(UroToday.com) The 2026 ASCO GU Annual Symposium featured a prostate and urothelial cancers poster session. Dr. Zeynep Ozay presented a real-world analysis evaluating the use and effectiveness of first-line enfortumab vedotin plus pembrolizumab (EV+P) among patients with advanced urothelial carcinoma (aUC) in the United States.
Enfortumab vedotin plus pembrolizumab (EV+P) demonstrated a significant improvement in overall survival (OS) compared with platinum-based chemotherapy in the EV-302 trial.1 Based on these data, EV+P has become the new first-line standard-of-care treatment for patients with advanced urothelial carcinoma. Recent reports further suggest that EV+P has rapidly emerged as the most frequently used treatment in the first-line aUC setting.2 However, despite this rapid adoption, real-world data describing survival outcomes with EV+P remain limited.
To address this knowledge gap, the investigators evaluated the real-world use and effectiveness of first-line EV+P using a large US-based electronic health record dataset.
In this IRB-approved retrospective study, the US-based electronic health record–derived deidentified Flatiron Health Research Database was used to extract patient-level data. Eligible patients included those diagnosed with advanced urothelial carcinoma who received first-line treatment with EV+P. The analytic cohort included patients diagnosed with aUC between April 1, 2014, and June 23, 2025. Patients enrolled on clinical trials were excluded. The data cut-off date for the analysis was June 30, 2025.
Uptake of EV+P by year of first-line initiation was summarized using frequencies and percentages. Overall survival (OS) was defined as the time from initiation of first-line EV+P to death and censored at the last follow-up according to structured activities. Time to next therapy (TTNT) was defined as the time from initiation of first-line therapy to initiation of second-line therapy or death and censored at the last follow-up according to structured activities. The Kaplan–Meier method was used to estimate median OS and TTNT with corresponding 95% confidence intervals. All analyses were conducted using R version 4.2.3.
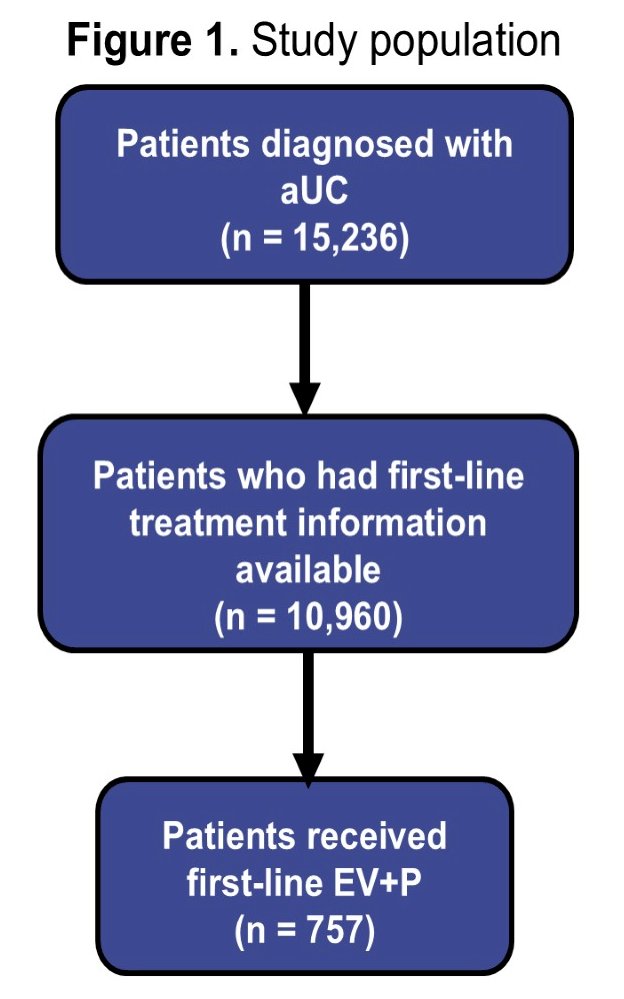
A total of 15,236 patients with advanced urothelial carcinoma were identified within the dataset, of whom 10,960 had information available regarding first-line treatment. Among these patients, 757 received first-line EV+P. The start date for first-line EV+P therapy ranged from February 28, 2020, to June 24, 2025.
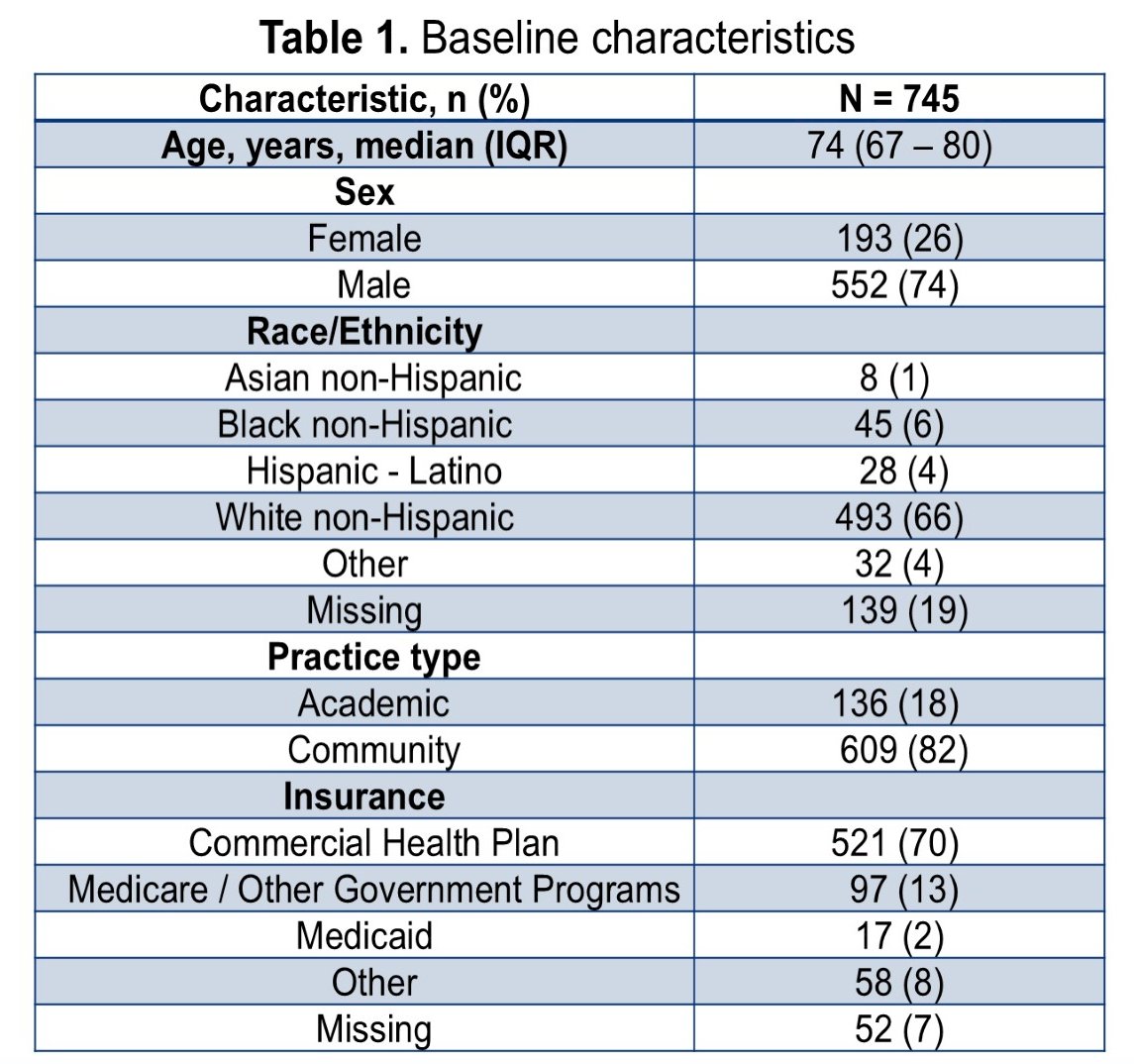
Baseline characteristics were reported for the 745 patients included in the effectiveness analyses. The median age was 74 years (interquartile range 67–80). The majority of patients were male (74%), while females comprised 26% of the cohort. With respect to race and ethnicity, most patients were White non-Hispanic (66%), followed by Hispanic/Latino (6%), Black non-Hispanic (6%), Asian non-Hispanic (1%), and other categories, with 19% missing race data.
Most patients were treated in community practice settings (82%), whereas 18% were managed at academic centers. Regarding insurance coverage, the majority of patients had commercial health plans (70%), followed by Medicare or other government programs (13%), Medicaid (2%), and other insurance types (8%), with 7% missing insurance data.
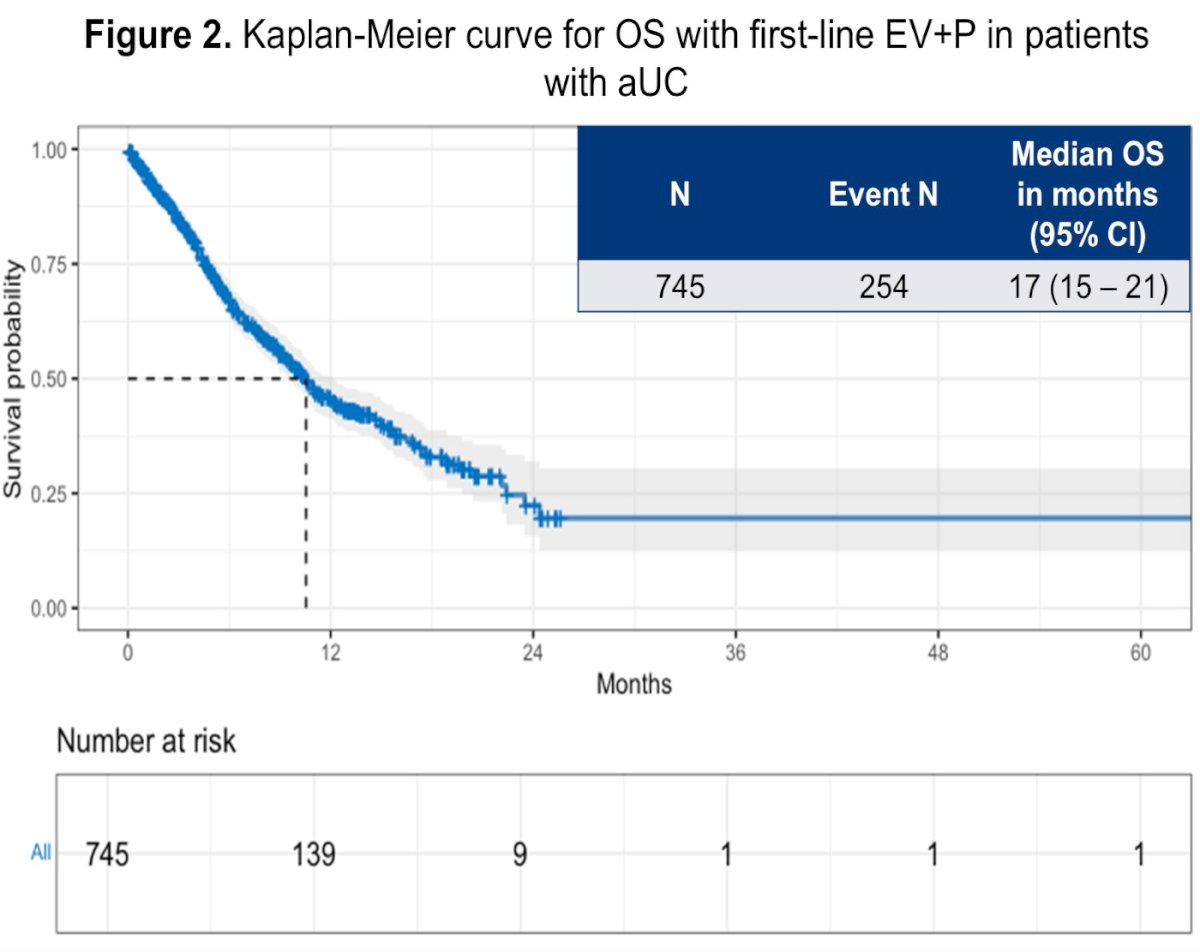
At a median follow-up of 10.3 months, 254 patients (34%) had died. The Kaplan–Meier analysis demonstrated a median overall survival of 17 months (95% CI 15–21 months) among patients treated with first-line EV+P. The corresponding Kaplan–Meier survival curve demonstrated a rapid early decline in survival probability during the first year after treatment initiation, followed by a more gradual plateau thereafter.
Time-to-next-therapy outcomes were also evaluated. The median TTNT was 11 months (95% CI 9.5–12 months), with 328 events observed (44%). The Kaplan–Meier TTNT curve demonstrated a similar early decline, reflecting transition to subsequent therapy or death within the first year of treatment for a substantial proportion of patients.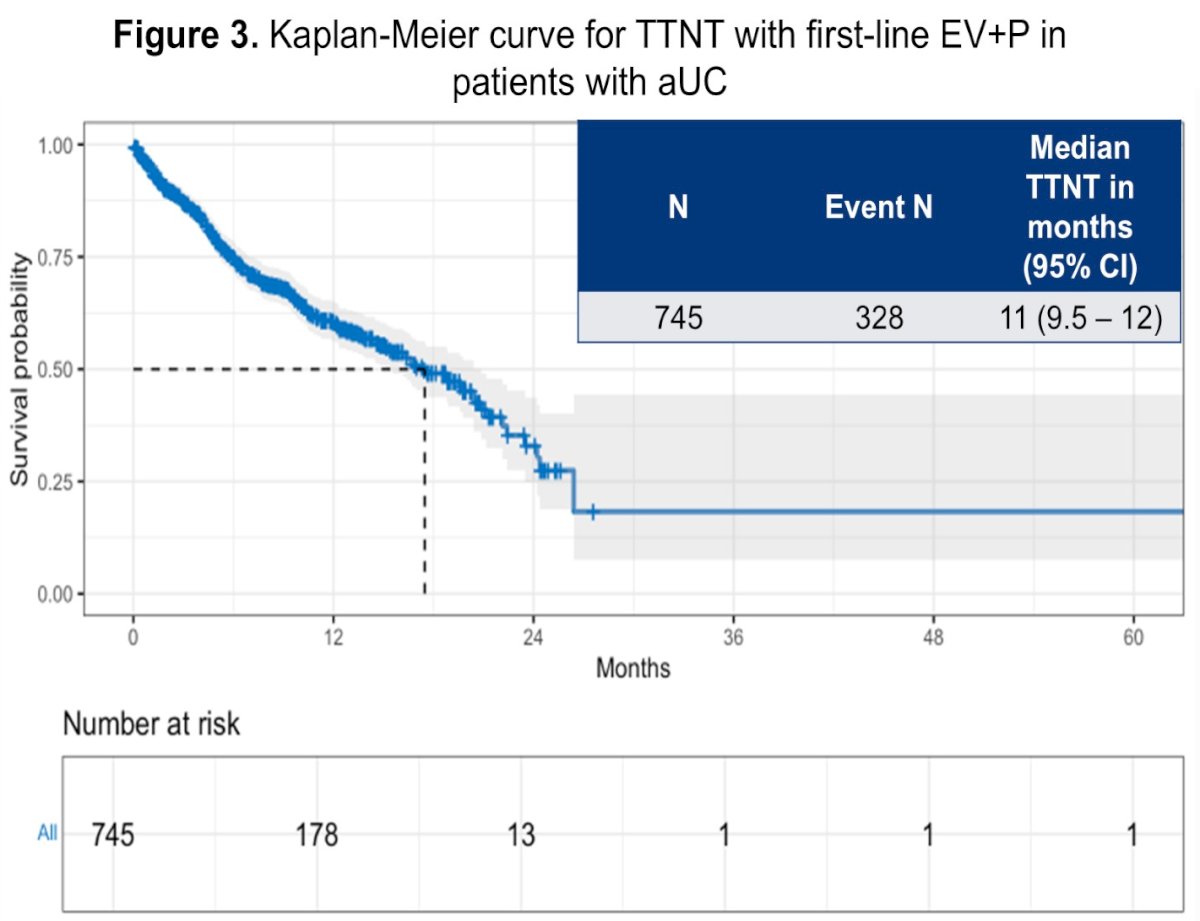
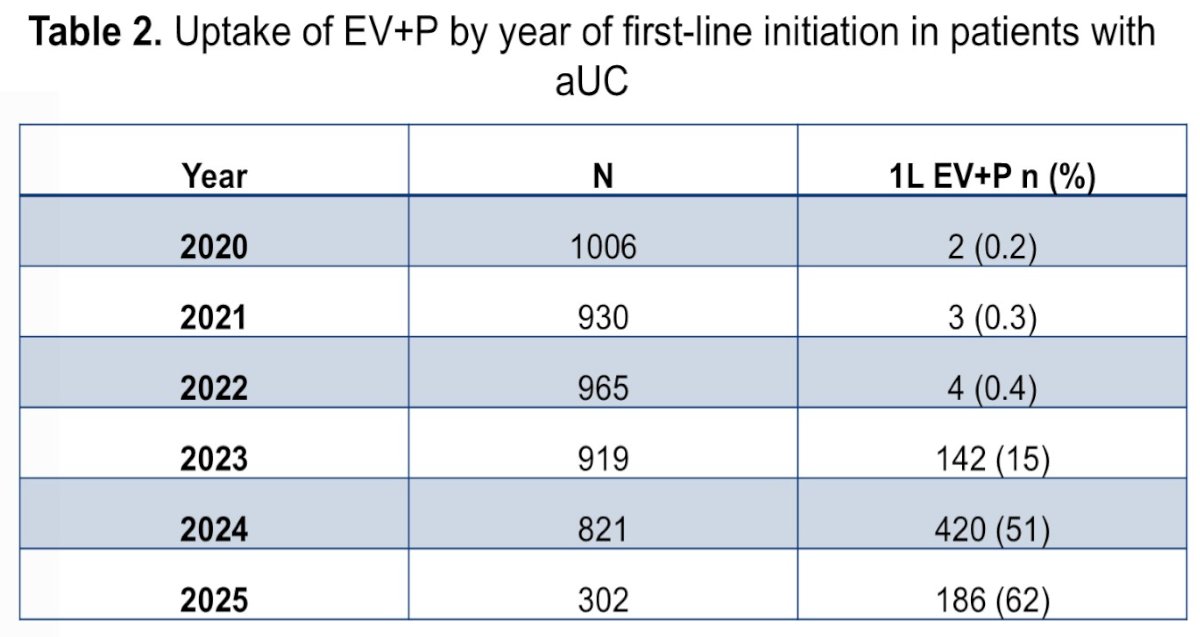
The investigators also evaluated temporal trends in the uptake of EV+P over time. Uptake increased substantially between 2020 and 2025. In 2020, only 2 of 1,006 patients (0.2%) received EV+P as first-line therapy. Use remained limited in 2021 (0.3%) and 2022 (0.4%), but increased sharply beginning in 2023. In that year, 142 of 919 patients (15%) received EV+P. Uptake continued to expand in 2024, when 420 of 821 patients (51%) received EV+P as first-line treatment. By 2025, EV+P accounted for 62% of all first-line therapies in the dataset, highlighting the rapid adoption of this regimen into routine clinical practice.
Overall, these findings represent the largest real-world analysis to date evaluating uptake and survival outcomes associated with EV+P in patients with advanced urothelial carcinoma in the United States. The results demonstrate substantial and rapidly increasing use of EV+P in clinical practice, with real-world overall survival outcomes that appear consistent with previously reported data.
The authors note several limitations, including the retrospective design of the analysis, lack of treatment information in neoadjuvant and adjuvant settings, and relatively short follow-up time. Despite these limitations, the study provides important early real-world evidence regarding outcomes with EV+P and highlights the rapid integration of this regimen into contemporary treatment paradigms for advanced urothelial carcinoma.
Presented by: Zeynep Irem Ozay, MD, Postdoctoral Research Fellow, Huntsman Cancer Institute at the University of Utah, Salt Lake City, UT
- Powles T, Valderrama BP, Gupta S, et al. Enfortumab vedotin and pembrolizumab in untreated advanced urothelial cancer. N Engl J Med. 2024;390(10):875-888.
- Mamtani R, Ulloa-Pérez E, Parikh RB, et al. Real-world uptake of enfortumab vedotin plus pembrolizumab after US Food and Drug Administration approval among patients with advanced urothelial cancer. Eur Urol. 2024;86(5):474-476.