(UroToday.com) The 2026 GU ASCO annual meeting featured a urothelial carcinoma session and a presentation by Dr. Jonathan F. Anker discussing results of HCRN GU 20-444, a phase 2 trial of pembrolizumab with response-guided bladder-sparing in patients with muscle-invasive bladder cancer.
Many patients with muscle-invasive bladder cancer are not candidates for radical cystectomy and/or favor bladder-sparing alternatives. Neoadjuvant chemotherapy following TURBT leads to a pathologic complete response in a subset of patients, suggesting that radical cystectomy is not universally required to achieve cure. Dr. Anker and colleagues previously showed that TURBT followed by cisplatin-based neoadjuvant chemotherapy plus PD-1 blockade yielded a stringently defined clinical complete response in 43% of patients, and ~2/3 of such patients, omitting upfront radical cystectomy, experienced durable bladder-intact survival.1 However, ~50% of patients with muscle-invasive bladder cancer are ineligible for cisplatin, and neoadjuvant PD-1 blockade monotherapy can produce pathologic complete response rates of 30-40%. HCRN GU 20-444 evaluated TURBT followed by pembrolizumab monotherapy with response-guided bladder-sparing for patients with muscle-invasive bladder cancer.
Eligible patients had cT2-3N0M0 urothelial cancer and were cisplatin-declining or ineligible. Following maximal TURBT, patients received 2 cycles of pembrolizumab (q6 week dosing) followed by clinical restaging with MRI/CT, urine cytology, and cystoscopy with biopsies. Patients with a clinical complete response omitted definitive local therapy and received up to 7 additional cycles of pembrolizumab. Patients without a clinical complete response received definitive local therapy (radical cystectomy or chemoradiation):
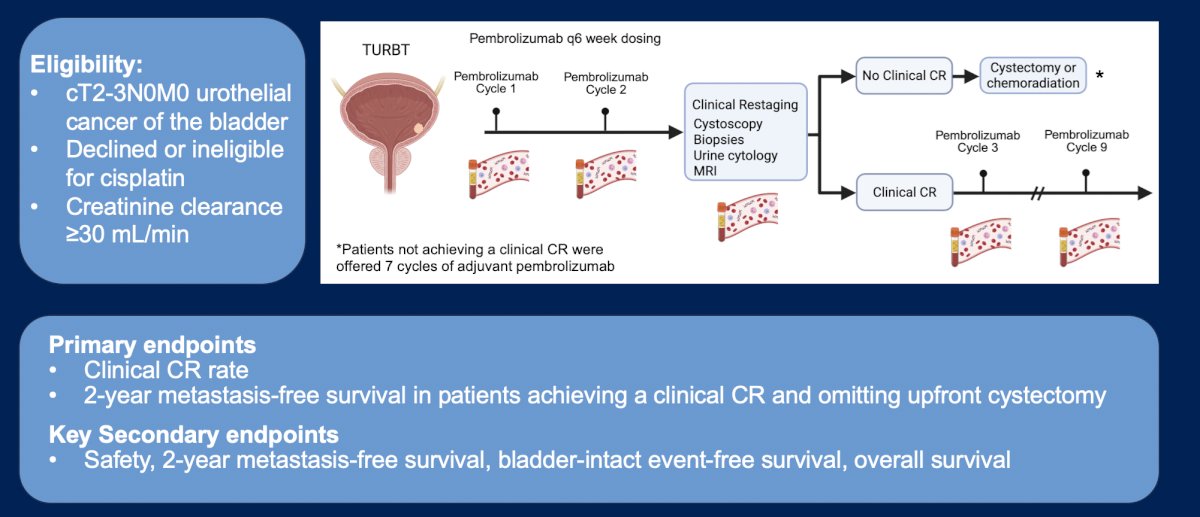
ctDNA was serially evaluated through whole genome sequencing of tumor and plasma coupled with artificial intelligence-based pattern recognition for ultrasensitive detection of residual disease (TrueMRD, Veracyte). The primary endpoint was the clinical complete response rate. Key secondary and exploratory endpoints included 2-year metastasis-free survival, overall survival, and ctDNA status.
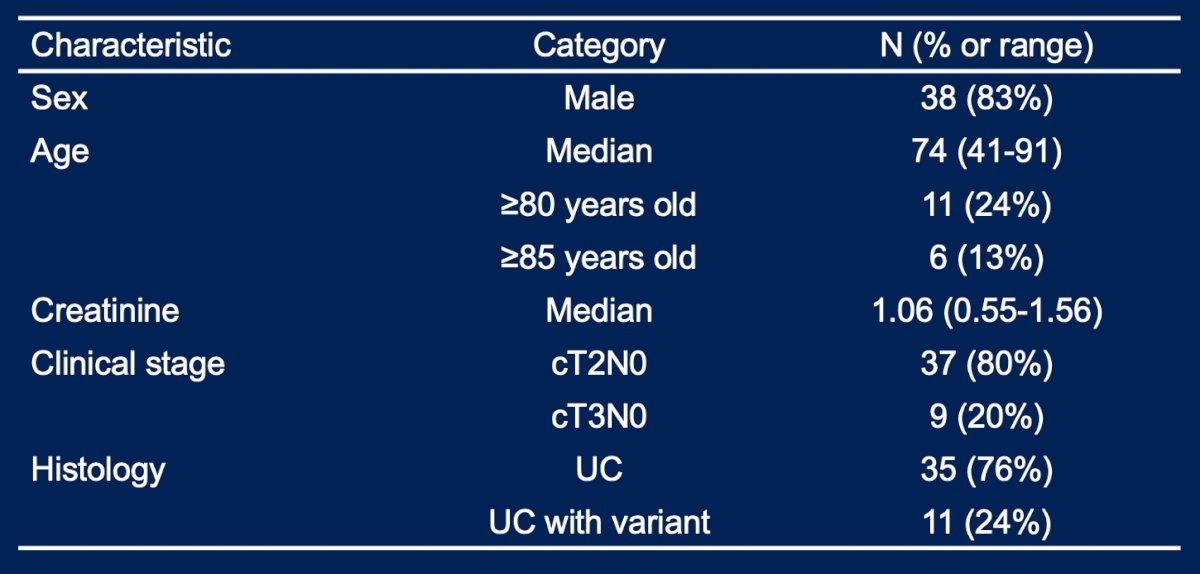
From July 2022 to December 2024, 46 patients were enrolled with a median age of 74 years (range: 41-91; 24% were ≥80):
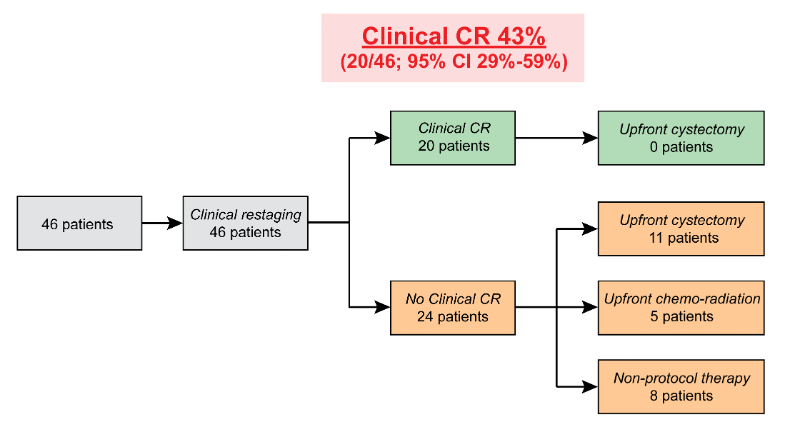
The median follow-up was 11 months (range: 2.4-33.5), with a clinical complete response achieved in 43% (95% CI 29%-59%) of patients. Among patients achieving a clinical complete response, all proceeded without upfront radical cystectomy, and none developed metastatic disease; 1/20 had a delayed cystoprostatectomy due to a new prostate cancer (bladder cancer pT0N0), and 2/20 died due to non-cancer causes:
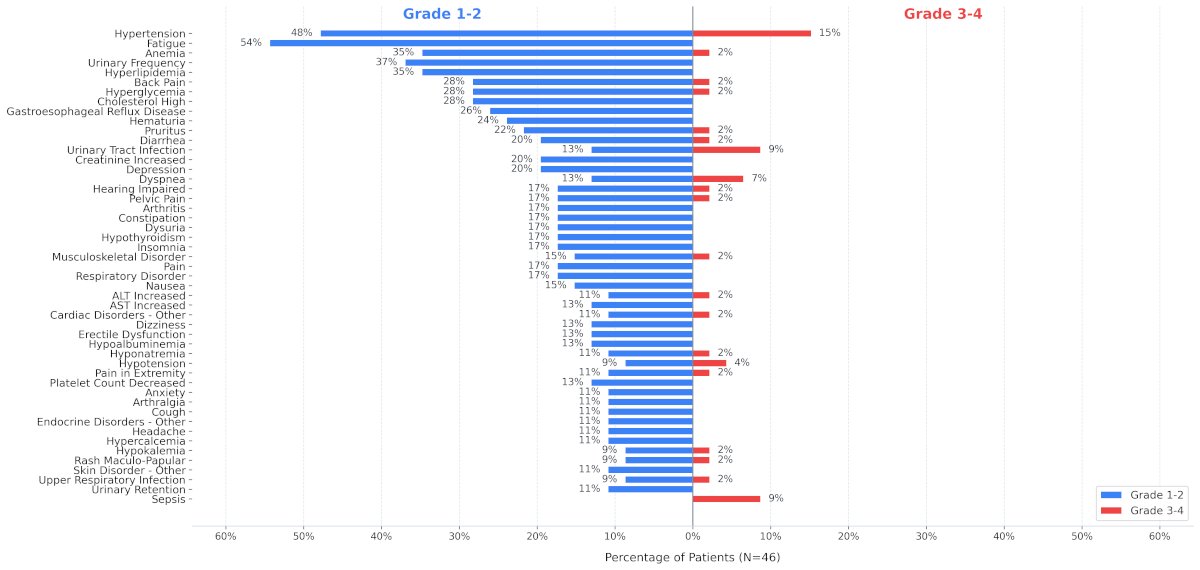
Adverse events were consistent with the toxicity profile of pembrolizumab:
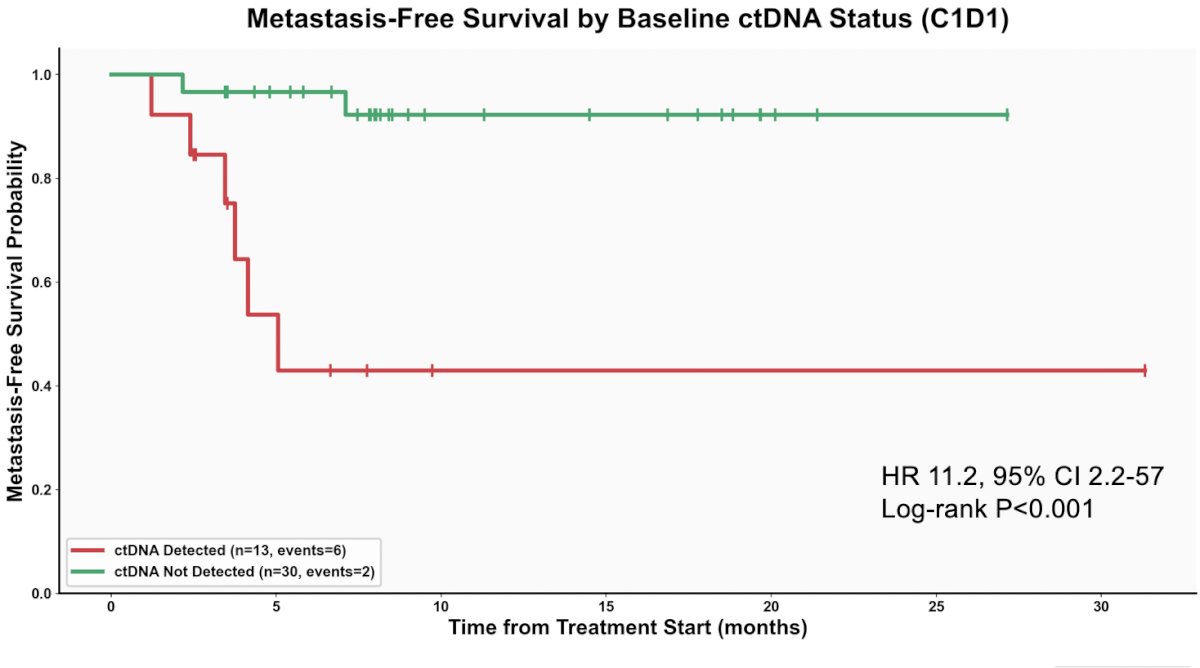
Cycle 1 ctDNA was undetectable in 90% and 55% of patients with and without a clinical complete response, respectively (Mann-Whitney p = 0.01). Undetectable cycle 1 ctDNA was associated with improved metastasis-free survival (HR 11.2, 95% CI 2.2-57, log-rank p = 0.0003) and overall survival (HR 11.4, 95% CI 1.3-103, p = 0.007):
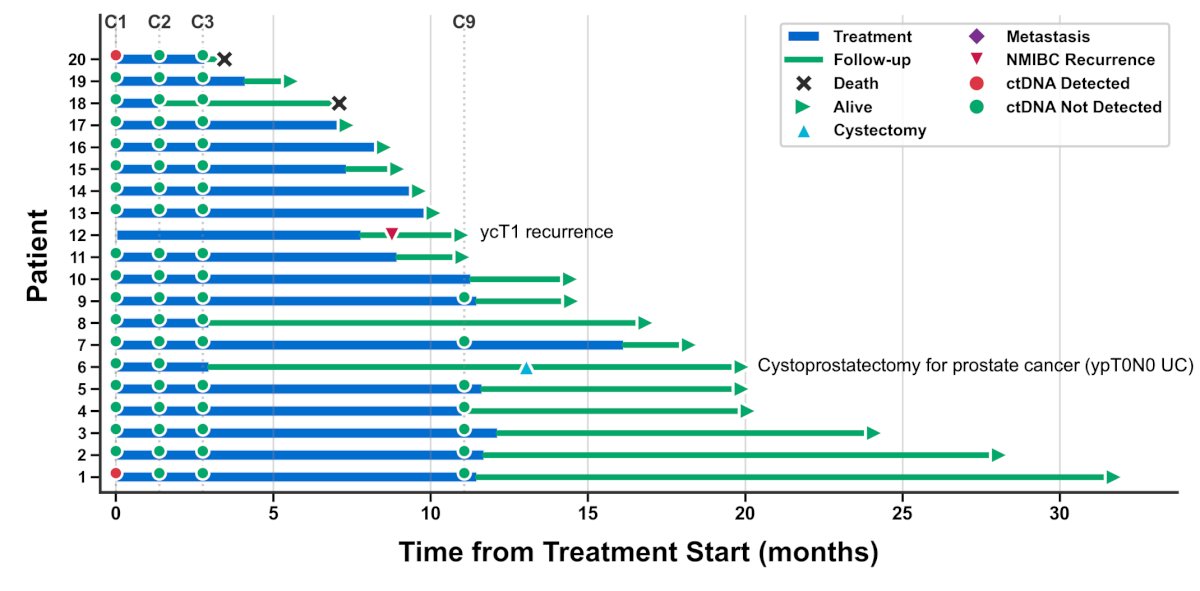
Cycle 2 ctDNA was undetectable in 100% patients with a clinical complete response. Among patients without a clinical complete response, undetectable cycle 2 ctDNA was associated with improved metastasis-free survival (HR 14.8, 95% CI 1.4-2000, p = 0.02). The following Swimmer plot highlights the outcomes in patients achieving a clinical complete response:
Dr. Anker concluded his presentation discussing the results of HCRN GU 20-444 with the following take-home points:
- A uniformly assessed and stringently defined clinical complete response was achieved in 43% of patients treated with pembrolizumab monotherapy after TURBT, and facilitated a response-guided bladder-sparing approach
- Undetectable ctDNA using an ultrasensitive whole genome sequencing-based approach identified patients at extremely low risk for metastatic recurrence
- All patients achieving a clinical complete response had undetectable ctDNA by cycle 2, day 1
- Follow-up for long-term outcomes in patients achieving a clinical complete response is ongoing
Presented by: Jonathan F. Anker, MD, PhD, Tisch Cancer Institute, Icahn School of Medicine at Mount Sinai, New York, NY
Related content: HCRN GU 20-444: Pembrolizumab After TURBT for Bladder‑Sparing in Cisplatin‑Ineligible MIBC - Jonathan Anker
Reference: