(UroToday.com) The 2026 ASCO GU Annual Symposium featured a prostate and urothelial cancers poster session. Dr. Elise Cai presented an analysis from the UNITE dataset evaluating outcomes with enfortumab vedotin plus pembrolizumab (EV+P) in patients with advanced urothelial carcinoma and FGFR3 alterations.
EV+P is the preferred 1st line therapy for patients with unresectable locally advanced or metastatic urothelial cancer (aUC). EV+P has also emerged as the preferred perioperative therapy for resectable UC. FGFR3 pathogenic alterations are found in 15–20% of patients with aUC. The FGFR inhibitor erdafitinib is approved as subsequent line therapy for aUC patients, and FGFR3 inhibitor + EV+P combination therapy is currently under investigation (NCT07218380). Outcomes of EV+P treatment in aUC patients with FGFR3 alterations are unknown.
To address this question, Dr. Cai and colleagues performed an analysis using the UNITE dataset, a multicenter retrospective study of real-world outcomes in patients with advanced urothelial carcinoma receiving targeted therapies. A total of 521 aUC patients treated with EV+P across 16 U.S. centers were identified, of whom 313 patients underwent genomic profiling and were included in this study.
Patients were categorized according to FGFR3 alteration status and evaluated for outcomes following first-line (1L) and subsequent-line (2L+) EV+P therapy. Statistical analyses included χ² testing and logistic regression to assess observed response rate (ORR) and disease control rate (DCR). Time-to-event outcomes—including duration of response (DOR), progression-free survival (PFS), and overall survival (OS)—were evaluated using log-rank testing and Cox proportional hazards models measured from initiation of EV+P therapy.
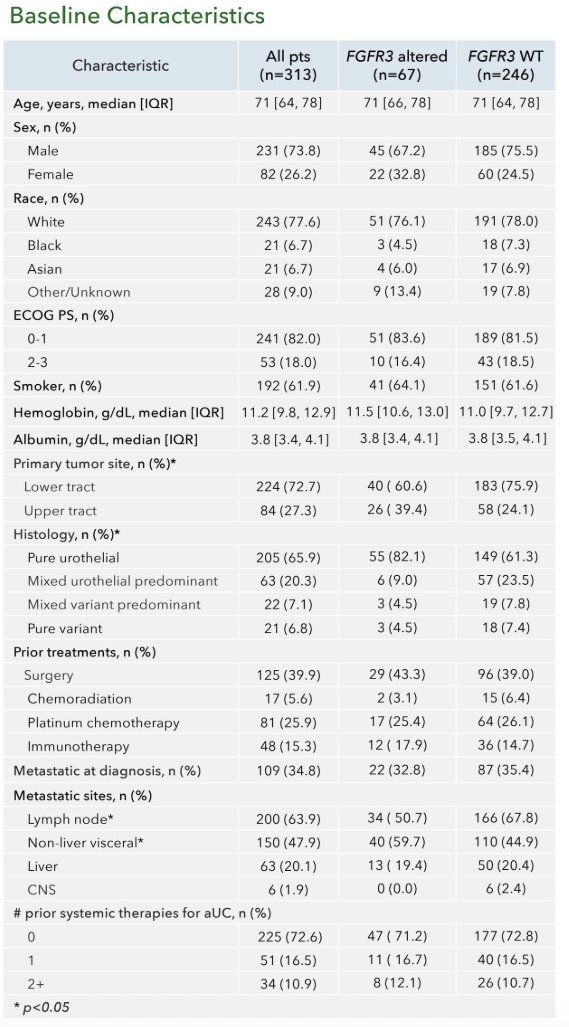
Baseline characteristics of the cohort are summarized in Table 1. Among the 313 included patients, 67 (21%) had FGFR3-altered tumors, while 246 (79%) were FGFR3 wild-type. The median age of the cohort was 71 years (IQR 64–78), with similar age distributions between groups. Approximately 74% of the cohort were male. Most patients had an ECOG performance status of 0–1 (82%). Primary tumor location differed modestly between groups, with a greater proportion of lower tract tumors among FGFR3 wild-type patients (75.9% vs 60.6%), while upper tract primaries were more common among FGFR3-altered cases (39.4% vs 24.1%).
Regarding histologic subtype, the majority of tumors were pure urothelial carcinoma (65.9% overall), with mixed histologies observed in smaller proportions. Prior treatments included surgery (39.9%), platinum chemotherapy (25.9%), and immunotherapy (15.3%). At diagnosis, approximately one-third of patients had metastatic disease (34.8%), with lymph node metastases being the most common metastatic site (63.9%).
Treatment outcomes were evaluated according to FGFR3 status. The overall response rate across the entire cohort was 52.8%. Response rates were similar between patients with FGFR3 alterations (52.6%) and those with FGFR3 wild-type tumors (52.8%). Disease control rates were likewise comparable (89.5% vs 79.9%).
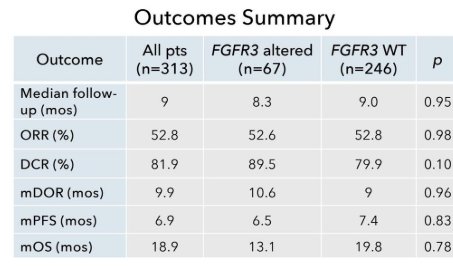
Median duration of response was 9.9 months overall, with similar outcomes in the FGFR3-altered and wild-type cohorts (10.6 vs 9.8 months). Median progression-free survival was 6.9 months overall, with a median PFS of 6.5 months in the FGFR3-altered group compared with 7.4 months among FGFR3 wild-type patients. Median overall survival for the entire cohort was 18.9 months, with a median OS of 13.1 months in patients with FGFR3 alterations and 19.8 months among FGFR3 wild-type tumors.
Kaplan–Meier analyses for duration of response, progression-free survival, and overall survival demonstrated overlapping curves between FGFR3-altered and wild-type cohorts, consistent with the absence of statistically significant differences between groups.

Additional analyses evaluated outcomes by line of EV+P therapy and by FGFR3 alteration subtype. When stratified by treatment line, both first-line and later-line EV+P therapy demonstrated similar response and survival outcomes between FGFR3-altered and wild-type groups. For example, the odds ratio for response comparing FGFR3-altered versus wild-type tumors was 0.99 (95% CI 0.6–1.8; p=0.98). No significant differences were observed in disease control rate, duration of response, PFS, or OS.
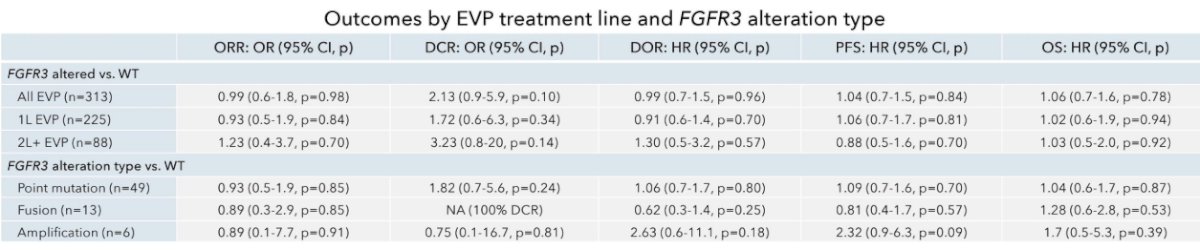
Further subgroup analyses evaluated specific FGFR3 alteration types, including point mutations, fusions, and amplifications. Again, no statistically significant differences in outcomes were observed relative to FGFR3 wild-type tumors across these subgroups.
A cohort overview visualization demonstrated the distribution of genomic alterations, tumor sites, prior therapies, and histologic subtypes across the study population, illustrating the heterogeneity of patients included in this real-world dataset.

Overall, the investigators concluded that patients with advanced urothelial carcinoma harboring FGFR3 alterations who received first- or subsequent-line EV+P experienced treatment outcomes comparable to those observed among patients with FGFR3 wild-type tumors. The authors noted that the retrospective nature of the analysis, the relatively small sample size of patients with FGFR3 alterations, and limited follow-up represent important limitations, and external validation in larger cohorts will be required.
Presented by: Elise Y. Cai, MD, PhD, Hematology and Medical Oncology Fellow, Department of Medicine, University of California, San Francisco, CA, USA
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026.