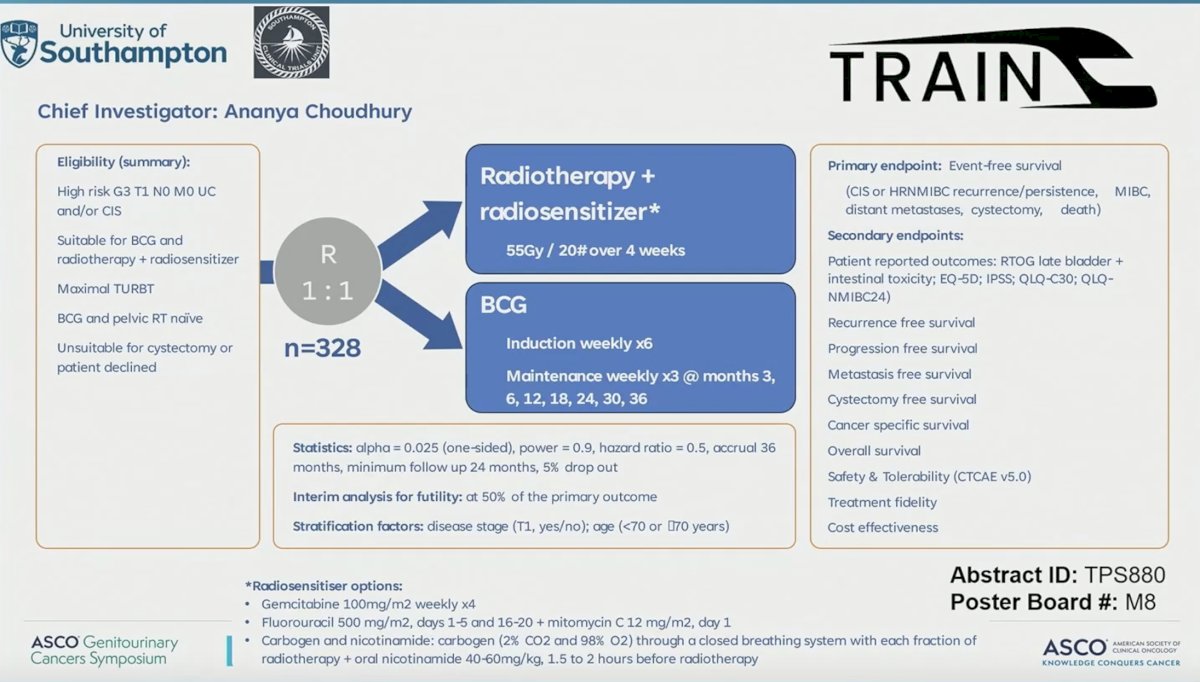
Several ongoing trials are currently evaluating the role of radiotherapy in NMIBC. The PARC trial (NRG-GU014) is a phase II study evaluating external beam radiotherapy combined with pembrolizumab versus radiotherapy with concurrent chemotherapy. The TRAIN trial is a phase III study comparing hypofractionated radiotherapy with radiosensitizer (55 Gy in 20 fractions) versus standard BCG in high-risk BCG-naïve NMIBC. Another phase II study is evaluating external beam radiotherapy in patients with BCG-unresponsive disease. These trials aim to determine whether radiotherapy can emerge as a viable alternative or adjunct to current NMIBC treatments.

In summary, BCG remains an effective therapy for high-risk NMIBC but is associated with substantial toxicity. Emerging systemic therapies offer promising activity but are costly and carry their own toxicity profiles. While radiotherapy is well established in muscle-invasive bladder cancer, its role in NMIBC remains poorly defined due to limited and outdated data. Advances in radiation technology, improved radiosensitization strategies, and ongoing randomized trials may help clarify whether modern radiotherapy can serve as a safe and effective bladder-preserving treatment option for patients with NMIBC. Ultimately, results from ongoing late-phase trials will determine whether radiotherapy can be integrated into future NMIBC treatment algorithms.
Presented by: Ananya Choudhury, MA (Cantab), PhD, MRCP, FRCR, Professor, Chair and Honorary Consultant in Clinical Oncology, The Christie NHS Foundation Trust, Manchester, UK
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026.
References:
- Malmström PU, Sylvester RJ, Crawford DE, et al. An individual patient data meta-analysis of the long-term outcome of randomised studies comparing intravesical mitomycin C versus bacillus Calmette–Guérin for non–muscle-invasive bladder cancer. Eur Urol. 2009;56(2):247-256.
- Adriaensen MEAPM, Sylvester RJ, Collette L, et al. Quality of life results from a randomized trial comparing intravesical bacillus Calmette–Guérin with mitomycin C for intermediate- and high-risk superficial bladder cancer. Eur Urol. 2004;44(4):429-434.
- Barneston AR, Mameghan H, Turner SL, et al. Radiosensitivity of human bladder carcinoma cell lines and the effect of hypoxia. Radiat Oncol Investig. 1999;7(4):214-221.
- Bodgi L, Canet A, Pujo-Menjouet L, et al. Mathematical modeling of radiation response in bladder cancer cells reveals heterogeneity in radiosensitivity. Front Oncol. 2019;9:1379.
- Shore ND, Bivalacqua TJ, Cookson MS, et al. Pembrolizumab plus bacillus Calmette–Guérin for high-risk non–muscle-invasive bladder cancer: Results from the phase III CREST trial. Nat Med. 2025.
- Di Santis M, Bellmunt J, Mead G, et al. Randomized phase II/III trial assessing gemcitabine and cisplatin versus methotrexate, vinblastine, doxorubicin, and cisplatin in patients with advanced or metastatic urothelial cancer: EORTC intergroup study 30987. J Clin Oncol. 2012;30(2):191-199.
- James ND, Hussain SA, Hall E, et al. Radiotherapy with or without chemotherapy in muscle-invasive bladder cancer. N Engl J Med. 2012;366(16):1477-1488.
- Mak RH, Hunt D, Shipley WU, et al. Long-term outcomes in patients with muscle-invasive bladder cancer after selective bladder-preserving combined-modality therapy: A pooled analysis of RTOG trials. J Clin Oncol. 2014;32(34):3801-3809.
- Sylvester RJ, van der Meijden APM, Oosterlinck W, et al. Predicting recurrence and progression in individual patients with stage Ta T1 bladder cancer using EORTC risk tables: A combined analysis of 2596 patients from seven EORTC trials. Eur Urol. 2006;49(3):466-477.
- Kitamura H, Tsukamoto T, Shibata T, et al. En bloc transurethral resection of bladder tumor. J Urol. 1980;124(3):374-375.
- Teoh JYC, Cheng CH, Tsang CF, et al. Transurethral en bloc resection versus conventional transurethral resection of bladder tumour: A randomized, multicentre, phase 3 trial. Eur Urol. 2022;81(6):635-642.
- Teoh JYC, Bracco FM, Wong JHF, et al. A novel transurethral robotic platform for performing en bloc resection of bladder tumour: Results from the first phase of the VIABLE trial. Eur Urol Oncol. 2025.
- Babjuk M, Burger M, Capoun O, et al. European Association of Urology guidelines on non–muscle-invasive bladder cancer (TaT1 and CIS). Eur Urol. 2022;81(1):75-94.
- Chang SS, Boorjian SA, Chou R, et al. Diagnosis and treatment of non–muscle invasive bladder cancer: AUA/SUO guideline. J Urol. 2016;196(4):1021-1029.
- Kamat AM, Sylvester RJ, Böhle A, et al. Definitions, end points, and clinical trial designs for non–muscle-invasive bladder cancer: Recommendations from the International Bladder Cancer Group. J Clin Oncol. 2016;34(16):1935-1944.