(UroToday.com) The 2026 GU ASCO annual meeting featured the release of new data from the Bladder Cancer Advocacy Network’s (BCAN) New Faces of Bladder Cancer Survey. Over the past two decades, the bladder cancer landscape has evolved significantly, with meaningful advances in diagnostics, intravesical therapies, systemic treatment options, and patient education. However, therapeutic progress alone does not fully define quality care.
Understanding the lived experience of patients, for example, how they navigate symptoms, delays, procedures, financial stress, and survivorship, is equally essential. BCAN’s New Faces of Bladder Cancer 2025 Survey offers one of the most comprehensive patient-reported datasets to date, providing a granular look at where there has been improvement and where gaps persist. The following article summarizes the key findings of the BCAN New Faces of Bladder Cancer 2025 Survey presented at GU ASCO 2026.
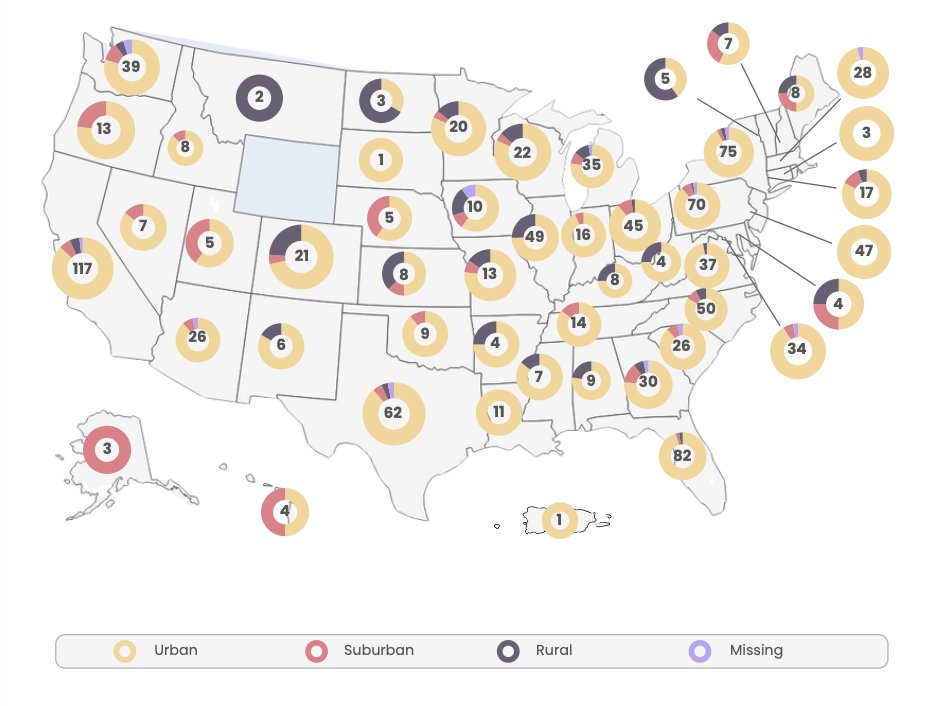
The New Faces of Bladder Cancer 2025 survey represents the largest patient-centered initiative in BCAN’s history, incorporating over 1,100 analyzable United States responses from individuals across 49 states and Puerto Rico. This also includes representation from urban (86%), suburban (7%), and rural residents (6%):
With a 74-question instrument capturing quantitative and qualitative data, the survey evaluates the entire bladder cancer journey: from symptom onset and diagnostic pathways to treatment experiences, surveillance burden, psychosocial impact, and financial toxicity.
The demographic profile among survey respondents broadly mirrors the national epidemiology. The median age at bladder cancer diagnosis was 66 years and the median at survey completion was 70 years, aligning closely with SEER data demonstrating a predominance in older adults: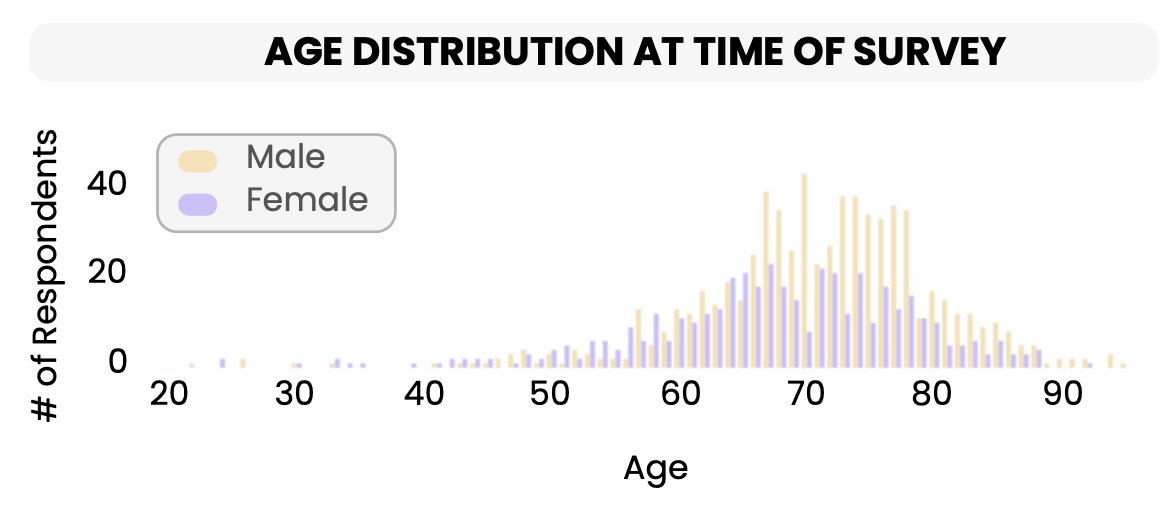
Approximately 61% of respondents were male and 39% female, a smaller male predominance than national incidence statistics, potentially reflecting higher engagement of women within patient advocacy communities. Importantly, racial and ethnic diversity was limited, with 95% identifying as White, underscoring the need for broader outreach and inclusion in future patient experience research. Most respondents were retired (63%), though several patients noted that they retired early secondary to their diagnosis and treatments. Among these respondents (n = 42), the mean age at diagnosis of bladder cancer was 57 years. Overall, 2 of 3 respondents reported that they had other comorbidities, most commonly hypertension and cardiovascular disease:
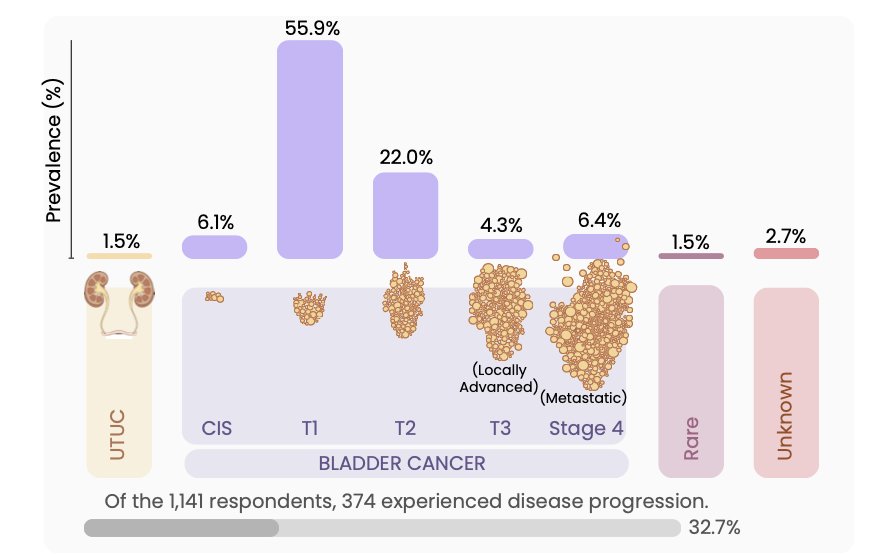
Stage distribution was consistent with national patterns: approximately half of patients were initially diagnosed with non–muscle invasive bladder cancer, 22% with T2 disease, and smaller proportions with locally advanced, metastatic, upper tract urothelial carcinoma, or rare histologies. Nearly one-third of respondents experienced disease progression over time, reflecting the chronic and recurrent nature of bladder cancer:
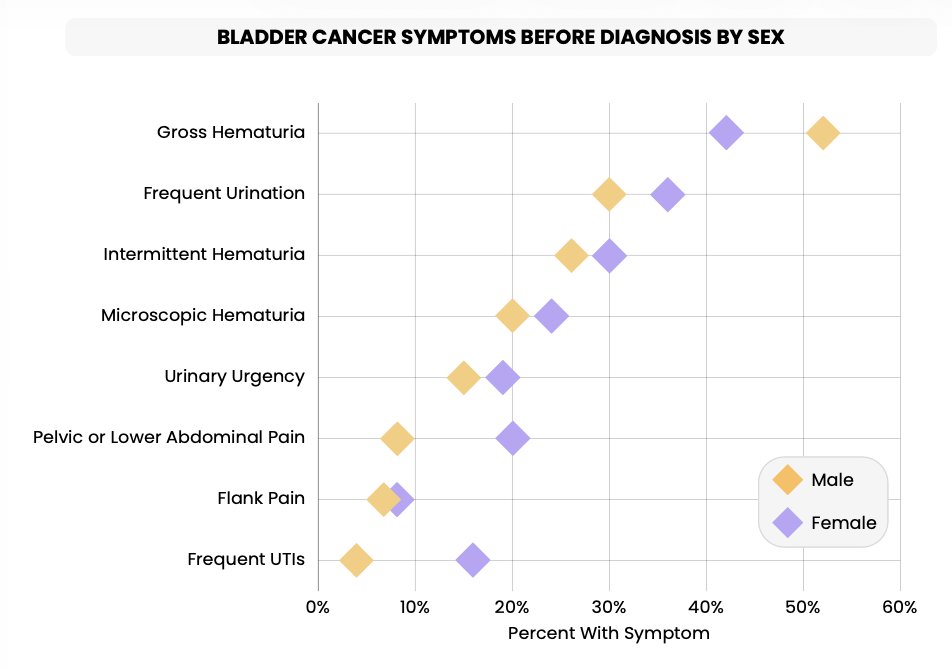
Gross hematuria remained the most common presenting symptom, reported by nearly half of respondents. When including intermittent and microscopic hematuria, the majority of patients experienced bleeding prior to diagnosis. Frequent urination and urgency were also common, particularly among women:
Despite this classic symptom profile, diagnostic delays remain prevalent, particularly among female patients. Nearly half (45%) of women reported being treated for at least one urinary tract infection prior to diagnosis, compared to 15% of men. Many described multiple rounds of antibiotics before referral to urology, and those with UTI histories were more likely to ultimately present with muscle-invasive disease, reinforcing evidence that misattribution of hematuria to infection contributes to later-stage diagnosis.
Care pathways also differed by sex, whereby women were less likely to see a urologist initially and more likely to begin care with primary care providers or gynecologists. Younger patients also demonstrated longer delays before seeking evaluation, sometimes waiting more than six months. These findings highlight a critical opportunity for improved education and referral pathways, particularly in populations perceived as lower risk. Importantly, 61% of respondents sought medical attention immediately after symptom onset, suggesting that patient-driven delay is not the sole issue. Structural barriers, including appointment availability, specialist access, and diagnostic sequencing, remain important for a timely diagnosis
Bladder cancer surveillance remains procedurally intensive. Nearly half of respondents reported undergoing 5 or more cystoscopies, and 17% experienced more than 15 procedures. The burden was particularly pronounced among those with CIS and high-risk NMIBC, consistent with guideline-directed surveillance:
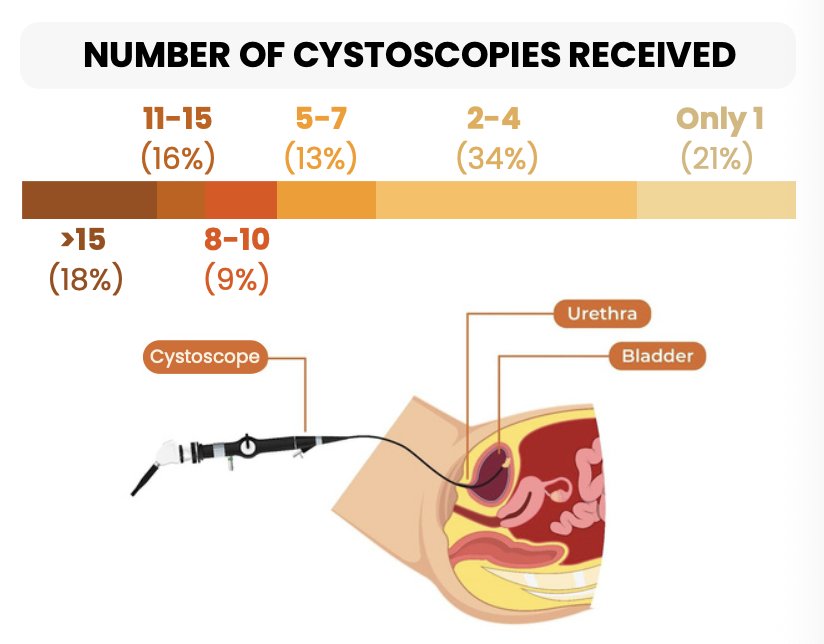
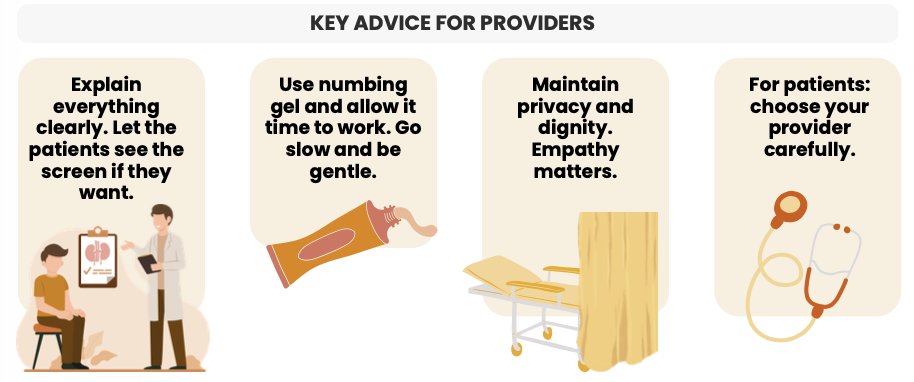
Patient experiences with cystoscopy varied considerably. While many described modern flexible cystoscopes as more tolerable than older rigid instruments, negative experiences were often linked to inadequate pain control, insufficient explanation, and perceived lack of empathy. A consistent theme emerged in that technical proficiency alone does not define procedural quality, highlighting the importance of communication, privacy, and clinician demeanor significantly shaping patient perception. The following figure highlights key advice for providers performing cystoscopy:
TURBT frequency mirrored the bladder cancer stage of disease. Among those with NMIBC, the majority underwent multiple resections, with a subset (7%) reporting more than seven procedures. Restaging TURBT was performed in 45% of patients with NMIBC or MIBC, and 24% of those undergoing restaging reported present cancer, recurrence, or progressive disease. These findings highlight both the oncologic necessity and cumulative burden of repeat resections in early-stage bladder cancer management.
Blue light cystoscopy adoption remains limited in real-world practice. Only 15% of respondents reported receiving blue light cystoscopy, despite evidence supporting improved tumor detection and recurrence reduction. Utilization did not vary substantially by insurance type, suggesting that institutional access and infrastructure may be the primary limiting factors.
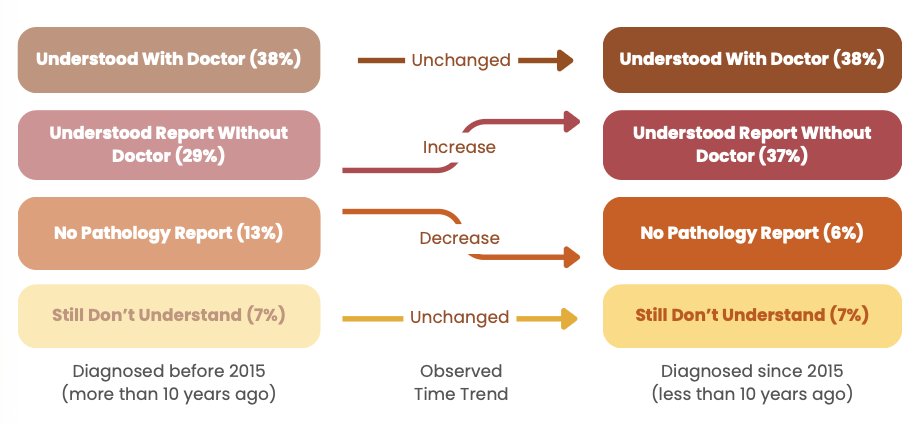
Nearly all patients reported receiving pathology reports after TURBT. Encouragingly, comprehension appears to have improved compared to a decade ago. Approximately one-third understood the report independently, and another 38% understood after the clinician's explanation, with only 7% reporting persistent confusion:
However, pathology reports remain highly technical. Many respondents described anxiety when viewing reports through patient portals prior to clinical discussion. Importantly, advocacy resources—particularly BCAN educational materials—were frequently credited with improving understanding.
Only 12% of respondents reported undergoing genetic or molecular testing of their tumors, many being unaware that such testing was available, with cost barriers being common. Among those tested, reported alterations included FGFR3, TP53, ERBB2, and Nectin-4. As molecular profiling becomes increasingly relevant to treatment selection, recurrence prediction, and clinical trial enrollment, this low utilization rate highlights a significant gap in contemporary bladder cancer care. Financial barriers further complicate access, given that 1 in 6 of those tested paid out-of-pocket or faced insurance denials. These findings emphasize the need for standardized discussions around molecular testing and improved insurance navigation support.
Respondents diagnosed within the past decade were more likely to report being presented with multiple treatment options and participating in goal-oriented discussions. Indeed, advances in intravesical therapies, immunotherapies, targeted agents, and systemic combinations have expanded therapeutic options. Only 34% of recently diagnosed patients reported that treatment goals were not discussed, compared to 42% diagnosed over ten years ago.
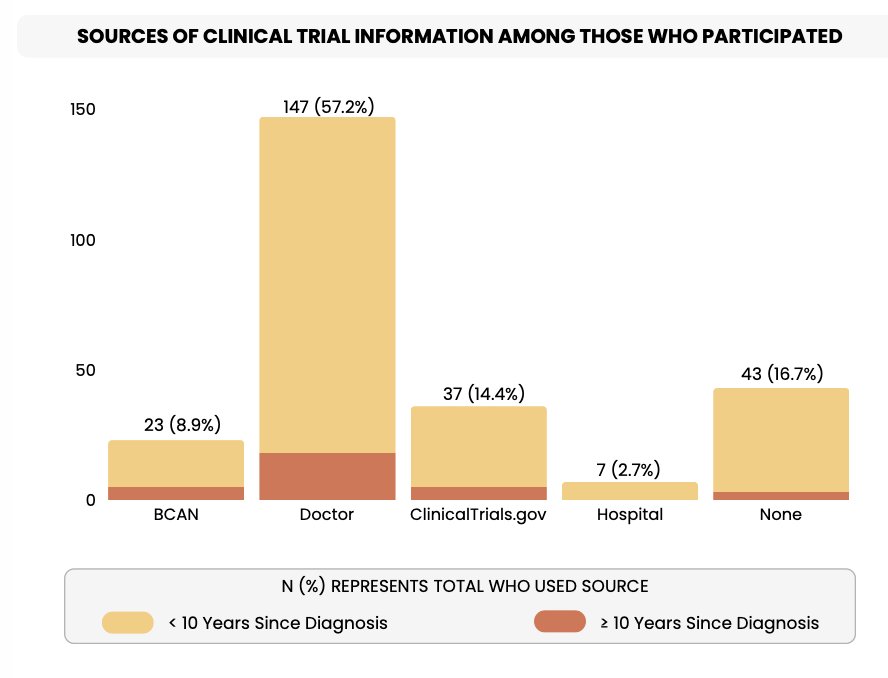
Clinical trial awareness has also improved, with 33% of recently diagnosed patients exploring trials compared to 23% in earlier cohorts, suggesting growing integration of research into standard care discussions. The following figure highlights the sources of clinical trial information among those who participated:
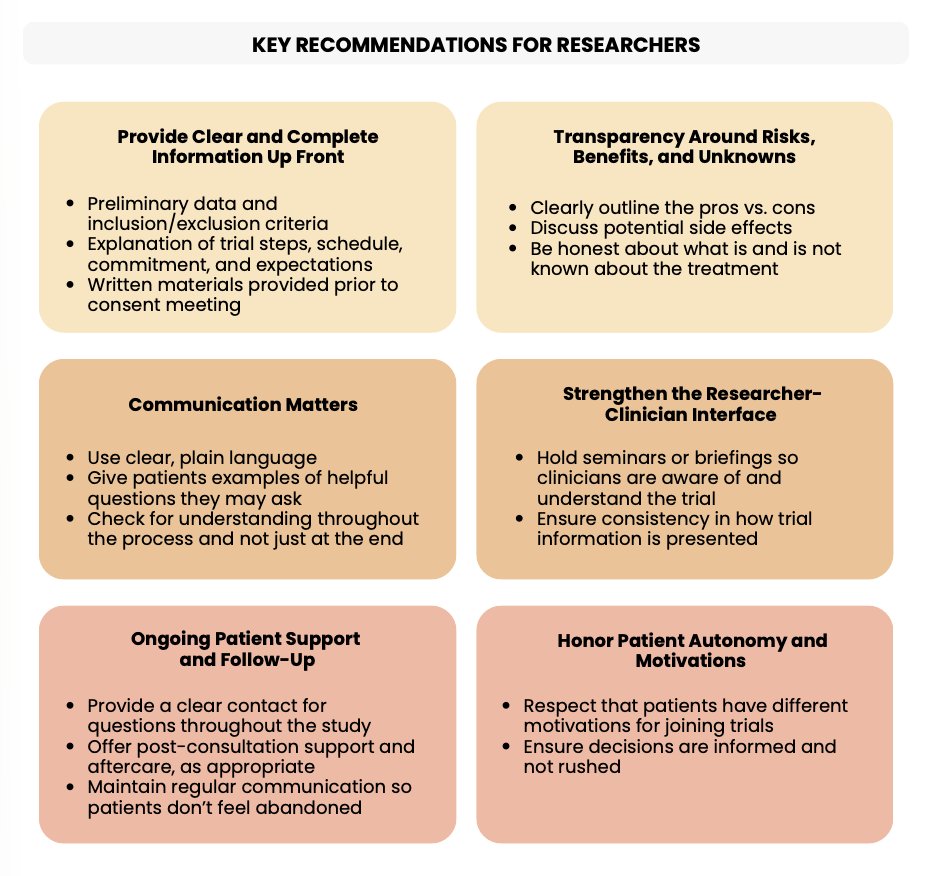
Additionally, respondents provided the following key recommendations for providers regarding patients considering a clinical trial:
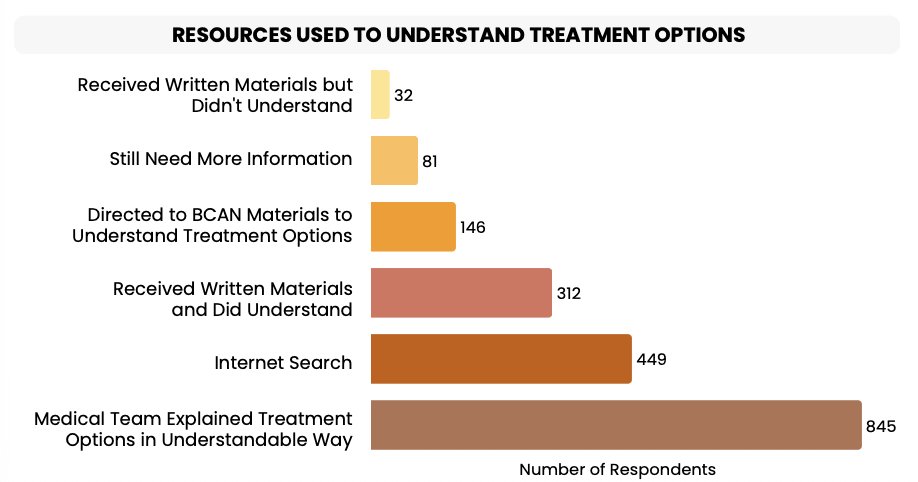
Patients diagnosed within the last 10 years were also more likely to have understandable written materials and other resources compared to those diagnosed more than a decade ago:
Overall, 43% of respondents noted that they sought a second opinion for their treatment options, which were more common among urban and suburban residents (44%) compared to rural residents (26%). Patients responded that a second opinion was an empowering experience that instilled confidence that they were receiving the correct treatment.
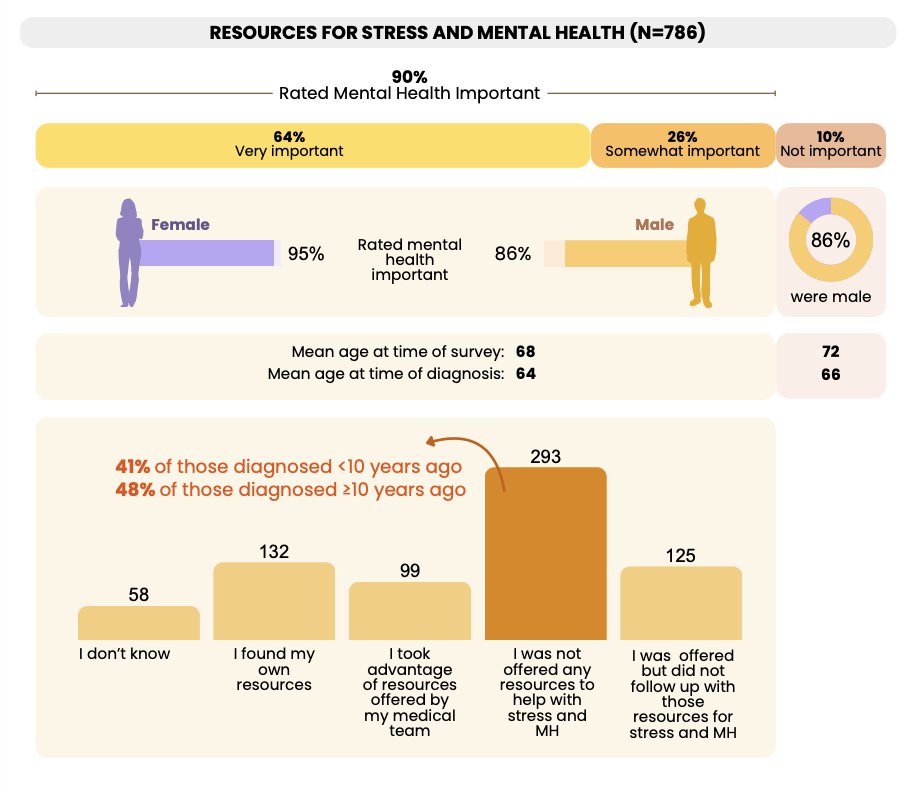
Despite therapeutic progress, supportive care remains inconsistent. While over 90% of respondents rated mental health support as important, 41% were never offered such resources. Even when offered, uptake was limited by insurance coverage, availability of cancer-focused counseling, and logistical barriers:
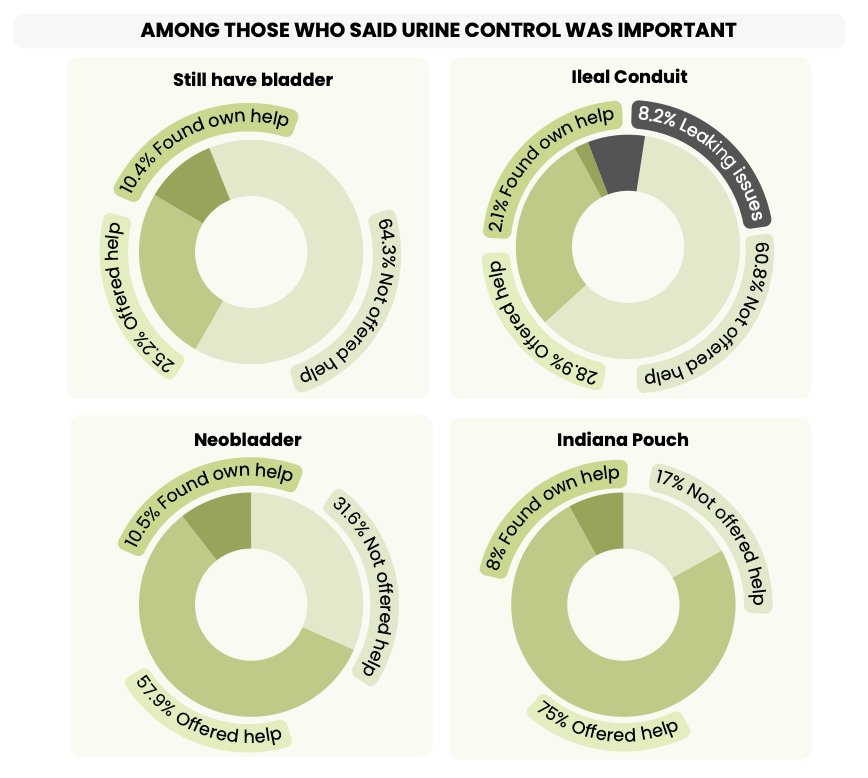
Fear of recurrence remains pervasive, affecting 79% of respondents. Younger patients (91% of those under 50 years of age) and women (86% versus 74% of men) reported even higher rates of fear of recurrence. This chronic anxiety shapes survivorship in profound ways, yet structured survivorship care plans were not routinely provided. Over half of respondents reported never receiving a survivorship plan, despite recognizing its importance. Sexual function and continence support were also under-addressed, with only 27% of patients who valued sexual function (79%) being offered relevant resources. Additionally, continence experiences, challenges, and support varied by urinary diversion reconstruction type, with neobladder patients reporting continence as most important, but only 30% saying they were offered any help despite commonly having nighttime leakage, urgency, and incontinence. The following figure highlights what respondents said among those who stated urine control was important:
Financial strain affected 20% of respondents overall and 41% of those diagnosed before the age of 50 years. Hidden costs, including travel, surveillance copays, time off work, and long-term supply needs, compounded the burden. A particularly concerning finding is that some patients reported modifying or delaying treatment due to cost concerns. Employment disruption was also common, particularly among younger individuals and those with advanced disease. Many described early retirement, disability, or job loss secondary to treatment complications. These findings reinforce the far-reaching economic consequences of bladder cancer beyond direct medical costs.
The New Faces of Bladder Cancer report documents meaningful advances in patient education, treatment availability, shared decision-making, and clinical trial awareness. Modern cystoscopy technology has improved tolerability, pathology comprehension has strengthened, and treatment options have expanded. However, diagnostic disparities, particularly among women, persist. Genetic testing remains underutilized, and mental health and survivorship services are inconsistently integrated. Financial toxicity continues to influence care decisions. These gaps represent actionable targets for clinicians, institutions, policymakers, and advocacy organizations.
In conclusion, the New Faces of Bladder Cancer 2025 survey represents the collective voice of over 1,100 individuals dealing with bladder cancer. Indeed, bladder cancer care has progressed substantially over the past two decades, but patient-reported data make clear that excellence in oncologic outcomes must be matched by equity in access, communication, and supportive care. Addressing sex-based diagnostic delays, expanding molecular testing access, embedding structured survivorship planning, and proactively mitigating financial toxicity are essential next steps. As therapeutic innovation accelerates, ensuring that every patient experiences comprehensive, patient-centered care remains a shared responsibility.
Related content: BCAN Unveils Patient-Centered Survey on Emotional and Financial Impacts of Bladder Cancer - Meri-Margaret Deoudes