(UroToday.com) The 2026 GU ASCO annual meeting featured a urothelial carcinoma session and a presentation by Dr. Avivit Peer discussing results from the KEYMAKER-U04 substudy 04B assessing first-line enfortumab vedotin + pembrolizumab-based immune checkpoint inhibitor combinations for advanced urothelial carcinoma.
Enfortumab vedotin + pembrolizumab is the preferred standard first-line therapy for patients with locally advanced or metastatic urothelial carcinoma. The randomized, open-label phase 1/2 substudy 04B in the KEYMAKER-U04 umbrella study (NCT05845814) aimed to build on the efficacy of this combination and evaluated enfortumab vedotin + pembrolizumab, containing immune checkpoint inhibitor co-formulations and enfortumab vedotin + pembrolizumab as first-line treatment in participants with locally advanced or metastatic urothelial carcinoma.
Adult participants without prior systemic therapy for locally advanced or metastatic urothelial carcinoma and an ECOG performance status of 0-1 were randomized 1:1:1 to enfortumab vedotin + coformulated favezelimab (anti–LAG3) + pembrolizumab 800 mg/200 mg (arm A), enfortumab vedotin + coformulated vibostolimab (anti-TIGIT) + pembrolizumab 200 mg/200 mg (arm B), and enfortumab vedotin + pembrolizumab 200 mg (arm C). Participants received enfortumab vedotin 1.25 mg/kg IV on d1 and d8 Q3W until disease progression, intolerable toxicity, or study withdrawal, and pembrolizumab or pembrolizumab-containing coformulations IV on day 1 Q3W for ≤2 years:
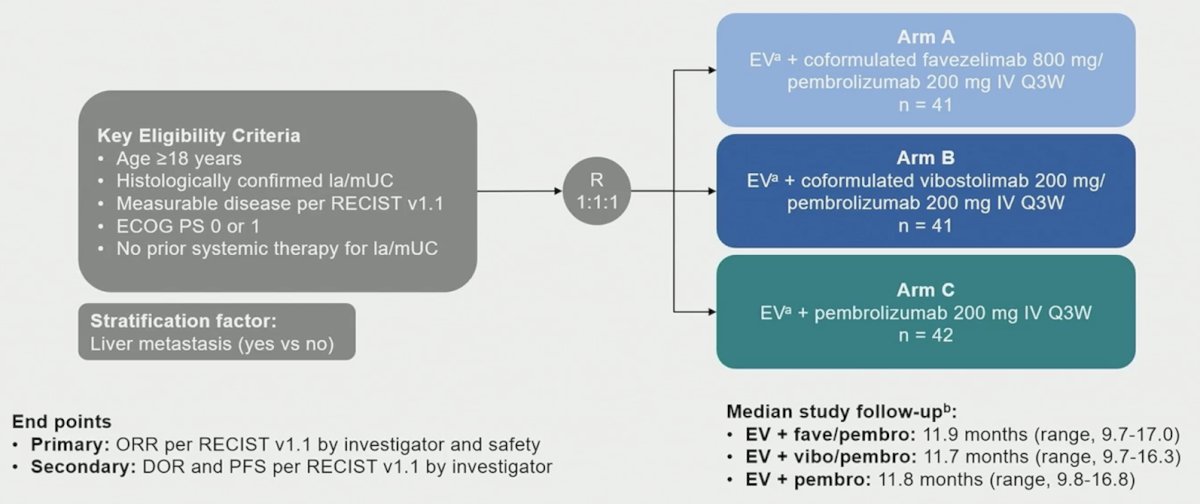
A safety lead-in was performed for the first 10 participants in each of enfortumab vedotin + favezelimab + pembrolizumab and enfortumab vedotin + vibostolimab + pembrolizumab arms per modified toxicity probability interval with dose-limiting toxicity monitoring in cycle 1. The primary end points were objective response rate per RECIST v1.1 by blinded independent central review and safety. Secondary end points included progression-free survival and duration of response per RECIST v1.1 by blinded independent central review.
There were 124 participants that received treatment (arm A: n = 41; arm B: n = 41; arm C: n = 42). The median follow-up (time from randomization to data cutoff; December 16, 2024) was 11.9 months (range: 9.7-17.0), 11.7 months (range: 9.7-16.3), and 11.8 months (range: 9.8-16.8), for arms A, B, and C, respectively. Most participants were male (74%), and the median age was 69 years. The following table highlights the baseline characteristics of patients in the trial:

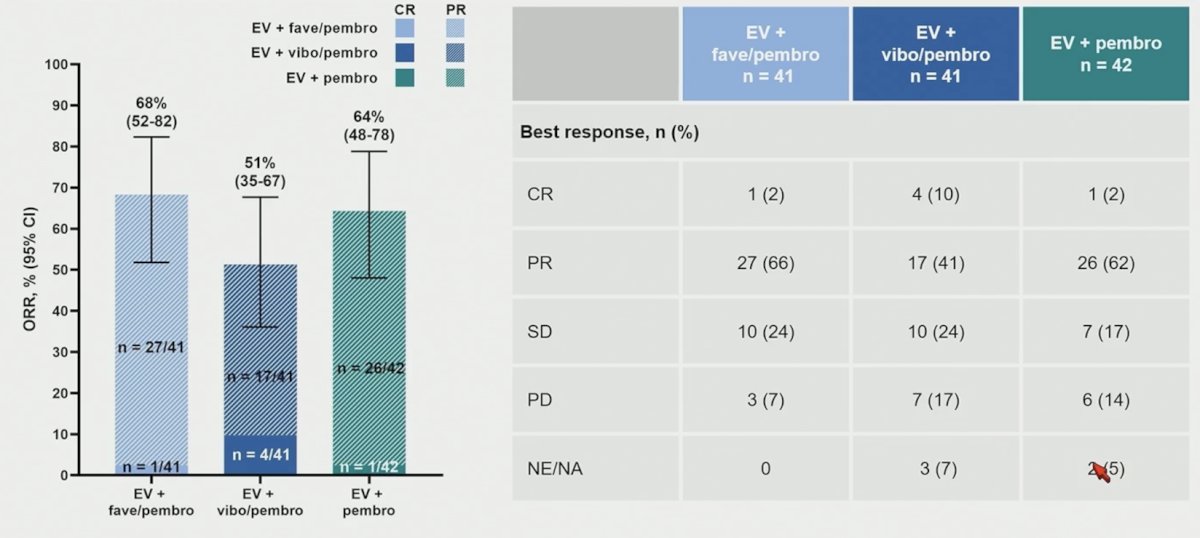
Dose limiting toxicity was reported for 1/10 participants on enfortumab vedotin + favezelimab + pembrolizumab and no participants on enfortumab vedotin + vibostolimab + pembrolizumab. The objective response rate was 68% for Arm A, 51% for Arm B, and 64% for Arm C:
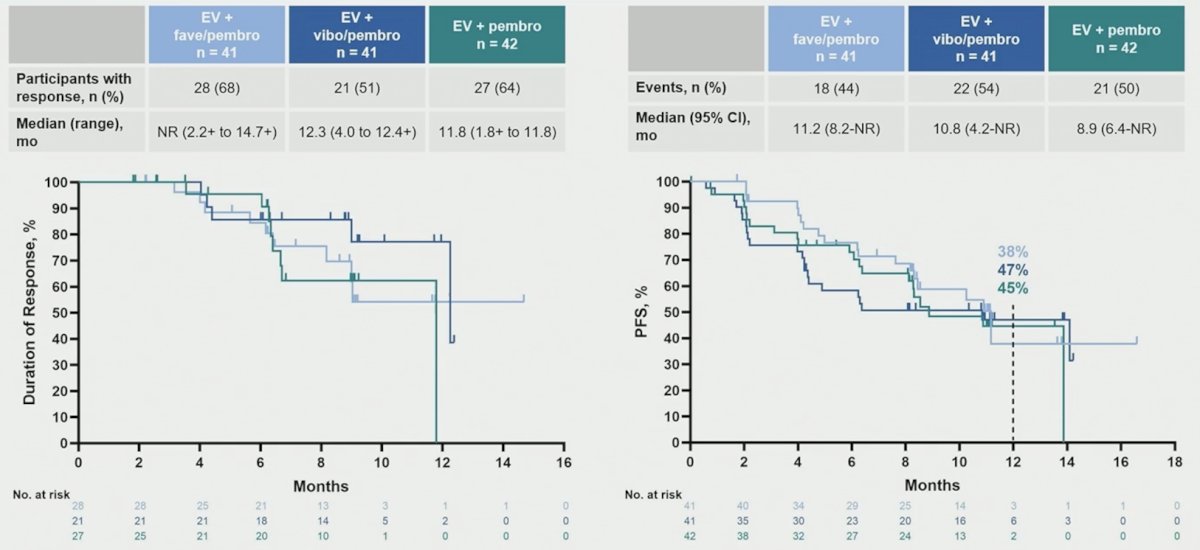
The median duration of response was not reached for Arm A, was 12.3 months for Arm B, and was 11.8 months for Arm C. The median progression-free survival was 11.2 months for Arm A, 10.8 months for Arm B, and 8.9 months for Arm C:
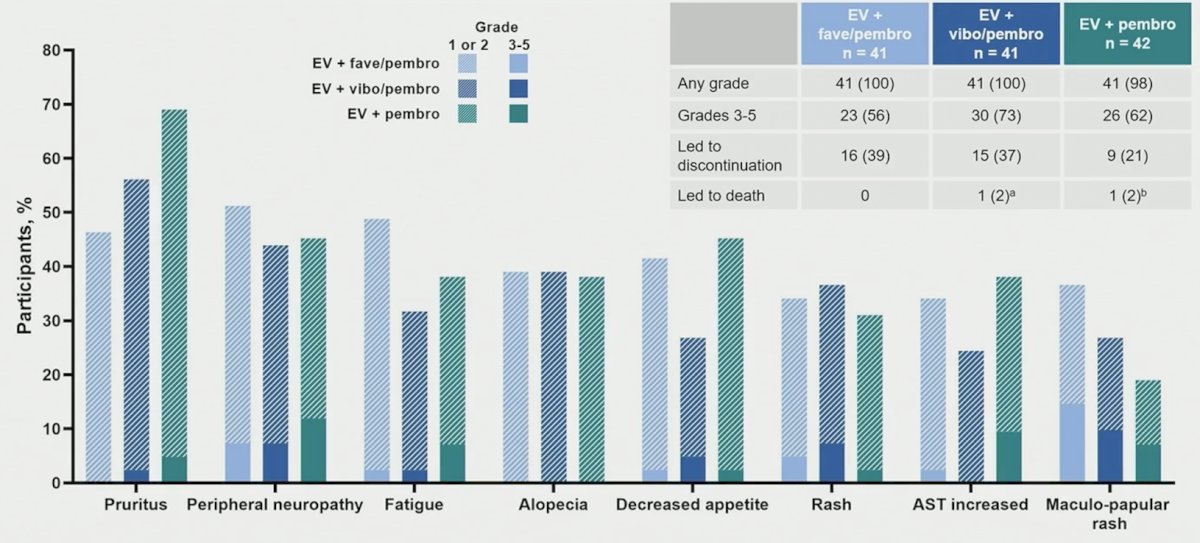
Any-grade treatment-related adverse events were similar across all arms (arm A: 100%; arm B: 100%; arm C: 98%). Moreover, grade ≥3 treatment-related adverse events were reported for 56%, 73%, and 6% of participants in arms A, B, and C, respectively:
Immune-mediated adverse events and infusion reactions were reported for 66% participants in arm A, 54% in arm B, and 423% in arm C:

Immune-mediated adverse events with > 10% higher incidence in any enfortumab vedotin + pembrolizumab containing immune checkpoint inhibitor coformulation were hypothyroidism (31.7%, 14.6%, and 2.4%, respectively), severe skin reactions (24.4%, 29.3%, and 14.3%, respectively), hyperthyroidism (22.0%, 4.9%, and 4.8%, respectively), and infusion reactions (17.1%, 2.4%, and 0%, respectively).
Dr. Peer concluded her presentation discussing results from the KEYMAKER-U04 substudy 04B with the following take-home points:
- In participants with locally advanced or metastatic urothelial carcinoma, there is no indication of improvement in efficacy with the addition of LAG-3– or TIGIT-targeted immune checkpoint inhibitors to enfortumab vedotin + pembrolizumab
- Safety profiles were consistent with the known profiles of the individual drugs
Incidence of some immune-mediated adverse events was higher with pembrolizumab-containing coformulations compared with enfortumab vedotin + pembrolizumab, including hypothyroidism, severe skin reactions, hyperthyroidism, and infusion reactions
- Safety profiles were consistent with the known profiles of the individual drugs
- Current data do not support further evaluation of LAG-3 and TIGIT inhibition in locally advanced or metastatic urothelial carcinoma
- Limitations include the small sample size and that the study arms were descriptive and not designed for formal comparison
Presented by: Avivit Peer, MD, Rambam Health Care Campus, Haifa, Israel
Related content: KEYMAKER Substudy Tests Triplet Combinations with EV-Pembro in First-Line Bladder Cancer - Avivit Peer