(UroToday.com) The 2026 GU ASCO annual meeting featured a urothelial carcinoma session and a presentation by Dr. Thomas Powles discussing results from RC48G001, a phase 2 study of disitamab vedotin in HER2-expressing previously treated advanced urothelial carcinoma. Treatment options for locally advanced or metastatic urothelial carcinoma in the second-line setting and beyond remain limited.
Approximately 50 to 80% of patients with locally advanced or metastatic urothelial carcinoma have tumors that express HER2, underscoring the potential benefit of this biomarker for selecting patients who may benefit from HER2-targeted therapies. Disitamab vedotin is a HER2-directed antibody drug conjugate, comprising a humanized HER2-directed monoclonal antibody, disitamab, conjugated to the microtubule-disrupting agent MMAE via a protease-cleavable mc-vc linker. Disitamab vedotin has demonstrated promising antitumor activity and a manageable safety profile as monotherapy in participants with HER2-expressing (IHC 1+ or greater) locally advanced or metastatic urothelial carcinoma in clinical trials conducted in China.1 At ASCO GU 2026, Dr. Powles and colleagues presented the primary efficacy and safety findings from Cohorts A and B of the global, phase 2 RC48G001 trial, which evaluated disitamab vedotin monotherapy in previously treated participants with HER2-expressing locally advanced or metastatic urothelial carcinoma.
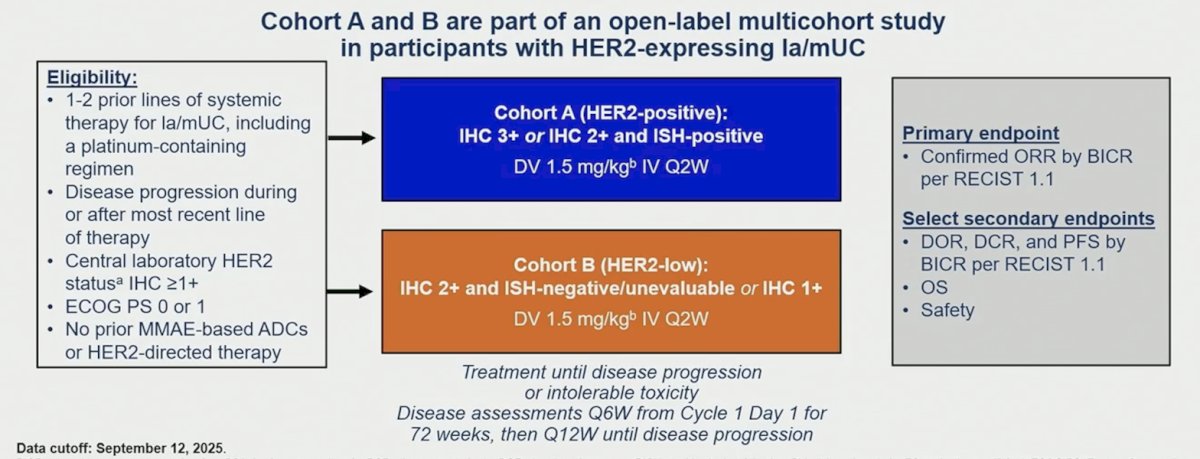
RC48G001 is a global, multicohort, single-arm, open-label, phase 2 study that enrolled patients with locally advanced or metastatic urothelial carcinoma who received 1-2 prior systemic therapies (including a platinum-containing regimen). HER2 expression was determined by the central laboratory using the VENTANA HER2 IHC and HER2 Dual ISH DNA Probe Cocktail assays. The two cohorts were as follows:
– Cohort A: HER2-positive locally advanced or metastatic urothelial carcinoma, defined as IHC 3+, or IHC 2+/ISH-positive
– Cohort B: HER2-low locally advanced or metastatic urothelial carcinoma, defined as IHC 2+/ISH-negative or unevaluable, or IHC 1+
Patients received 1.5 mg/kg disitamab vedotin monotherapy IV once per 2-week cycle. The primary endpoint was confirmed objective response rate per RECIST 1.1 by blinded independent central review, and secondary endpoints included duration of response, disease control rate, progression-free survival (all per RECIST 1.1 by blinded independent central review), overall survival, and safety:
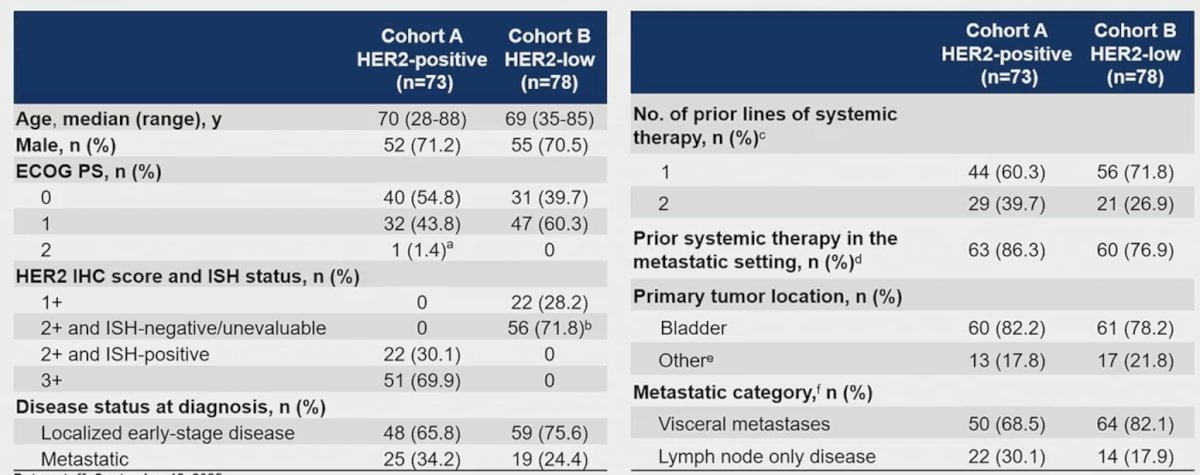
Overall, there were 293 patients screened for enrollment, with 151 patients enrolled, including 73 in Cohort A and 78 in Cohort B:

Baseline characteristics are highlighted in the following table; notably, 54.8% and 39.7% of patients had ECOG performance status 0, and 68.5% and 82.1% had visceral disease in each cohort, respectively. Cohort A included 69.9% patients with IHC 3+ and 30.1% patients with IHC 2+/ISH-positive locally advanced or metastatic urothelial carcinoma. Cohort B included 28.2% patients with IHC 1+ and 69.2% patients with IHC 2+/ISH-negative locally advanced or metastatic urothelial carcinoma:
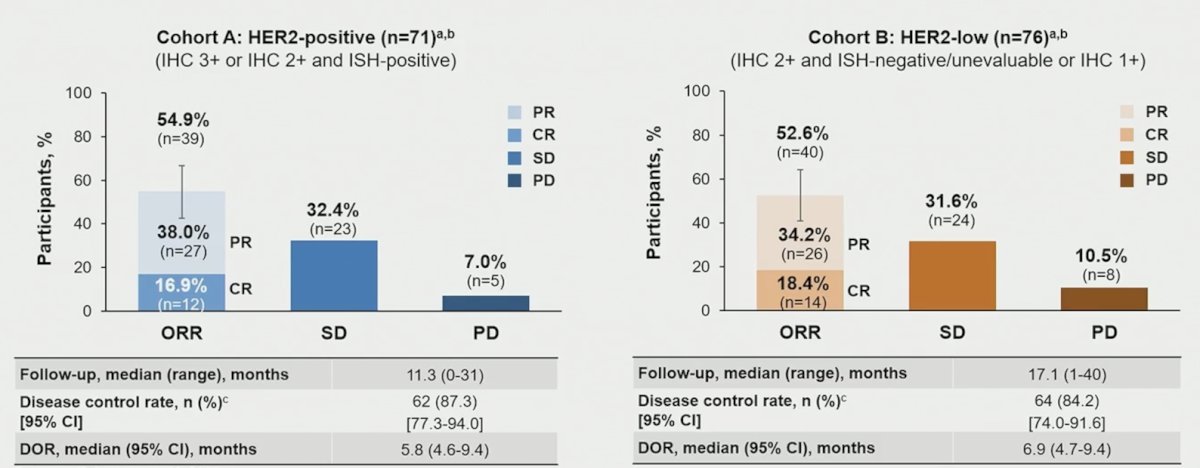
The median follow-up was 11.3 months for Cohort A and 17.1 months for Cohort B, and patients received a median of 9 disitamab vedotin cycles in both cohorts. Confirmed objective response rate per blinded independent central review was 54.9%, with a complete response rate of 16.9%, in Cohort A, and 52.6%, with a complete response rate of 18.4%, in Cohort B:
Complete response was observed in patients primarily with IHC 2+/3+ tumors, those with visceral metastasis or lymph node only disease, and those with or without prior radical surgery:

For the best percentage change in the sum of diameters from baseline, responses were achieved across HER2 expression levels:
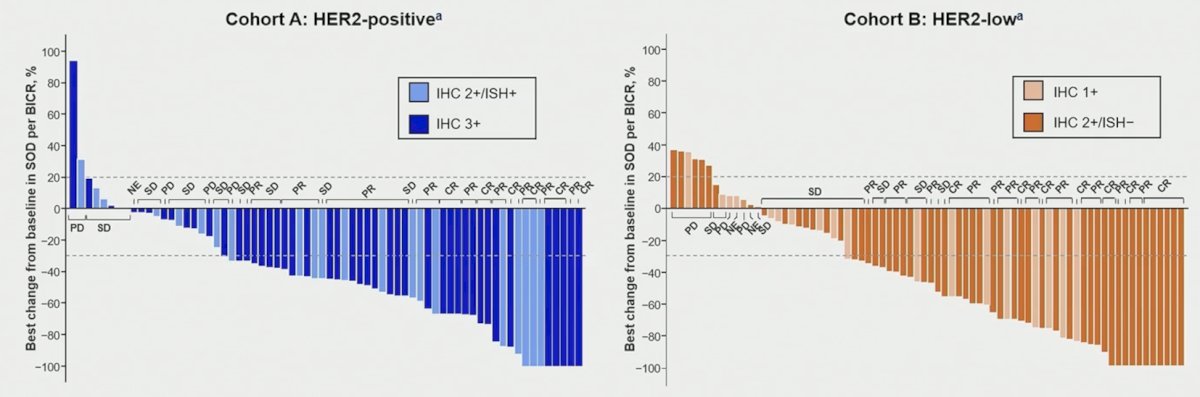
Objective response rate was consistent across subgroups, including those with different levels of HER2 expression. A numerically higher objective response rate was observed in the subgroup with lymph node metastases for both cohorts, and the objective response rate was similar in subgroups with upper versus lower tract primary tumors, 1 versus 2 prior lines of therapy, and across HER2 expression levels:

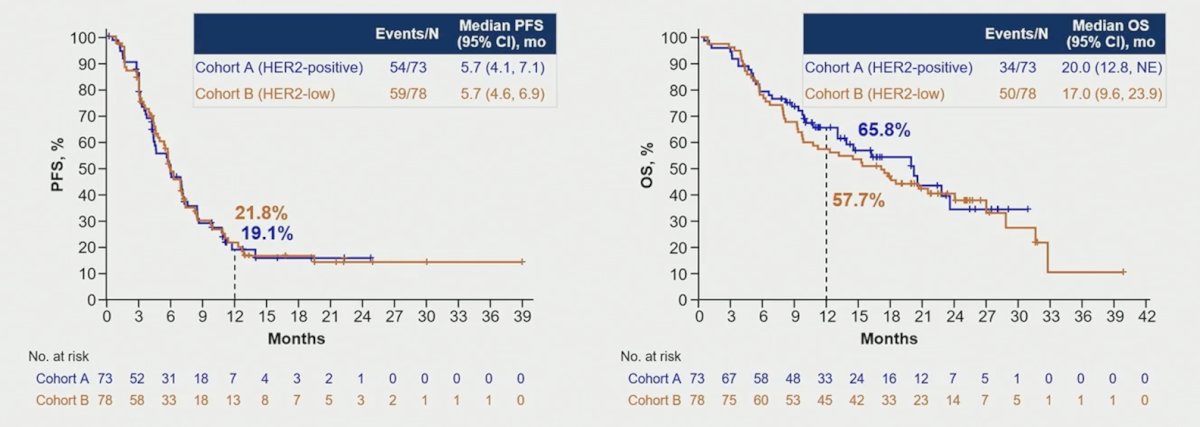
The median progression-free survival by blinded independent central review was 5.7 months in both cohorts, and the median overall survival was 20.0 months and 17.0 months in Cohort A and B, respectively:
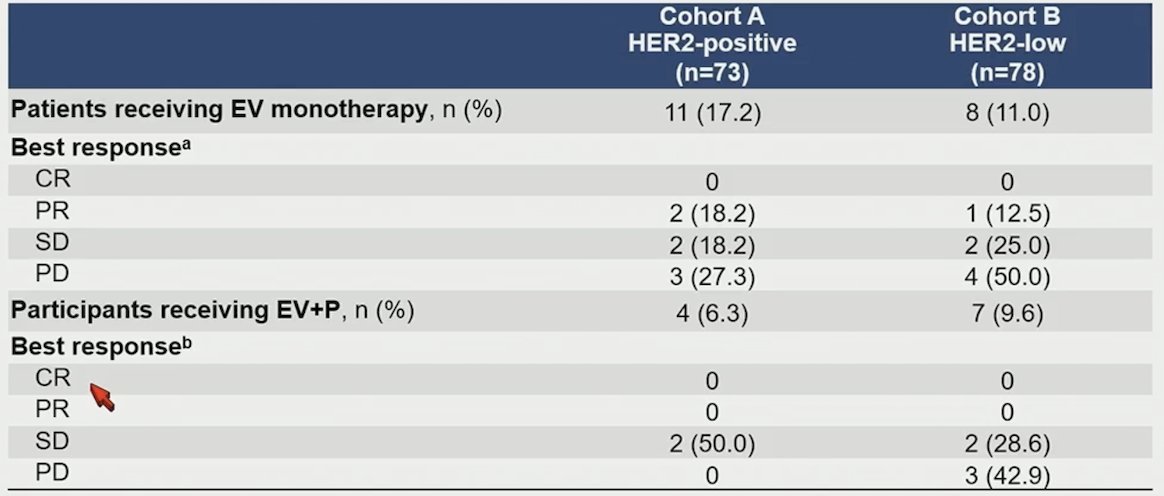
Approximately half of the patients received subsequent therapy, which included enfortumab vedotin-based therapy:

Specific to patients receiving subsequent enfortumab vedotin-based therapy, clinical activity was observed in these patients after discontinuation of disitamab vedotin. For those receiving subsequent enfortumab vedotin monotherapy, 2 of 11 in Cohort A and 1 of 8 in Cohort B achieved a partial response. For those receiving subsequent enfortumab vedotin + pembrolizumab, 2 of 4 in Cohort A and 2 of 7 in Cohort B achieved stable disease:
Grade ≥3 treatment-related adverse events occurred in 62 (41.1%) patients, with fatigue (13.9%) being the most common:
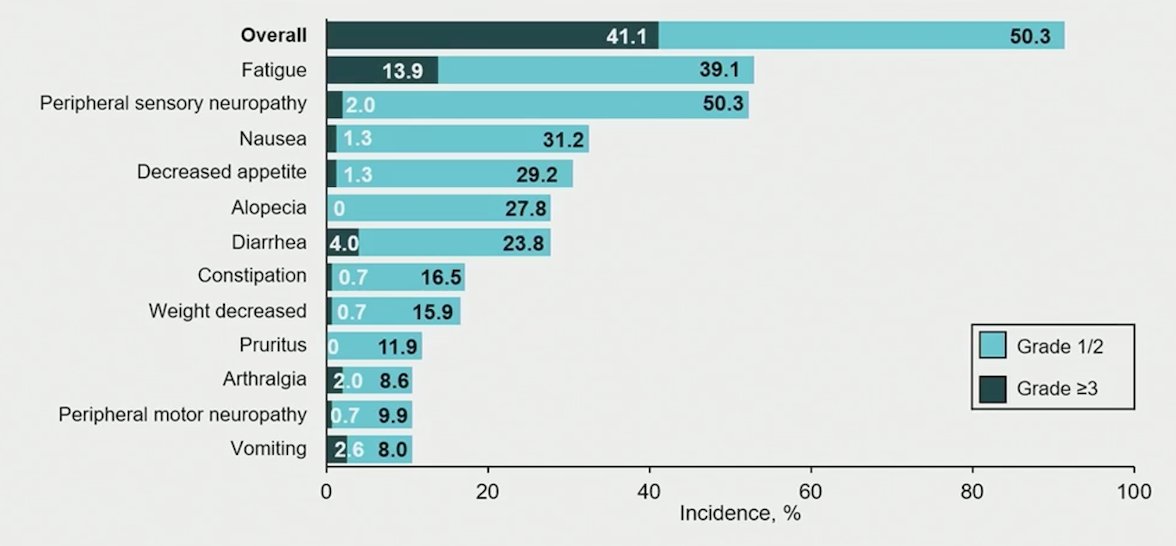
Overall, 16.6% of patients discontinued treatment due to adverse events, most commonly peripheral sensory neuropathy (6.0%):

Dr. Powles concluded his presentation discussing results from RC48G001, a phase 2 study of disitamab vedotin in HER2-expressing previously treated advanced urothelial carcinoma, with the following take-home points:
- Disitamab vedotin demonstrated clinically meaningful antitumor activity consistently across HER2 expression levels in previously treated participants with HER2-expressing locally advanced or metastatic urothelial carcinoma:
- The confirmed objective response rate was >52% and complete response rate was >16% in both the HER2-positive and HER2-low cohorts
- Overall survival outcome was favorable regardless of HER2 expression levels
- The observed safety profile was consistent with the known profile of disitamab vedotin: most treatment-related adverse events were low grade, with grade ≥3 treatment-related adverse events occurring in 41.1% of participants
- Toxicities were generally manageable, with 16.6% of participants discontinuing disitamab vedotin due to treatment-emergent adverse events
- Overall, the global study results are aligned with clinical trials conducted in China for disitamab vedotin in previously treated participants with HER2-expressing locally advanced or metastatic urothelial carcinoma
- A phase 3 study evaluating disitamab vedotin combined with pembrolizumab is ongoing in participants with HER2-expressing locally advanced or metastatic urothelial carcinoma
Presented by: Thomas Powles, MBBS, MRCP, MD, Professor of Genitourinary Oncology, Director, Barts Cancer Institute, Cancer Research UK Experimental Cancer Medicine Centre, Queen Mary University of London, London, United Kingdom
Reference:
- Sheng X, Zeng G, Zhang C, et al. Disitamab Vedotin plus Toripalimab in HER2-Expressing Advanced Urothelial Cancer. N Engl J Med. 2025 Dec 11;393(23):2324-2337.