(UroToday.com) The 2026 GU ASCO annual meeting featured a urothelial carcinoma session and a presentation by Dr. Michiel S. van der Heijden discussing urinary tumor DNA and ctDNA in patients with muscle-invasive bladder cancer who received perioperative durvalumab in NIAGARA.
In NIAGARA, the addition of perioperative durvalumab to neoadjuvant chemotherapy and radical cystectomy demonstrated a significant improvement in event-free survival and overall survival and a numerical increase in pathological complete response versus neoadjuvant chemotherapy and radical cystectomy alone in patients with muscle-invasive bladder cancer.1 In a prior exploratory analysis, negative plasma ctDNA status after neoadjuvant treatment prior to radical cystectomy (pre-radical cystectomy) was associated with prolonged event-free survival but not pathological complete response. At ASCO GU 2026, Dr. van der Heijden and colleagues assessed urinary tumor DNA (utDNA) as a complementary approach in this setting.
Cisplatin-eligible patients with muscle-invasive bladder cancer (cT2-T4aN0/1M0) were randomized 1:1 to receive perioperative durvalumab plus neoadjuvant chemotherapy (cisplatin + gemcitabine) and radical cystectomy (durvalumab arm) or neoadjuvant chemotherapy and radical cystectomy alone (comparator arm):

Dual primary endpoints were event-free survival and pathological complete response. Exploratory analysis of utDNA and ctDNA was completed using the personalized Signatera™ assay at baseline (n = 205) and pre-radical cystectomy (n = 183).
Of 1,063 patients, 265 (25%) comprised the biomarker-evaluable population (134 durvalumab arm; 131 comparator arm). At baseline, lower utDNA levels were associated with longer event-free survival (low versus high utDNA HR 0.65, 95% CI 0.40−1.04). From baseline to pre-radical cystectomy, utDNA positive rate decreased from 85% to 55%. utDNA clearance was associated with longer event-free survival (HR 0.24, 95% CI 0.09−0.62) and was 11% higher in the durvalumab versus comparator arm (38.5% versus 27.1%):

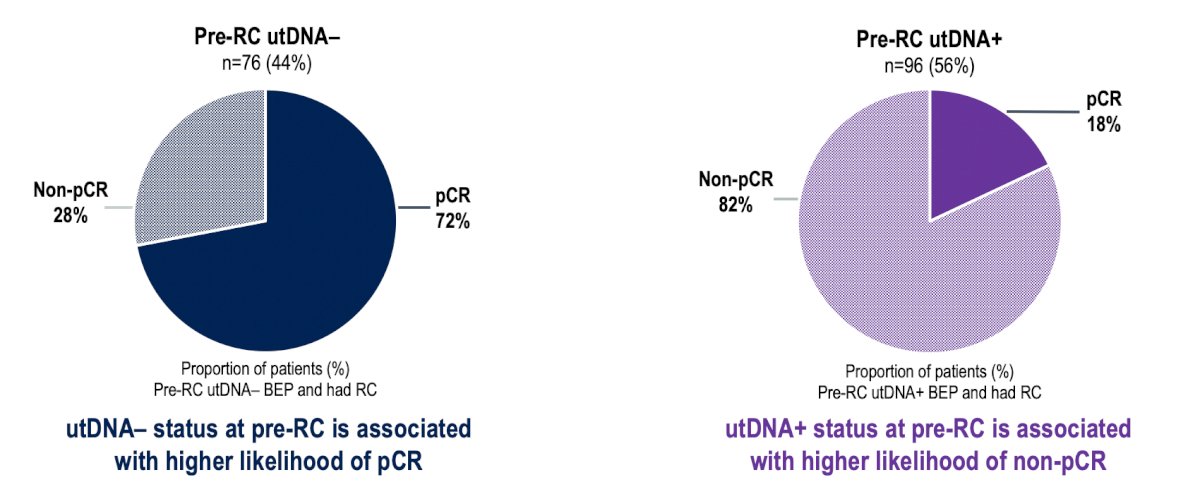
Pre-radical cystectomy utDNA status was associated with a pathological complete response: utDNA negative 72% (55/76) versus utDNA positive 18% (17/96):
Pre-radical cystectomy utDNA and ctDNA status differentially correlated with disease stage at radical cystectomy, with utDNA positive correlating with noninvasive disease (<T2N0M0) and ctDNA positive with invasive disease (≥T2N0M0) or systemic spread (N+ and/or M+):

The estimated 24-month event-free survival rate was highest for patients with dual-negative status at pre-radical cystectomy (utDNA negative ctDNA negative: 90%, 95% CI 83–97), followed by patients with utDNA positive only (utDNA positive ctDNA negative: 75%, 95% CI 65–87), and was lowest for patients with dual-positive status (utDNA positive ctDNA positive: 55%, 95% CI 41–75):

Dr. van der Heijden concluded his presentation discussing urinary tumor DNA and ctDNA in patients with muscle-invasive bladder cancer who received perioperative durvalumab in NIAGARA with the following take-home points:
- This is the largest data set from a phase 3 trial describing associations of utDNA with outcomes in muscle-invasive bladder cancer
- Pre-radical cystectomy clearance of utDNA appears to be prognostic for event-free survival (clearance versus persistence HR 0.24); utDNA clearance rate was 11% higher in the durvalumab arm versus the comparator arm
- utDNA negative status at pre-radical cystectomy was associated with a higher likelihood of pathological complete response, in contrast to prior findings for ctDNA negative status
- Combined pre-radical cystectomy ctDNA and utDNA analyses were associated with event-free survival and offer complementary insights into pathological staging at radical cystectomy, with utDNA potentially providing clinically relevant information on the primary bladder tumor
- These data highlight the potential value of combining utDNA and ctDNA analyses to guide future management of muscle-invasive bladder cancer
Presented by: Michiel Simon Van Der Heijden, MD, PhD, Medical Oncologist, Trial Group Leader, Department of Medical Oncology, Netherlands Cancer Institute, Amsterdam, Netherlands
Reference: