(UroToday.com) The 2026 GU ASCO annual meeting featured a urothelial carcinoma session and a presentation by Dr. Pooja Ghatalia discussing an integrated analysis of the RETAIN trials assessing ctDNA to guide response-adapted bladder preservation in muscle-invasive bladder cancer.
Radical cystectomy is a life-altering surgery, and bladder preservation is important to our patients. Approximately 35-60% of patients achieve a pathological complete response with neoadjuvant therapy, and thus response-adapted bladder-sparing approaches are being studied in clinical trials: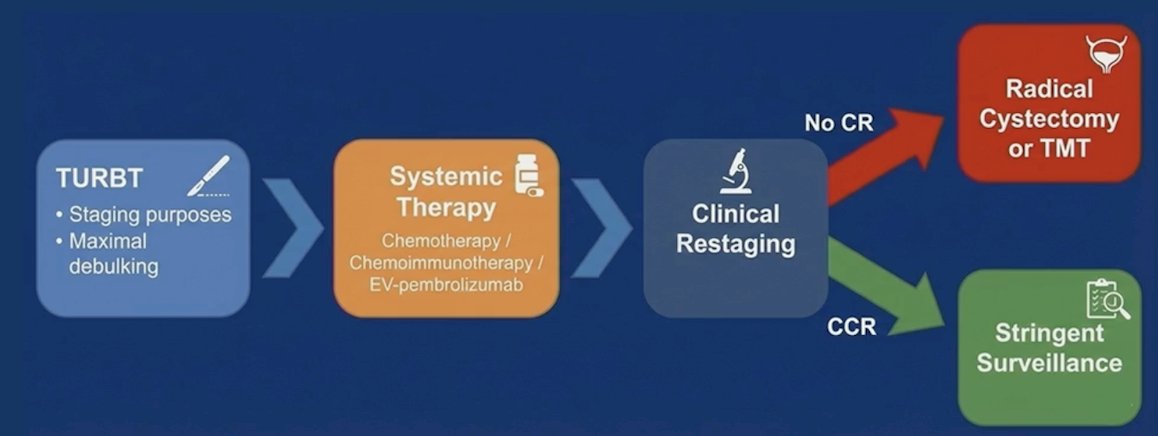
The phase II RETAIN-11 and 2 trials evaluated a response-adapted approach to identify patients with muscle-invasive bladder cancer who may safely undergo cystectomy-sparing active surveillance after neoadjuvant therapy. RETAIN-1 evaluated accelerated MVAC, and RETAIN-2 combined nivolumab with accelerated MVAC. Although ctDNA is prognostic in patients treated with cystectomy, its role in selecting or monitoring patients on active surveillance is unknown. At ASCO GU 2026, Dr. Ghatalia and colleagues reported updated RETAIN-2 outcomes and an integrated ctDNA analysis from RETAIN-1/2 to evaluate the role of ctDNA in risk stratification for bladder preservation.
RETAIN-2 enrolled patients with cT2-T3N0M0 muscle-invasive bladder cancer treated with accelerated MVAC + nivolumab. TURBT samples were sequenced for ATM, ERCC2, or RB1 mutations. Patients with >1 mutation and a clinical complete response (restaging TUR, urine cytology, and CT) entered active surveillance, whereas others received bladder-directed therapy: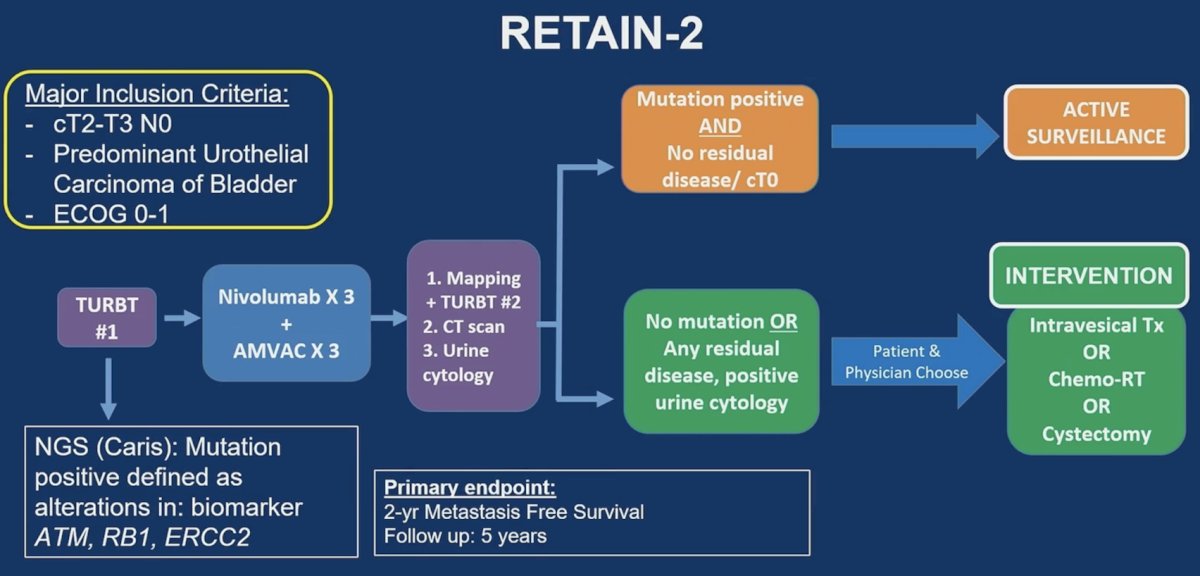
The primary endpoint was 2-year metastasis-free survival in the ITT population. Plasma from both trials was analyzed with Signatera at baseline and post-therapy, with RETAIN-2 including 3- and 6- month draws.
The patient disposition is highlighted in the following figure, noting there were 71 patients in the intention-to-treat population, of which 47 had an intervention recommended, and 23 were recommended to undergo active surveillance. Ultimately, 48 patients had an intervention, and 22 opted for active surveillance: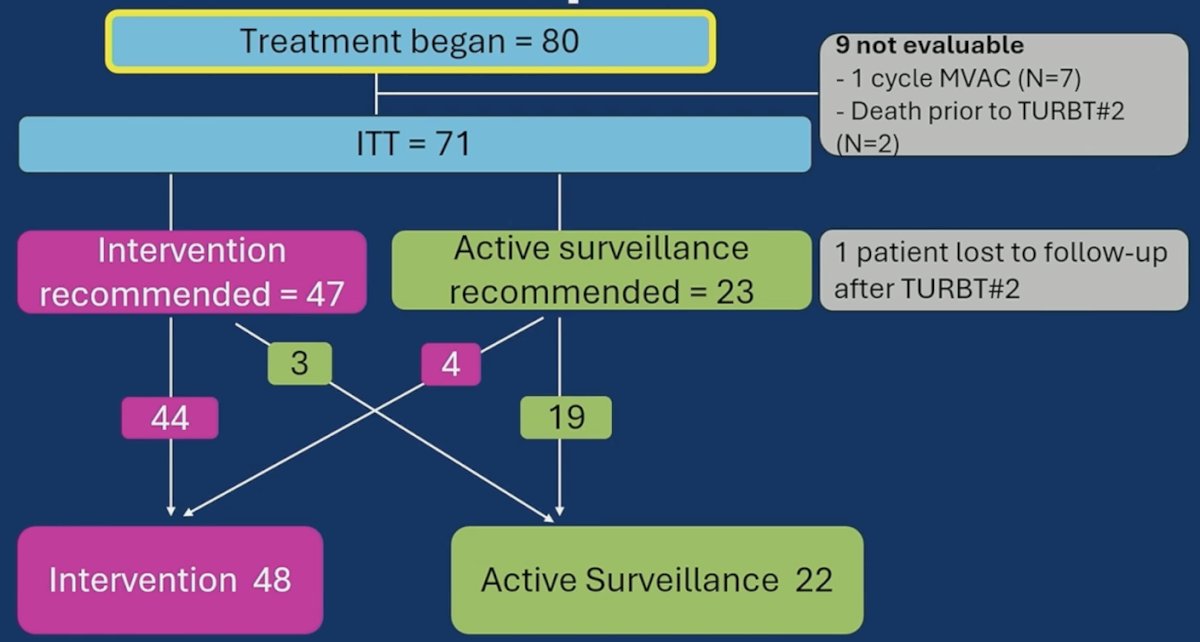
Among 71 evaluable RETAIN-2 patients, the median age was 69 years (range: 68-86), 77% were male, and 42% had cT3 disease: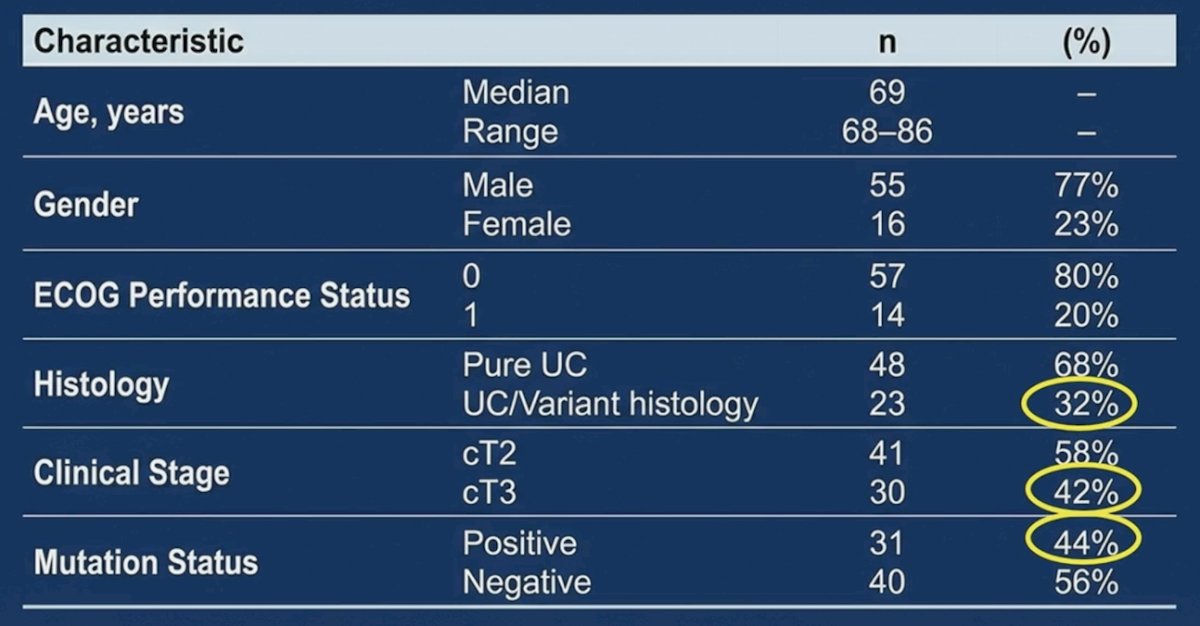
Over a median follow-up of 32 months (IQR 26.2-47.8), the proportion of patients who were metastasis-free at 2 years in the intention-to-treat population was 70%, with the lower bound of 1-sided 90% exact confidence interval of 62.4%. Non-inferiority was declared if the lower bound of the 1-sided 90% exact confidence interval was >56%. Thus, the null hypothesis was rejected, and declared that the risk-adapted approach was non-inferior.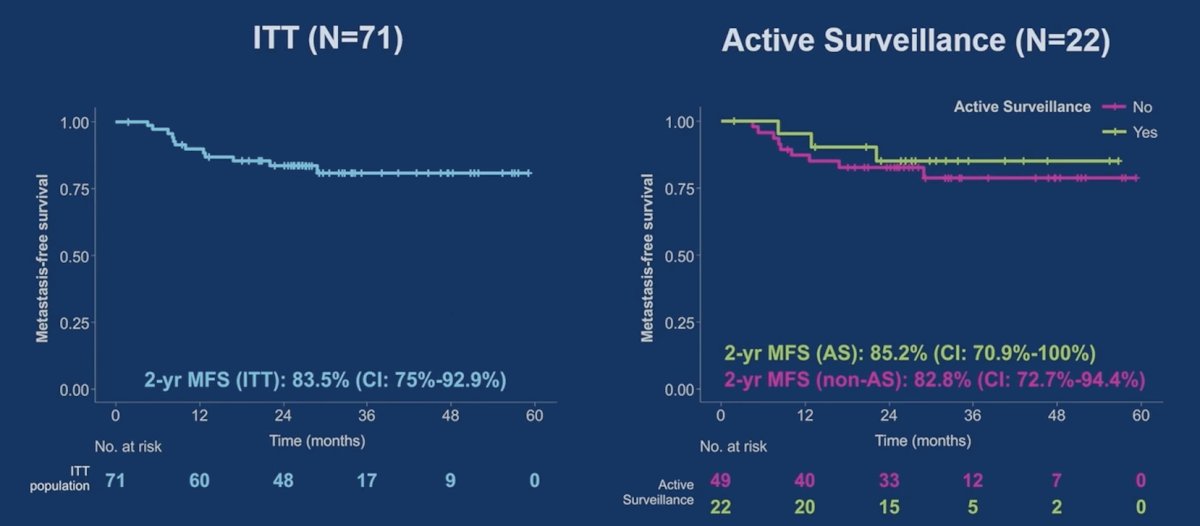
Among 48 patients in the intervention group, 36 underwent radical cystectomy, of which 46% were ypT0 and 63% were <= ypT1: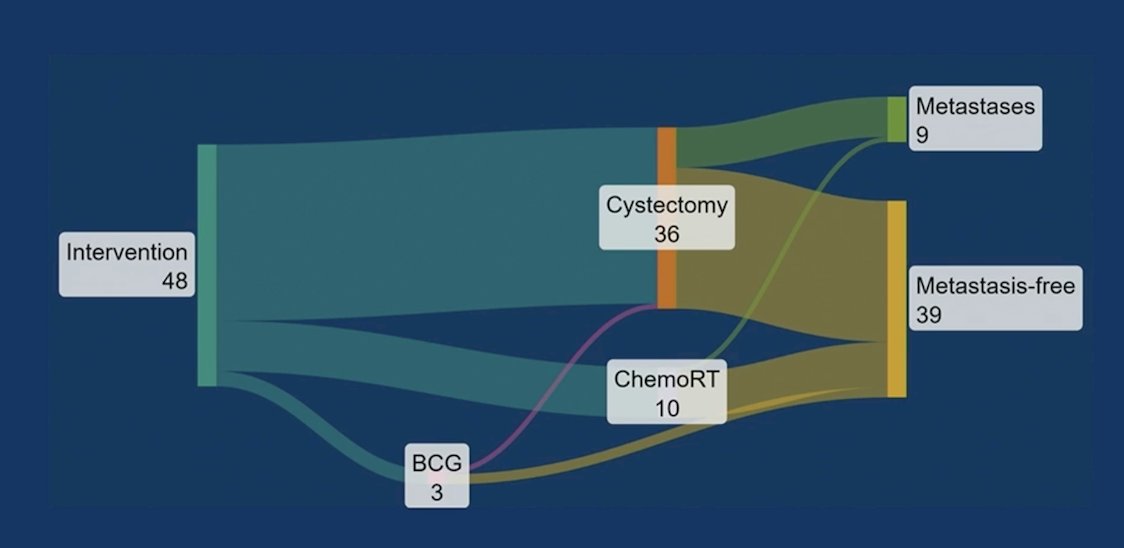
Among 22 active surveillance patients, 8 (36%) had bladder cancer recurrence, 3 (14%) developed metastases, and 4 needed salvage cystectomy: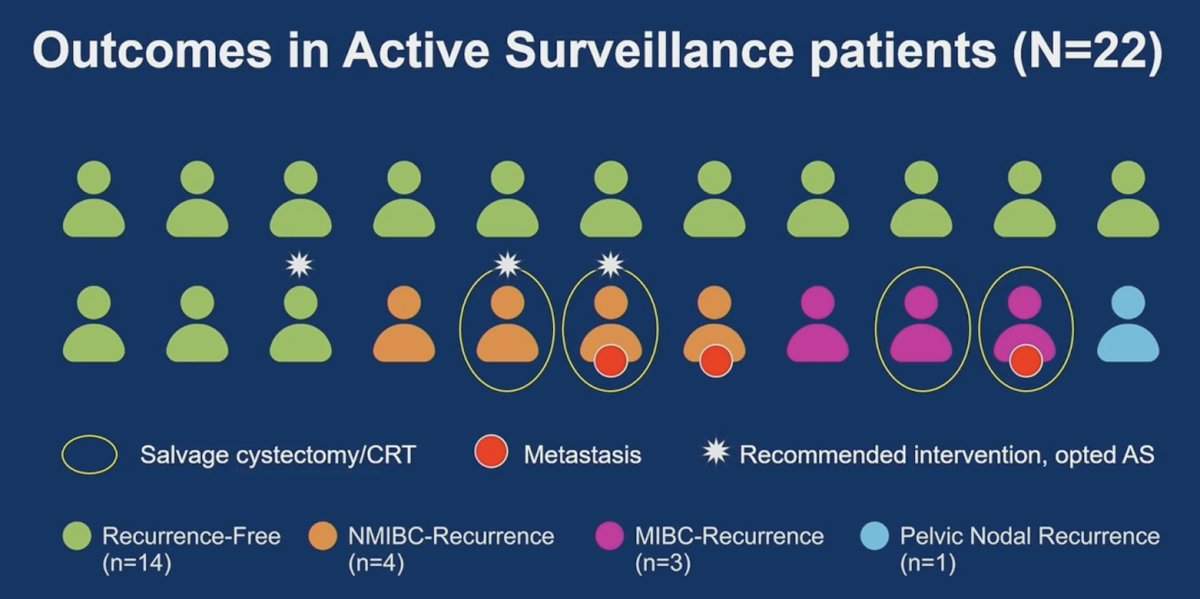
Overall, 68% of patients on active surveillance remained metastasis-free with an intact, non-irradiated bladder, and all metastatic events were preceded by local recurrence. The following figure highlights a comparison of RETAIN-1 versus RETAIN-2 outcomes in active surveillance patients: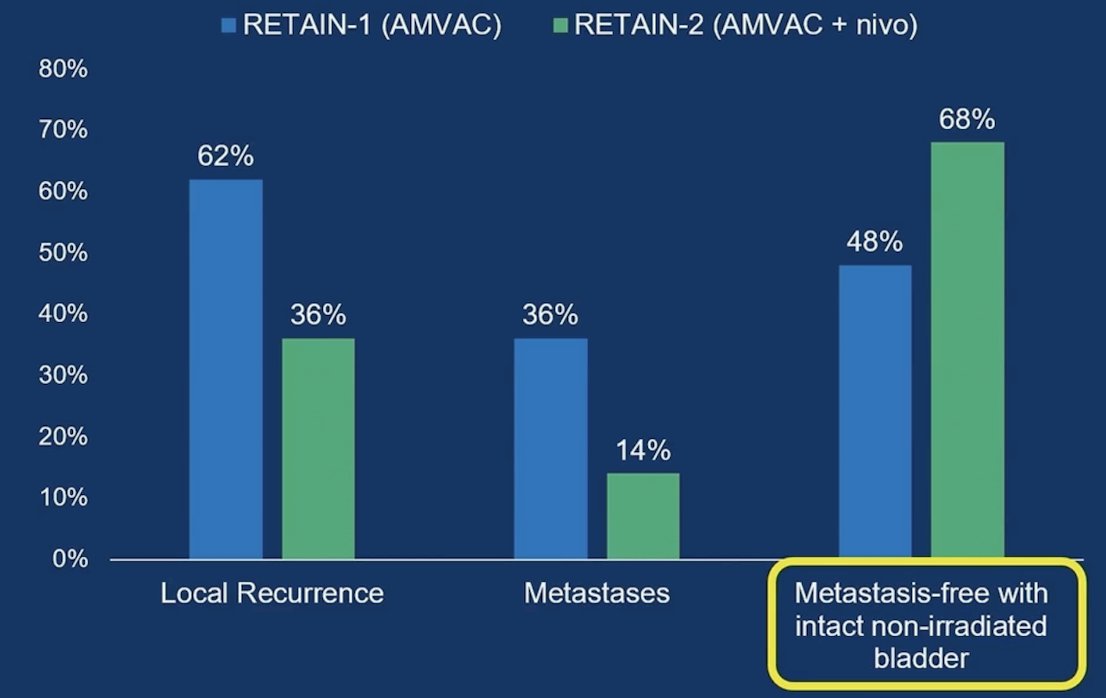
Across both trials (RETAIN-1/2), 274 ctDNA time points from 111 patients were analyzed. Baseline and post-therapy ctDNA positivity were 42.3% and 13.6%, respectively. Among baseline positives, 72.7% (32/44) cleared ctDNA: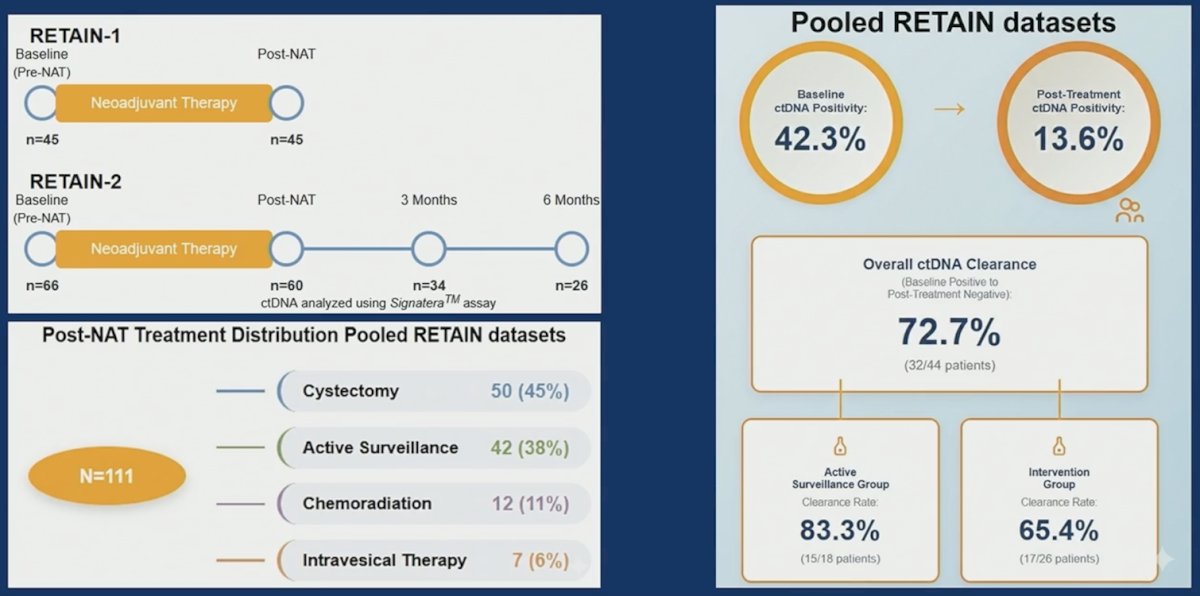
ctDNA positivity at baseline and post-neoadjuvant therapy was strongly prognostic in the overall population: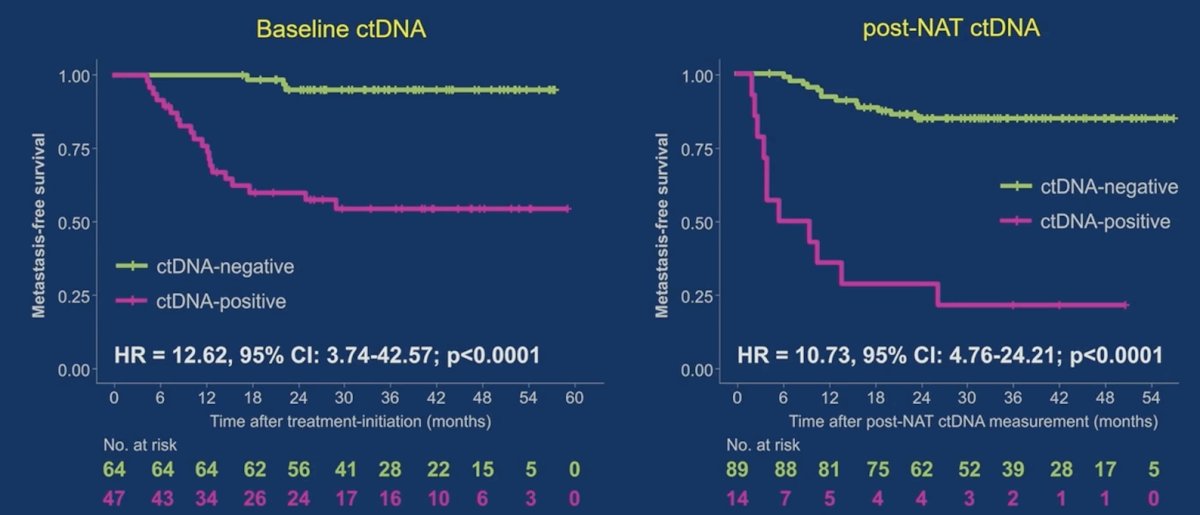
Additionally, ctDNA dynamics during treatment were prognostic in the overall population: 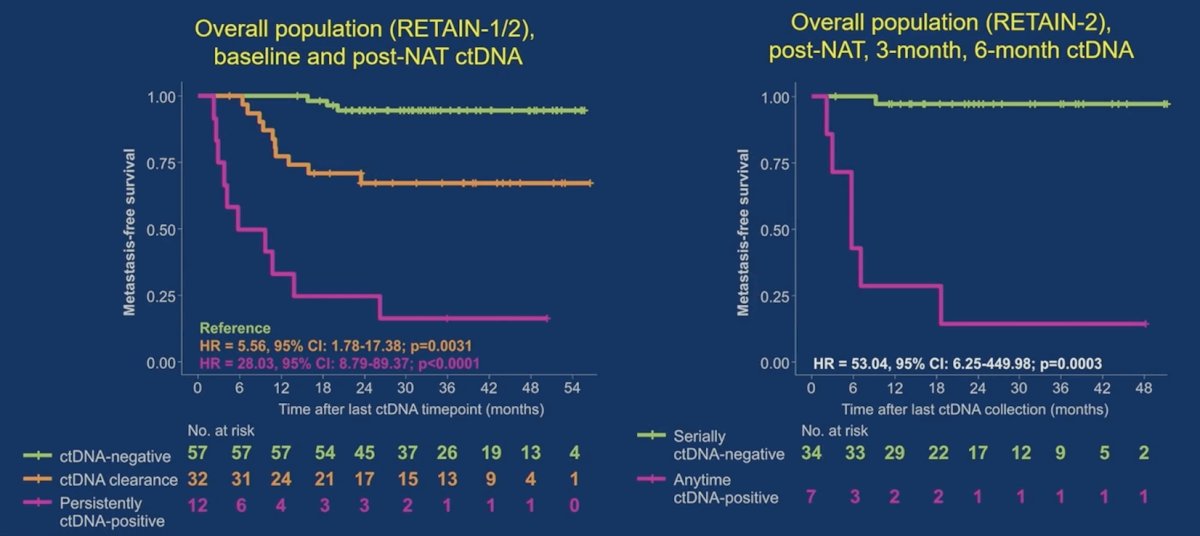
Similar outcomes in ctDNA negative patients were noted regardless of treatment (active surveillance or cystectomy):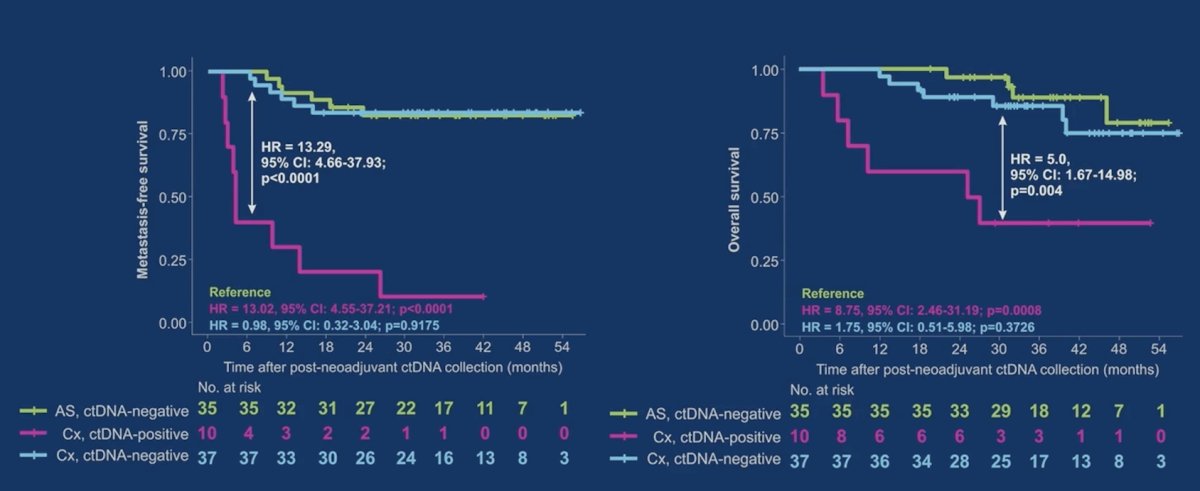
Among cystectomy patients, post-neoadjuvant therapy ctDNA status provided prognostic information beyond pathologic staging: 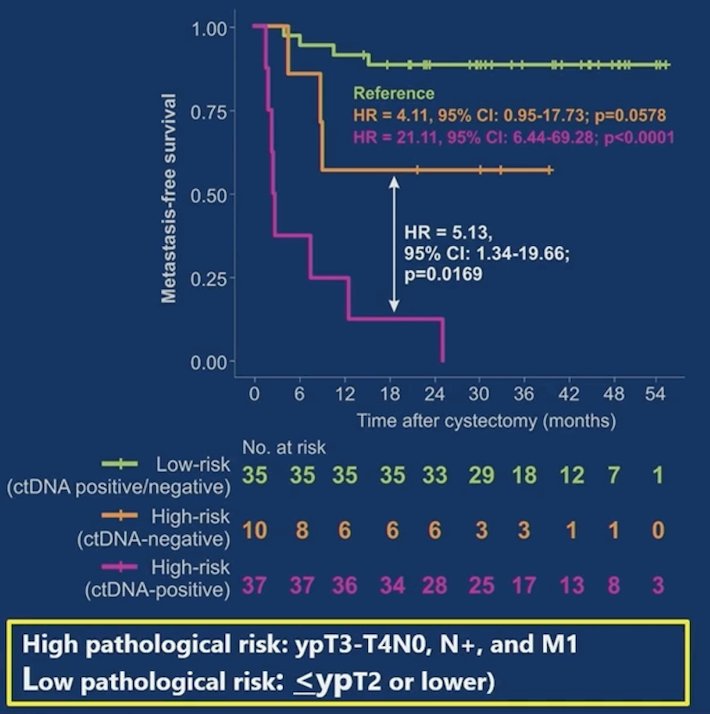
Moreover, post-neoadjuvant therapy ctDNA positivity predicted residual disease, but ctDNA negativity did not predict ypT0 in cystectomy patients: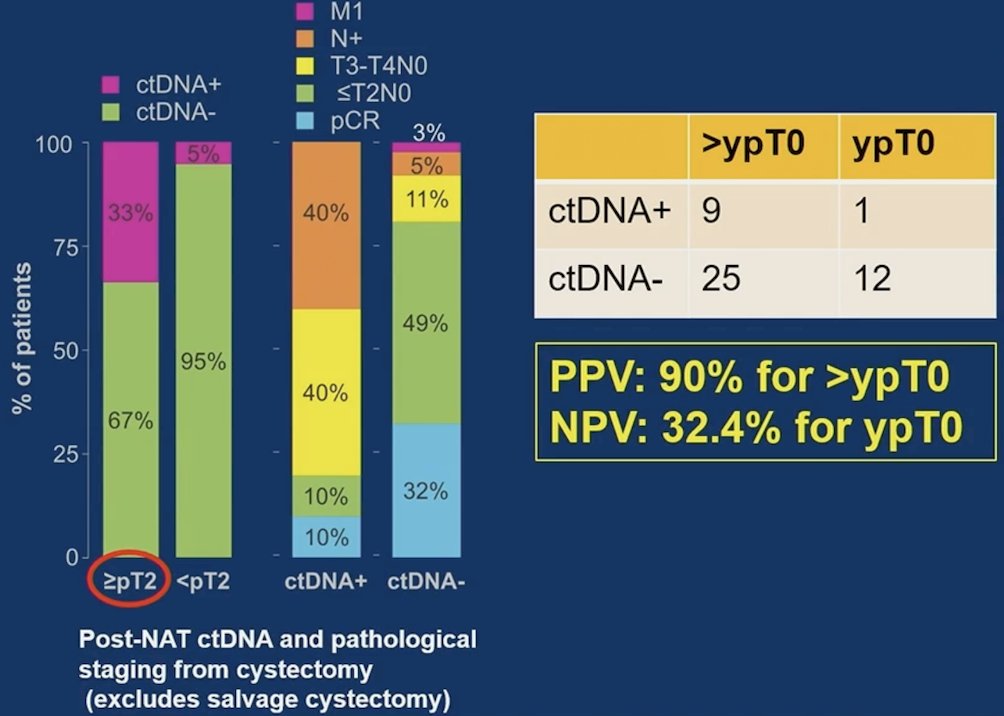
Dr. Ghatalia also notes that post-neoadjuvant therapy ctDNA status predicts systemic control, but not local control, among active surveillance patients: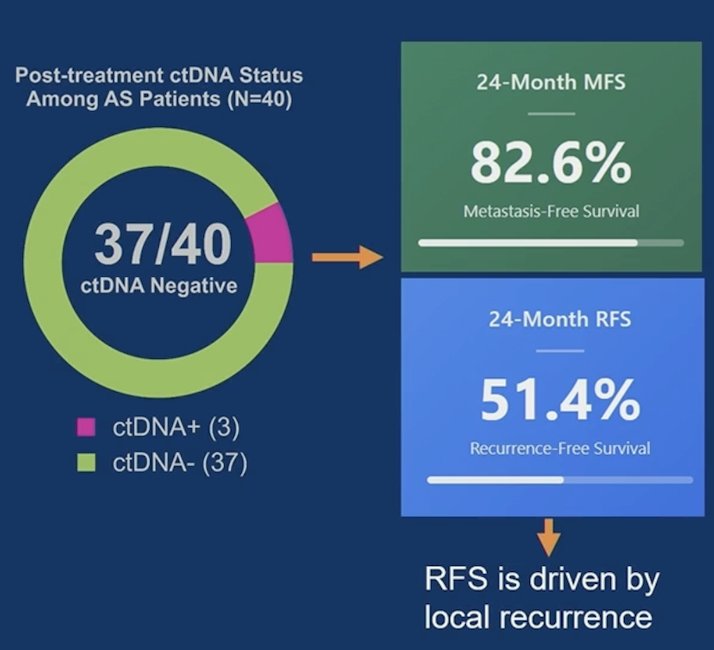
Additionally, post-neoadjuvant therapy ctDNA status predicts metastatic control but not local control in active surveillance patients: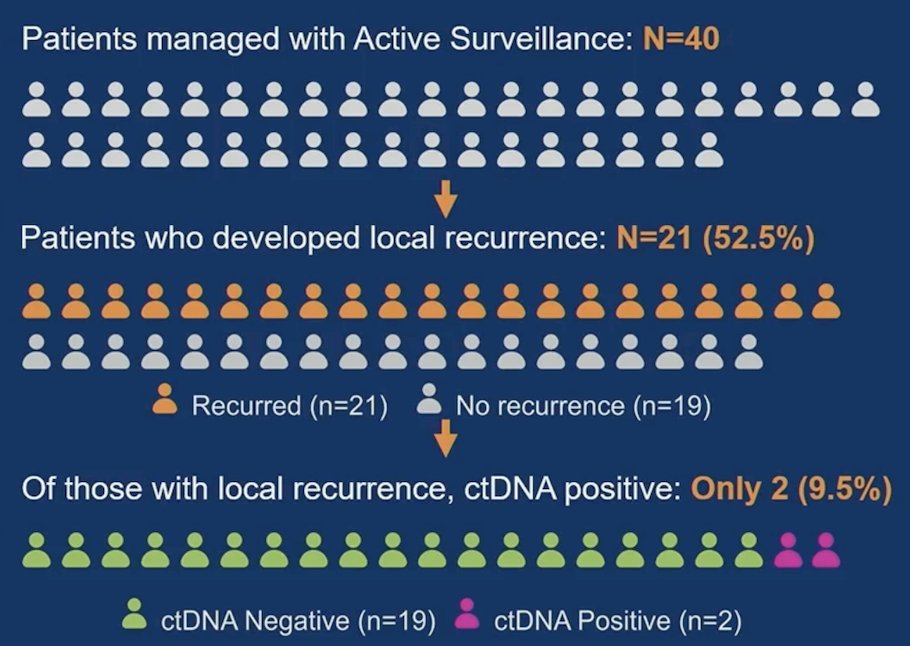
Dr. Ghatalia concluded her presentation discussing an integrated analysis of the RETAIN trials assessing ctDNA to guide response-adapted bladder preservation in muscle invasive bladder cancer with the following take-home points:
- The primary endpoint in RETAIN-2 was met
- ctDNA was prognostic for systemic disease control
- ctDNA positivity associated with a 10.7x higher risk of inferior metastasis-free survival (p<0.0001)
- ctDNA positivity was associated with poor outcomes despite cystectomy
- Future bladder preservation strategies should include multimodal surveillance
- ctDNA does not reliably capture residual bladder disease or local recurrence
- Future trials must integrate ctDNA + clinical restaging + urinary biomarkers
Presented by: Pooja Ghatalia, MD, Oncologist, Fox Chase Cancer Center, Philadelphia, PA
Reference: