(UroToday.com) The 2026 ASCO GU Annual Symposium was host to a session on integrating emerging evidence into practice for the management of non-muscle invasive bladder cancer (NMIBC) patients. Dr. Jeremy Teoh discussed optimizing the surgical management of NMIBC.
Dr. Teoh noted that transurethral resection of bladder tumor (TURBT) remains the cornerstone of diagnosis and treatment for NMIBC The modern TURBT procedure evolved over more than a century of endoscopic innovation. Early milestones included the development of the Lichtleiter by Philipp Bozzini in 1806, followed by the first endoscopic removal of urethral papilloma by Desormeaux in 1853. Subsequent advances included the development of cystoscopy, electrosurgical energy sources, and eventually the first resectoscope introduced by Stern in 1926. Later innovations, including fiberoptic imaging and video-assisted endoscopy, helped establish the modern TURBT platform used today.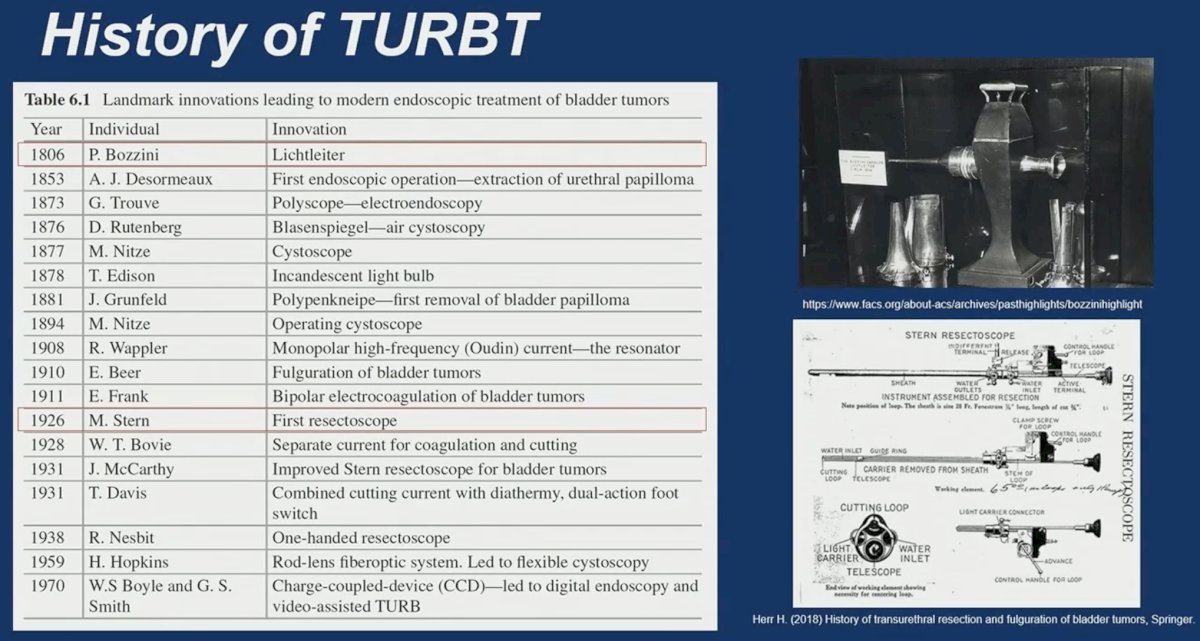
Despite these technological advances, the quality of the initial TURBT remains a critical determinant of oncologic outcomes in NMIBC. Accurate staging and complete tumor resection are essential to guide subsequent management strategies.
Clinical decision-making in NMIBC is largely guided by risk stratification tools. One of the most widely used models is the European Organisation for Research and Treatment of Cancer (EORTC) risk table, developed from a pooled analysis of 2,596 patients across seven EORTC trials. This model predicts both recurrence and progression based on clinical and pathologic variables, including tumor size, number of tumors, prior recurrence rate, stage, grade, and presence of carcinoma in situ.1
For example, patients with an EORTC recurrence score of 5 have an estimated recurrence risk of approximately 38% at 1 year and 62% at 5 years. Corresponding progression risks are approximately 1% at 1 year and 6% at 5 years. These tools emphasize the importance of accurate staging and high-quality initial tumor resection to optimize risk stratification and guide treatment decisions.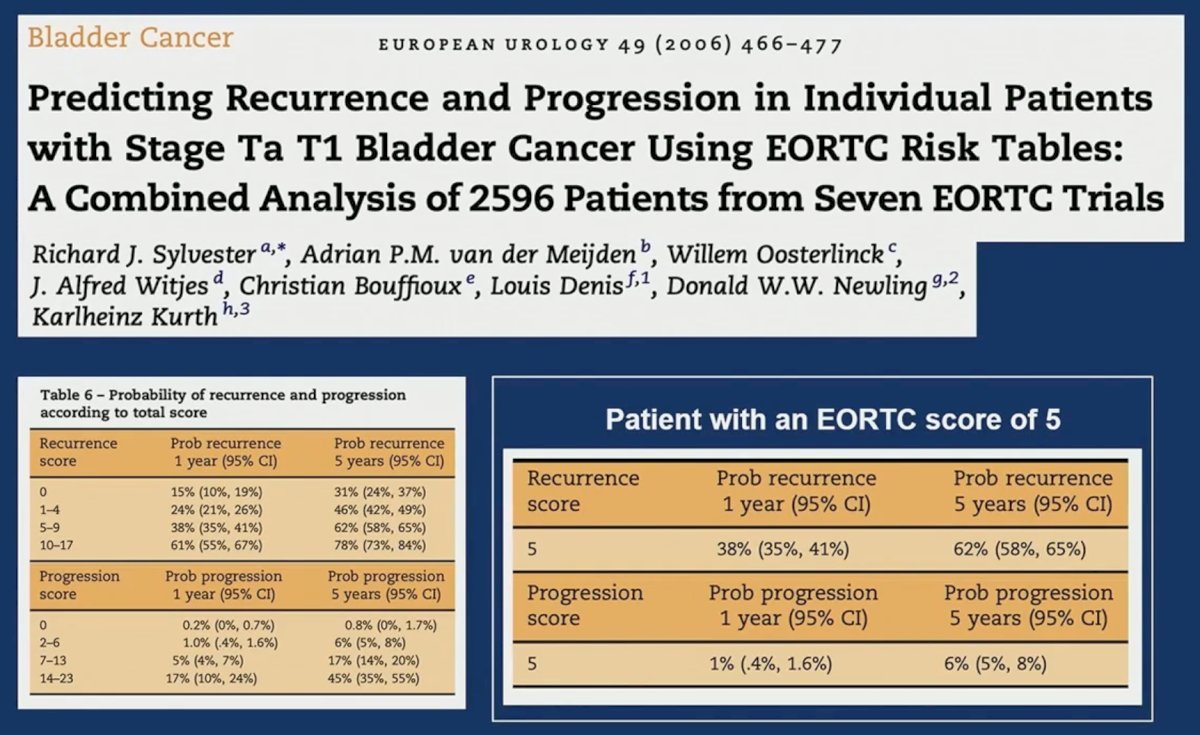
One strategy proposed to improve the surgical quality in NMIBC is en bloc resection of bladder tumor (ERBT). First described by Kitamura and colleagues in 1980, ERBT removes the tumor in a single intact specimen rather than piecemeal resection.
This technique offers several potential advantages. By avoiding tumor fragmentation, ERBT may reduce the risk of tumor cell reimplantation. It also allows the entire specimen—including both circumferential and deep margins—to be evaluated histologically. This enables improved pathologic assessment of tumor invasion depth and margin status. Various energy modalities can be used to perform ERBT, including bipolar electrocautery, holmium laser, and thulium laser systems.
Because the specimen is removed intact, both lateral and deep margins can be inked and evaluated by the pathologist. This facilitates more accurate staging and may reduce the likelihood of understaging.
What about randomized evidence supporting ERBT? The EB-StaR study represents one of the key randomized trials evaluating ERBT. This multicenter phase III trial compared transurethral en bloc resection with standard TURBT in patients with NMIBC.2

The primary endpoint was 1-year recurrence. Patients treated with ERBT experienced significantly lower recurrence rates compared with standard resection (28.5% vs 38.1%, p = 0.007). Subgroup analyses suggested that certain patients derived particular benefit from ERBT, including those with tumors measuring 1–3 cm, solitary tumors, Ta disease, and intermediate-risk NMIBC.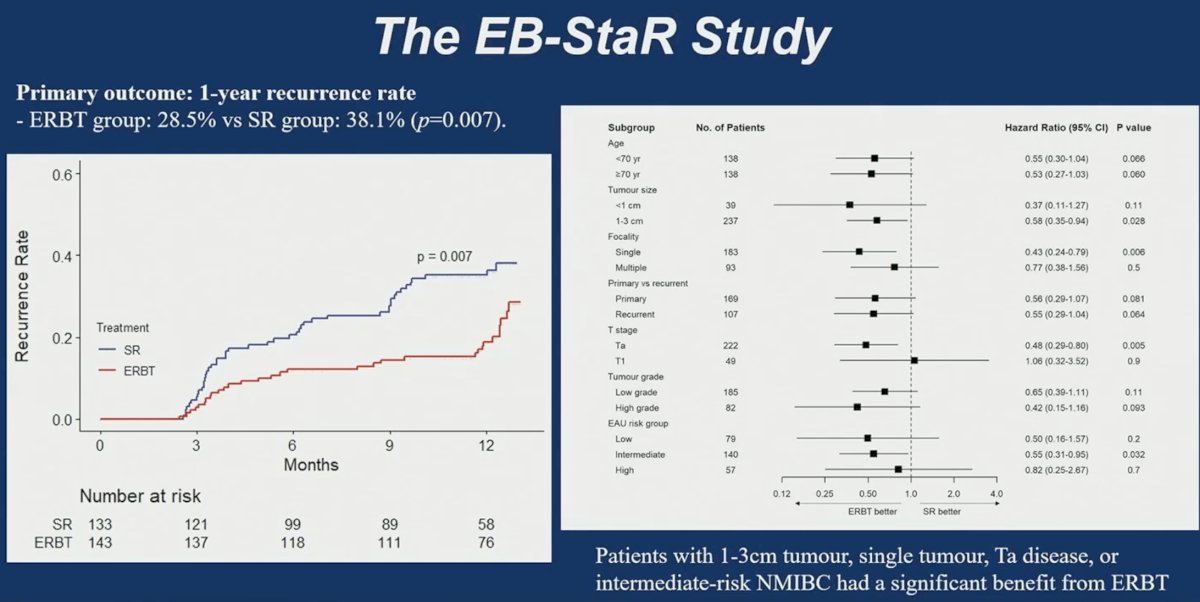
Additional analyses examined recurrence stratified by intravesical therapy use. Among patients who did not receive BCG, the 1-year recurrence rate was 40.8% after standard resection compared with 32.6% after ERBT. Among patients receiving BCG, recurrence rates were 26.3% with standard resection and 5% with ERBT, suggesting that high-quality tumor resection may enhance the effectiveness of adjuvant intravesical therapy.
The trial also evaluated secondary outcomes. The ERBT procedure required a longer operative time compared with standard resection (33.4 ± 18.5 minutes vs 24.7 ± 12.9 minutes, p < 0.001). However, there were no significant differences in detrusor muscle sampling rates, obturator reflex, postoperative bladder irrigation, mitomycin C administration, hospital stay, residual disease at second resection, upstaging, or 30-day complications.
Progression outcomes were also examined. The 1-year progression rate was 0% in the ERBT group compared with 2.6% in the standard resection group, although this difference did not reach statistical significance (p = 0.065).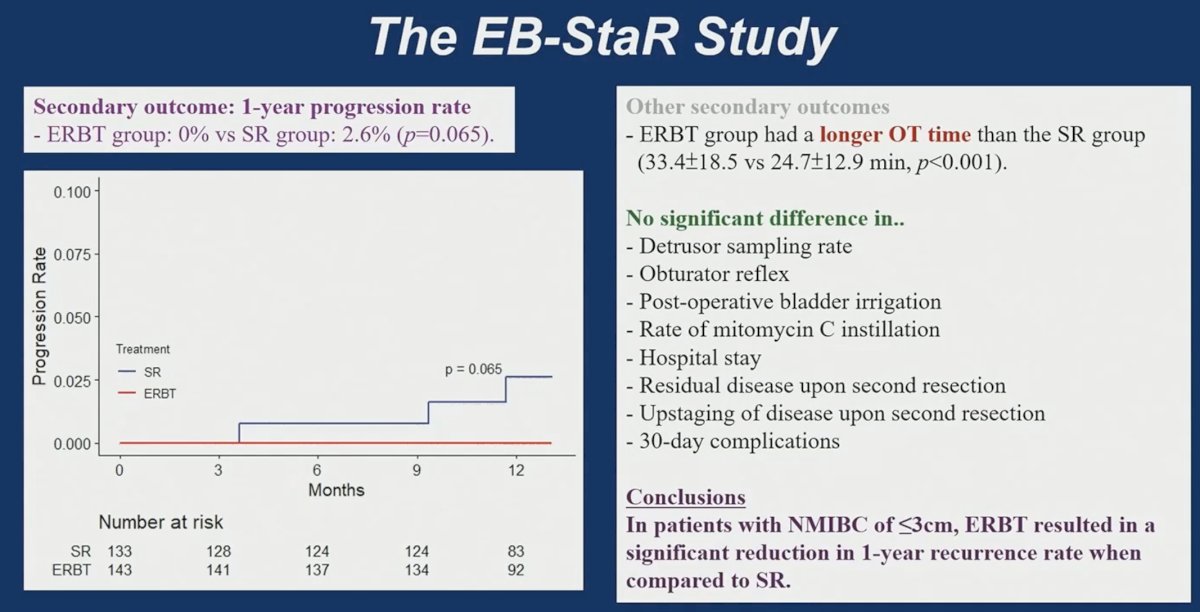
The mechanisms underlying recurrence in NMIBC can broadly be categorized into three pathways: residual disease following incomplete resection, tumor reimplantation due to intraoperative tumor cell dissemination, and the field change effect associated with underlying urothelial carcinogenesis.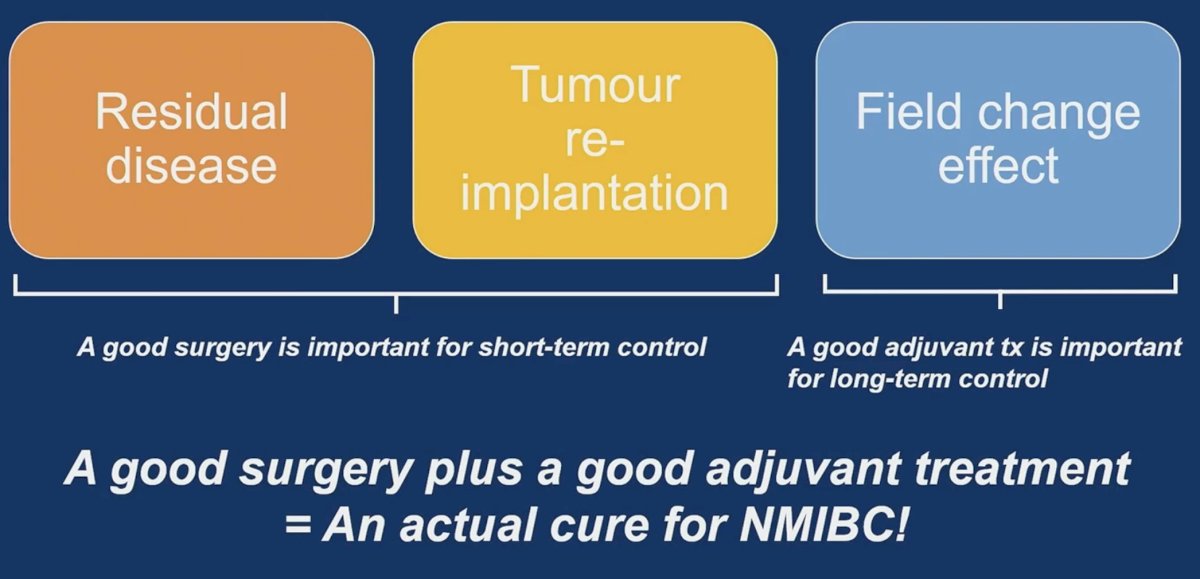
These mechanisms highlight the complementary roles of surgical quality and adjuvant therapy. Optimal surgery is essential for short-term disease control by eliminating residual disease and minimizing tumor seeding. Adjuvant intravesical therapies such as BCG are required for long-term control by addressing the underlying field cancerization process.
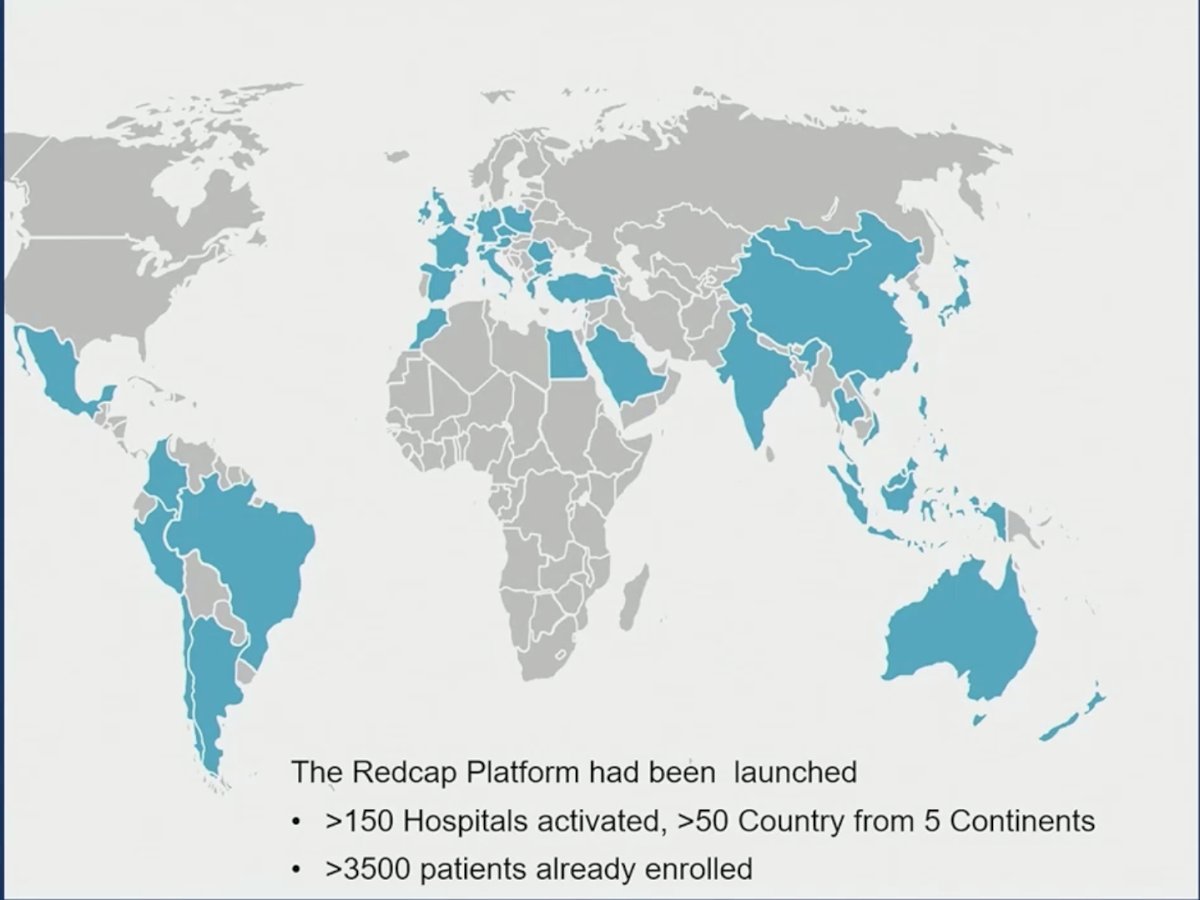
To better understand real-world implementation and outcomes of ERBT, a global registry has been established to collect prospective data on patients undergoing en bloc transurethral resection. The REDCap-based platform has already activated more than 150 hospitals across over 50 countries spanning five continents. More than 3,500 patients have already been enrolled in the registry. This initiative aims to generate large-scale real-world evidence regarding surgical outcomes, oncologic results, and patterns of ERBT adoption worldwide.

Technological innovation continues to expand the potential applications of ERBT. One emerging development is the Virtuoso Surgical robotic system, which utilizes patented concentric tube manipulators that enable robotic instruments at nearly one-tenth the scale of conventional robotic systems.
This platform is designed to enable highly precise endoscopic surgery through smaller access channels. The system aims to facilitate robotic en bloc resection of bladder tumors and potentially expand surgical capabilities within the bladder.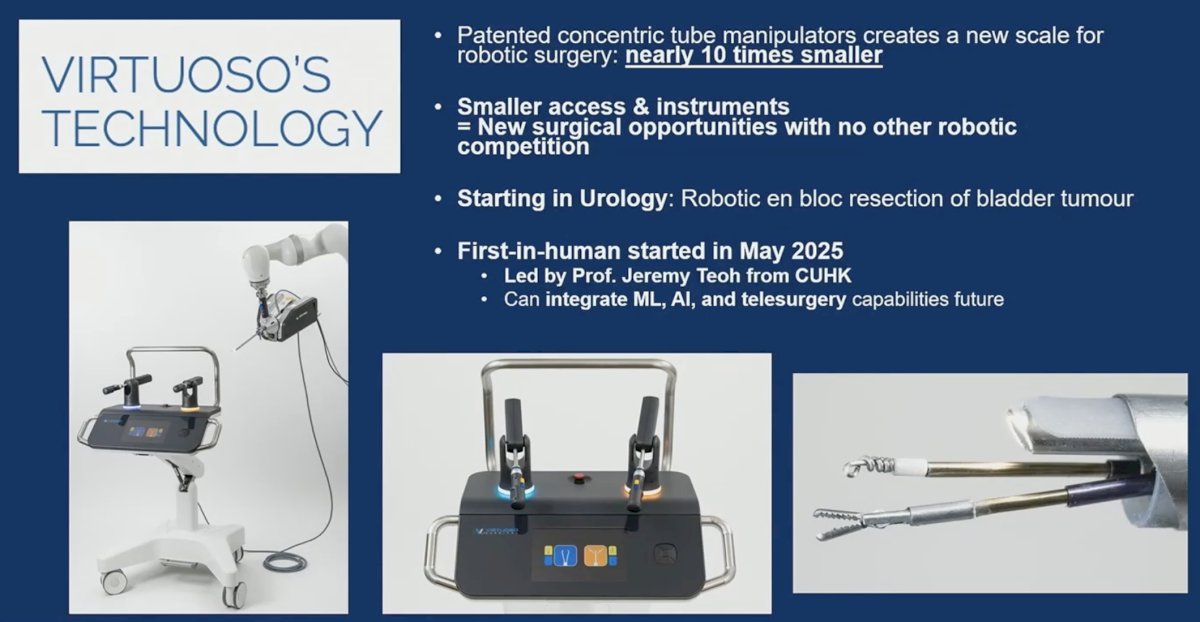
The initial human experience with this robotic platform was reported in the VIABLE trial. In the first phase of the study, six patients with a total of 12 tumors were treated.
The procedure achieved a 100% technical success rate and a 100% detrusor muscle sampling rate. All Ta and T1 tumors demonstrated negative resection margins. One patient with T2 disease had a clean resection bed endoscopically, a negative second-look TURBT, and was able to undergo bladder-sparing management.3

These results suggest that robotic en bloc resection is technically feasible and capable of achieving high-quality surgical specimens.
The Virtuoso system received FDA Breakthrough Device designation for bladder lesion removal via en bloc excision, recognizing its potential to significantly improve specimen quality and staging accuracy during bladder tumor surgery.
Dr. Teoh concluded as follows:
- Surgical quality during TURBT remains the most critical determinant of early oncologic control in NMIBC. En bloc resection represents a promising approach that may standardize the TURBT technique while adhering to core oncologic surgical principles.
- Randomized evidence from the EB-StaR trial demonstrates that ERBT can significantly reduce 1-year recurrence rates compared with conventional resection. When combined with intravesical therapy such as BCG, ERBT may further improve outcomes for patients with high-risk NMIBC.
- Emerging technologies, including robotic transurethral platforms, may further enhance surgical precision and facilitate broader adoption of ERBT techniques. Future studies exploring combinations of ERBT with novel intravesical or systemic therapies may further improve disease control and potentially move the field closer toward curative treatment for NMIBC.
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the 2026 ASCO GU Annual Symposium, San Francisco, CA, February 26th–28th, 2026
- Sylvester RJ, van der Meijden APM, Oosterlinck W, et al. Predicting recurrence and progression in individual patients with stage Ta T1 bladder cancer using EORTC risk tables: a combined analysis of 2596 patients from seven EORTC trials. Eur Urol. 2006;49:466-477.
- Teoh JYC, Cheng CH, Tsang CF, et al. Transurethral en bloc resection versus conventional transurethral resection of bladder tumour: a randomised, multicentre, phase 3 trial. Eur Urol. 2024;86(2):112-113.
- Teoh JYC, Bracco FM, Wong JHF, et al. A novel transurethral robotic platform for performing en bloc resection of bladder tumour: results from the first phase of the VIABLE trial. Eur Urol Oncol. 2026;9(1):111-115.