(UroToday.com) The 2026 ASCO GU Annual Symposium was host to a non-muscle invasive bladder cancer (NMIBC) session. Dr. Robert Svatek presented the late-breaking abstract from SWOG S1602, a phase III randomized trial evaluating BCG strain differences and priming with intradermal BCG before intravesical therapy for BCG-naïve, high-grade NMIBC.
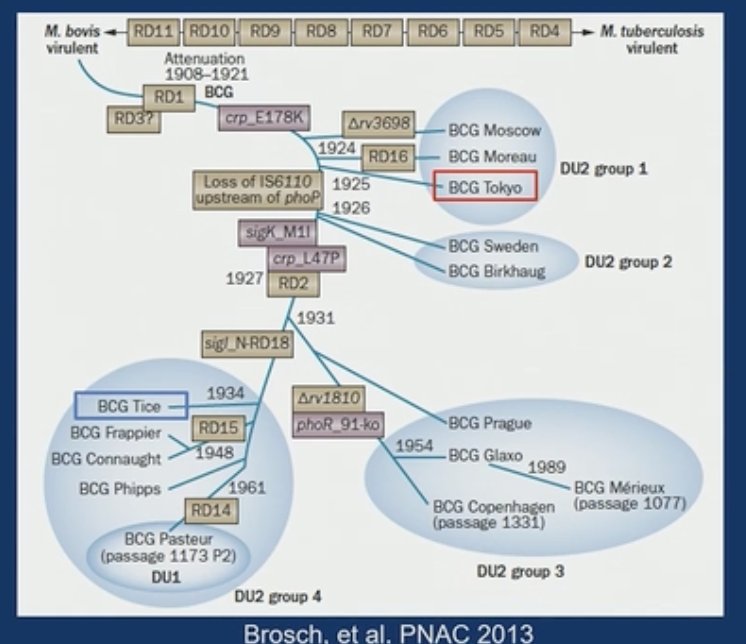
Dr. Svatek highlighted that there are various BCG strains available worldwide; however, only the TICE strain is currently approved in the United States. Given the current shortage of BCG in the United States, there is a clear need to evaluate additional potential candidate strains. These strains differ in their genealogy, which has important immunologic implications that may impact cancer response rates.1
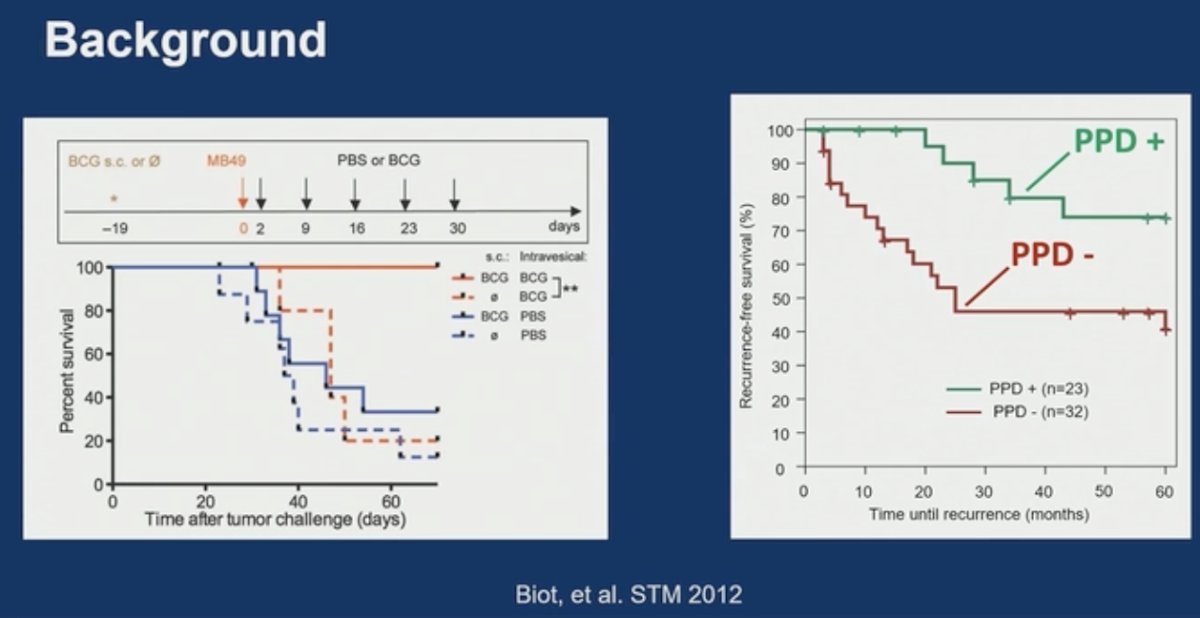
Additionally, data suggest that ‘priming’ mouse models, and later patients, with intradermal BCG may enhance systemic immunity responses and the recruitment of T-cells into the bladder, leading to improved responses to BCG.2
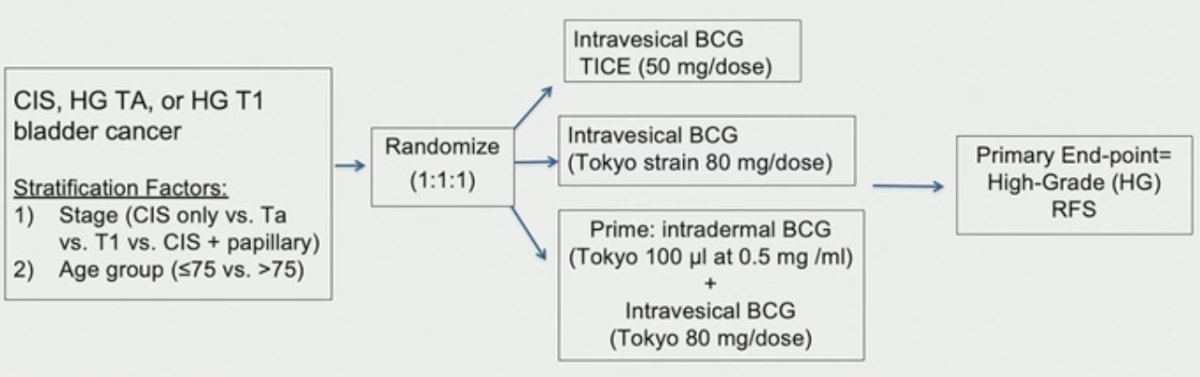
The study schema of SWOG S1602 is illustrated below. This study has two aims and three arms.
Eligible patients with CIS, HG Ta, or HG T1 bladder cancer underwent 1:1:1 randomization to:
- Intravesical BCG TICE strain
- Intravesical BCG Tokyo strain
- Priming with intradermal BCG (Tokyo strain) + intravesical BCG (Tokyo)
The primary endpoint was high-grade recurrence-free survival (HG-RFS).
The study objectives were as follows:
- Test the non-inferiority of the TOKYO strain versus the TICE strain
- Non-inferiority margin: 1.34 (1-year HG-RFS: 68% versus 75%)
- Test the superiority of priming
- Alternative HR is 1.40 (1-year HG-RFS: 75% versus 81%)
The treatment schedules were as follows:
- BCG: Induction (6 weekly) + maintenance (3 weekly) at 3, 6, 12, 18, 24, 30, and 36 months
- Prime: Intradermal BCG 21 days prior to intravesical BCG
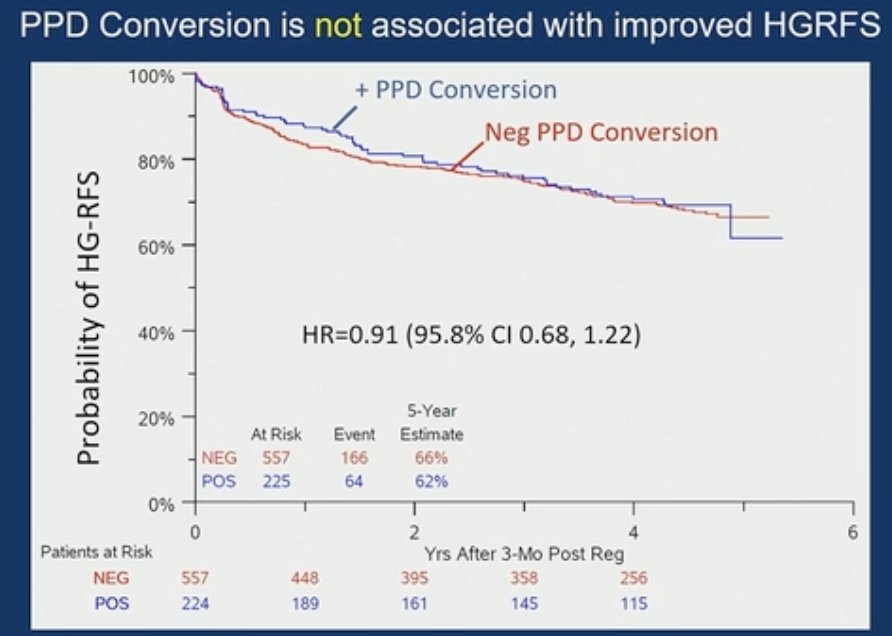
Given the suggested association between improved outcomes with BCG and conversion from PPD(-) to PPD(+) following intravesical BCG, the study investigators evaluated the prognostic significance of PPD conversion at 3 and 6 months.
The target sample size was 924 (308 per arm), powered at 84%, with planned follow-up for 5 years.
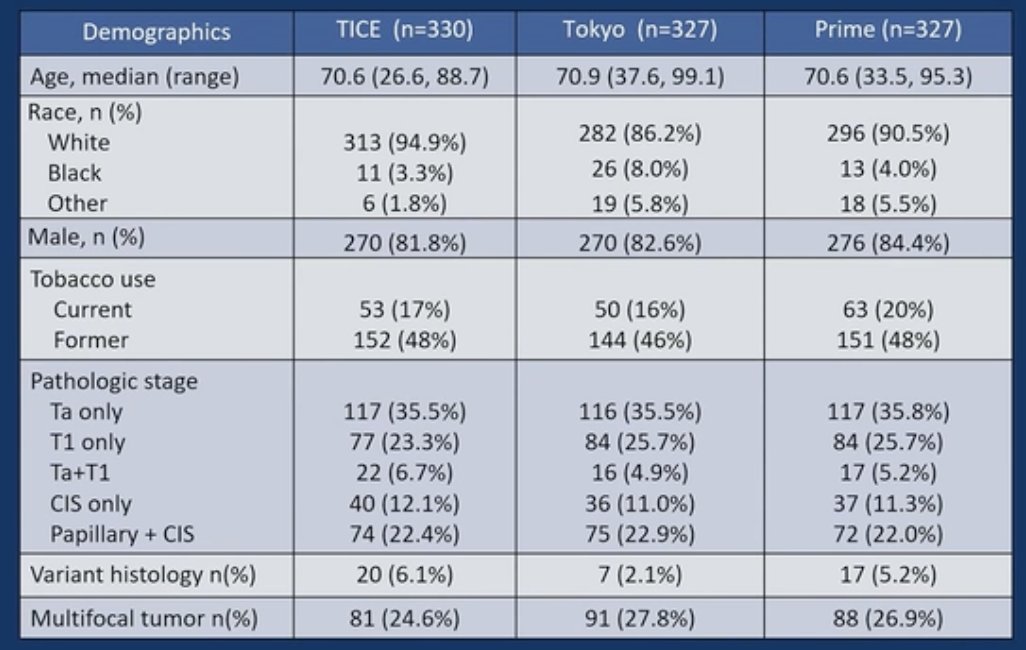
The baseline patient characteristics by treatment arm are summarized in the table below. The median age was approximately 70 years. 82-84% were male. Approximately 1/3 of patients had CIS disease, and 36% had Ta-only disease. Of note, patients with micropapillary disease were excluded.
Overall, 96-98% of patients completed induction therapy. Maintenance therapy for >1 year was completed by 36-48% of patients, and ≤1 year maintenance by 34-49%.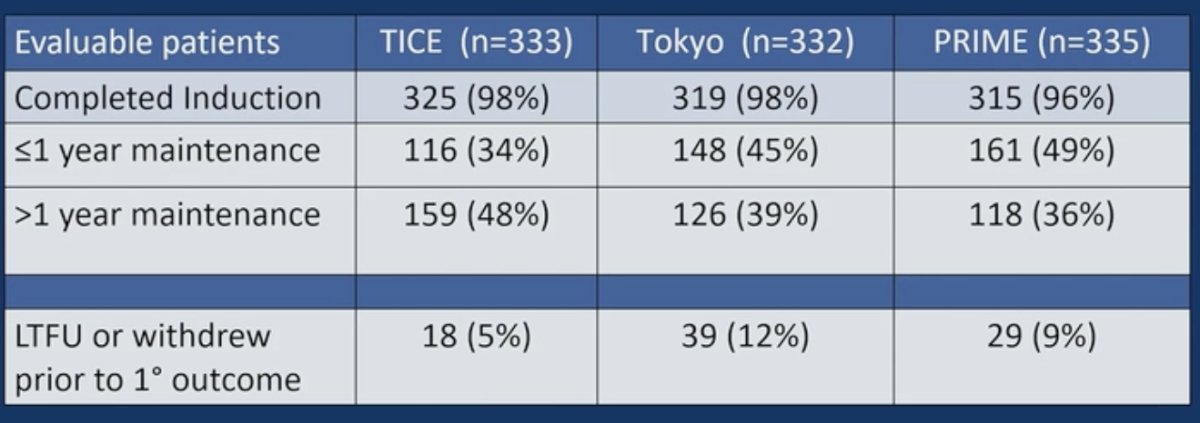
In the overall cohort, the Tokyo strain was shown to be non-inferior to TICE (HR for HG-RFS: 0.82, 95.8% CI: 0.63–1.08).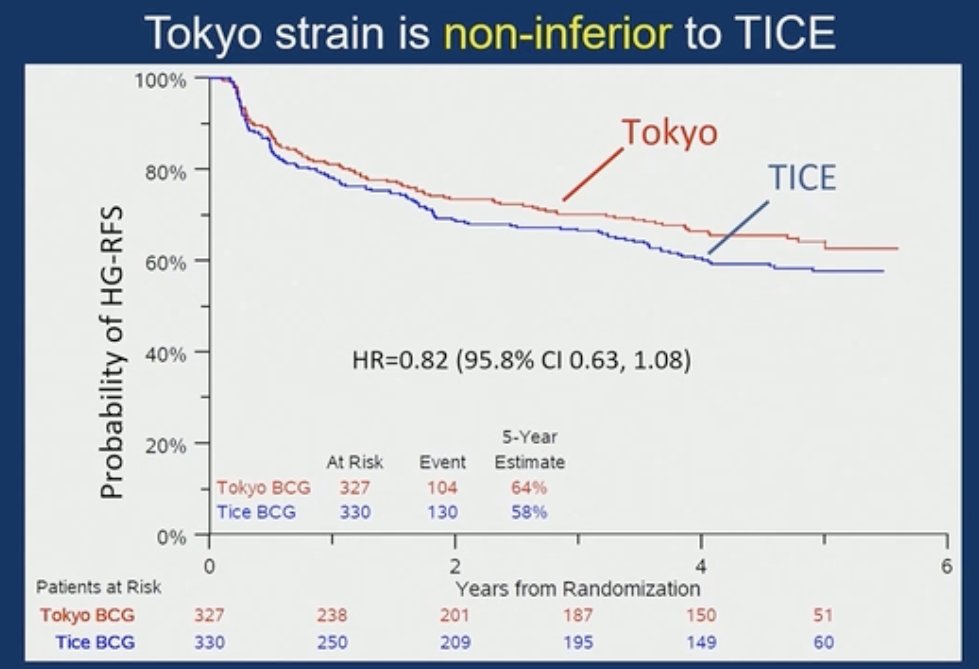
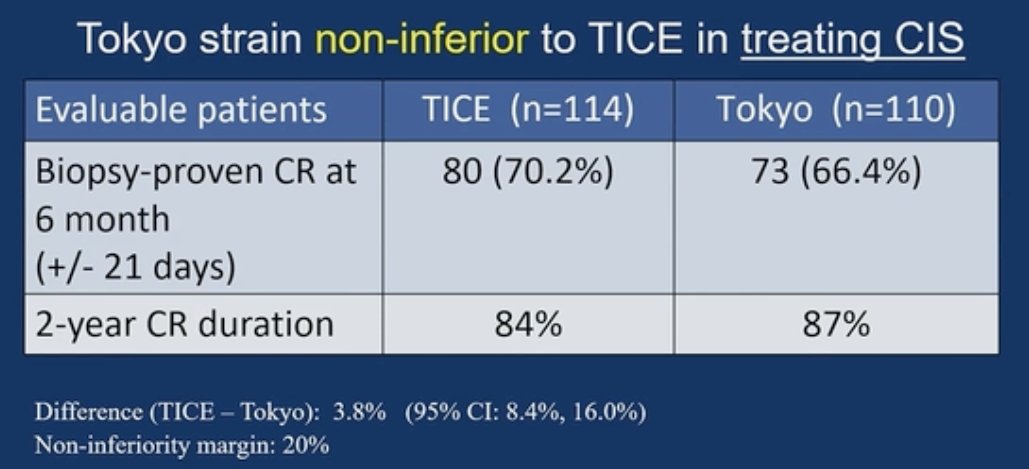
This held for the sub-group comparison of CIS +/- papillary patients, with TICE similarly shown to be non-inferior for:
- Biopsy-proven complete response at 6 months: 70.2% (TICE) versus 66.4% (Tokyo)
- 2-year complete response duration: 84% versus 87%
With regards to adverse events (AEs), Dr. Svatek noted that there were no Grade 5 AEs in either arm. Grade 3 AEs were more prevalent in the Tokyo arm (11% versus 5%). The vast majority of side effects were localized to the bladder (hematuria, urgency, frequency).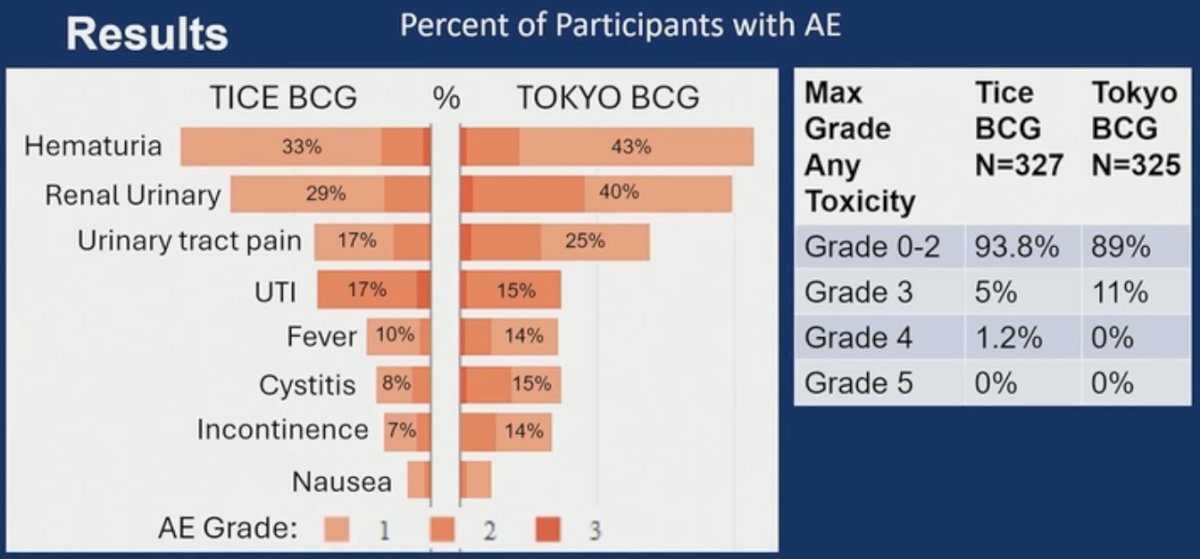
Discussing patient-reported outcomes in this trial, Dr. Svatek noted that the Bladder Cancer Index urinary domain scores were assessed at 6 months. TICE was noted to have a 3.7-point higher score, corresponding to improved urinary quality of life. However, given that commonly estimated thresholds for minimally important differences (MID) are referenced at 5-10 points, the study investigators concluded that this difference is of limited clinical relevance.
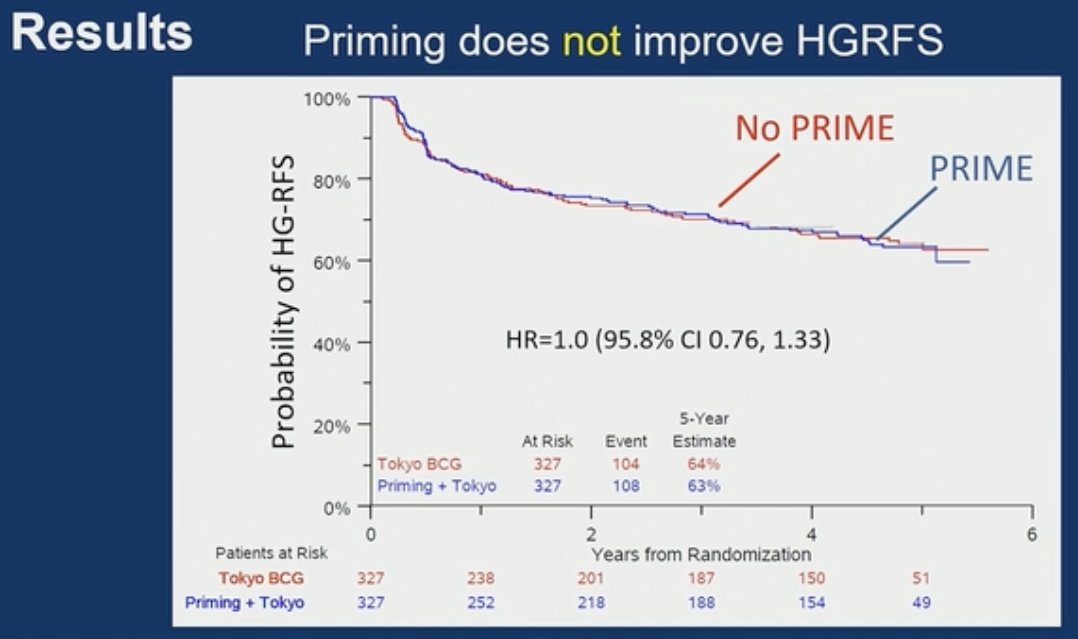
Moving on to the second objective of the trial, Dr. Svatek noted that priming does not improve HG-RFS outcomes in the overall cohort (HR 1.0, 95.8% CI: 0.76–1.33):
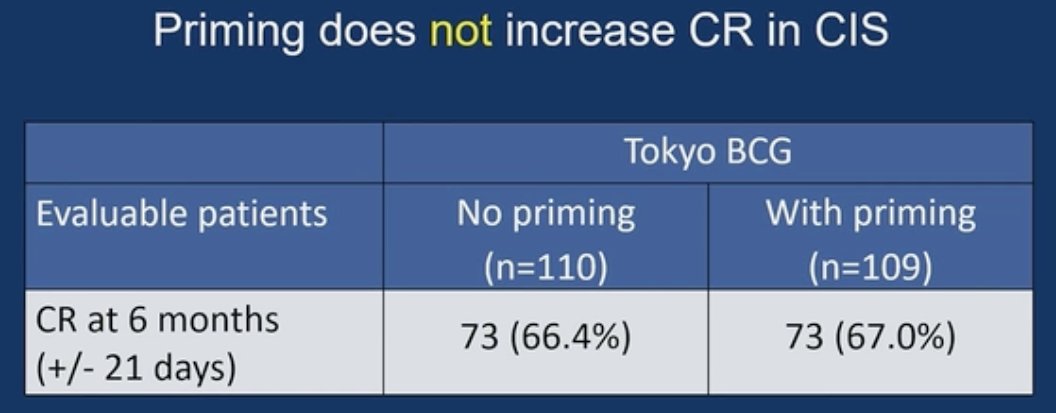
This held true in the CIS subgroup of patients, where priming was not found to increase complete response rates.
PPD conversion was noted to be higher with Tokyo (33%) versus TICE BCG treatment (22%). Notably, Tokyo priming did not increase PPD conversion compared to intravesical instillations alone (32% versus 33%).

The clinical relevance of this remains unclear, given that PPD conversion was not associated with improved HG-RFS.
Dr. Svatek concluded his presentation as follows:
- Tokyo BCG is non-inferior to TICE BCG
- BCG shortage could be mitigated with Tokyo BCG
- Compared to TICE, Tokyo had slightly higher bother and Grade ≥3 AEs
- Priming does not improve outcomes
- PPD conversion is infrequent (~30%) and does not correlate with response
Presented by: Robert S. Svatek, MD, Professor and Chair, Gary and Glenda Woods President’s Distinguished University Chair in GU Oncology, Department of Urology, UT Health San Antonio, TX
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the 2026 ASCO GU Annual Symposium, San Francisco, CA, February 26th–28th, 2026
Related content: Phase III Trial Compares BCG Strains and Priming in Non-Muscle-Invasive Bladder Cancer - Robert Svatek
- Brosch R, Gordon SV, Garnier T, et al. Genome plasticity of BCG and impact on vaccine efficacy. Proc Natl Acad Sci USA. 2013;110(2):426-431.
- Biot C, Rentsch CA, Gsponer JR, et al. Preexisting BCG-specific T cells improve intravesical immunotherapy for bladder cancer. Sci Transl Med. 2012;4(137):137ra72.