(UroToday.com) The 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, was host to the Poster Session B: Prostate Cancer and Urothelial Carcinoma. Dr. Andrea Necchi presented the poster: Neoadjuvant sacituzumab govitecan + pembro, followed by response-adapted bladder sparing and adjuvant pembro, in patients with MIBC: SURE-02 primary analysis and biomarker results.
Dr. Necchi began by underscoring that radical cystectomy with neoadjuvant chemotherapy remains the standard of care for MIBC, yet approximately half of patients are ineligible for or decline cisplatin-based chemotherapy. Outcomes with cystectomy alone are suboptimal. Both pembrolizumab and sacituzumab govitecan have previously demonstrated activity as neoadjuvant monotherapies in the PURE-01 and SURE-01 trials, providing the rationale for combining these agents in a perioperative strategy.1,2
SURE-02 (NCT05535218) enrolled patients with cT2–T3bN0M0 MIBC who were ineligible for or refused cisplatin-based chemotherapy and were candidates for radical cystectomy. Patients received four cycles of pembrolizumab (200 mg day 1) plus sacituzumab govitecan (7.5 mg/kg days 1 and 8, every 3 weeks), followed by adjuvant pembrolizumab for up to 13 cycles. Importantly, a bladder-sparing approach was allowed for patients achieving a strictly defined clinical complete response, requiring a negative MRI and no residual viable tumor at reTURBT (ypT0). The primary endpoint was clinical complete response rate, with 19 cCRs required to meet the prespecified threshold in a two-stage design.
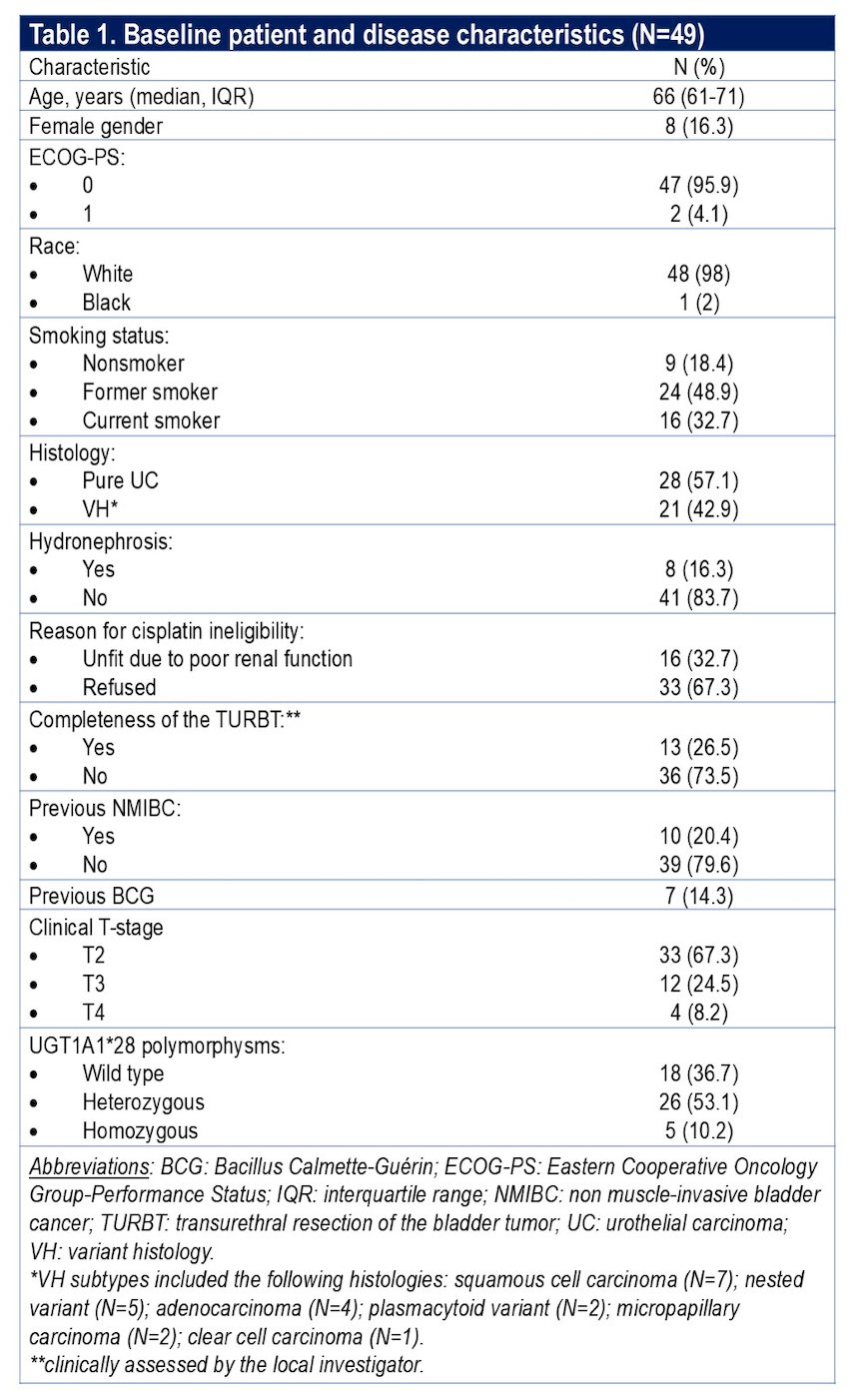
Between October 2023 and February 2025, 49 patients were treated and were evaluable for efficacy. Most patients had cT2 disease (67.3%), and 38.8% had centrally confirmed variant histology.
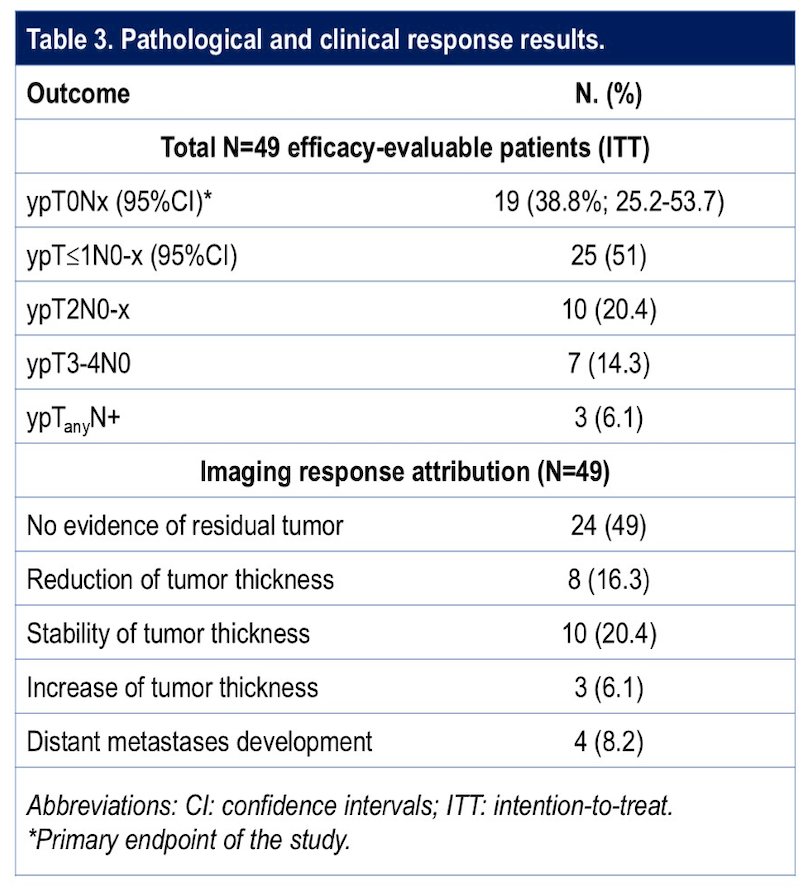
The clinical complete response rate was 38.8% (19 of 49 patients; 95% CI 25.2–53.8), meeting the predefined primary endpoint. All patients with cCR underwent reTURBT. The rate of ypT≤1N0/x was 51%, as shown below.
At 12 months, event-free survival defined as any high-grade relapse, progression, need for further bladder therapy, or death was 71% overall. Outcomes were strongly associated with response:
- 12-month EFS was 90.9% in patients achieving cCR
- 12-month EFS was 59.6% in non-cCR patients
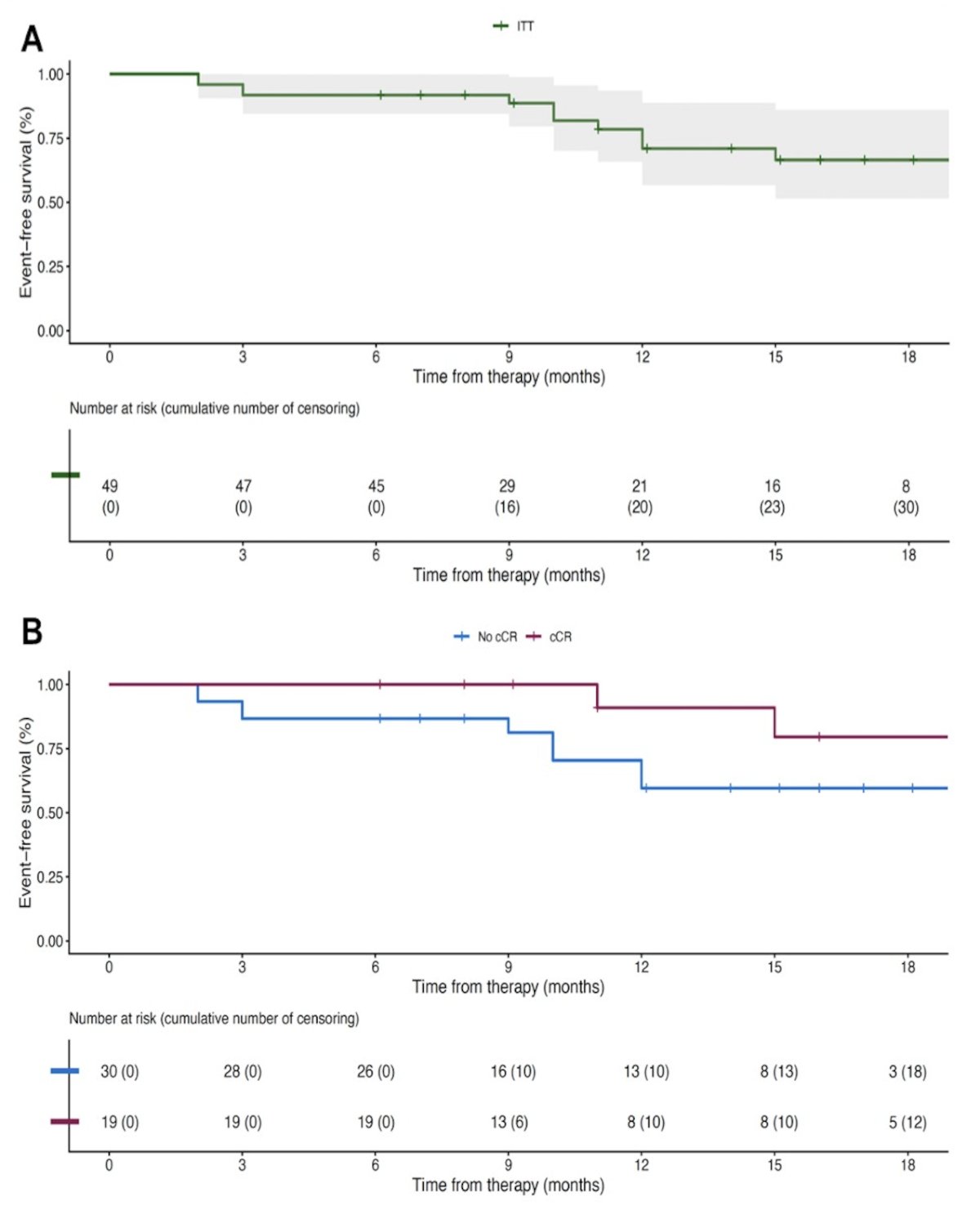
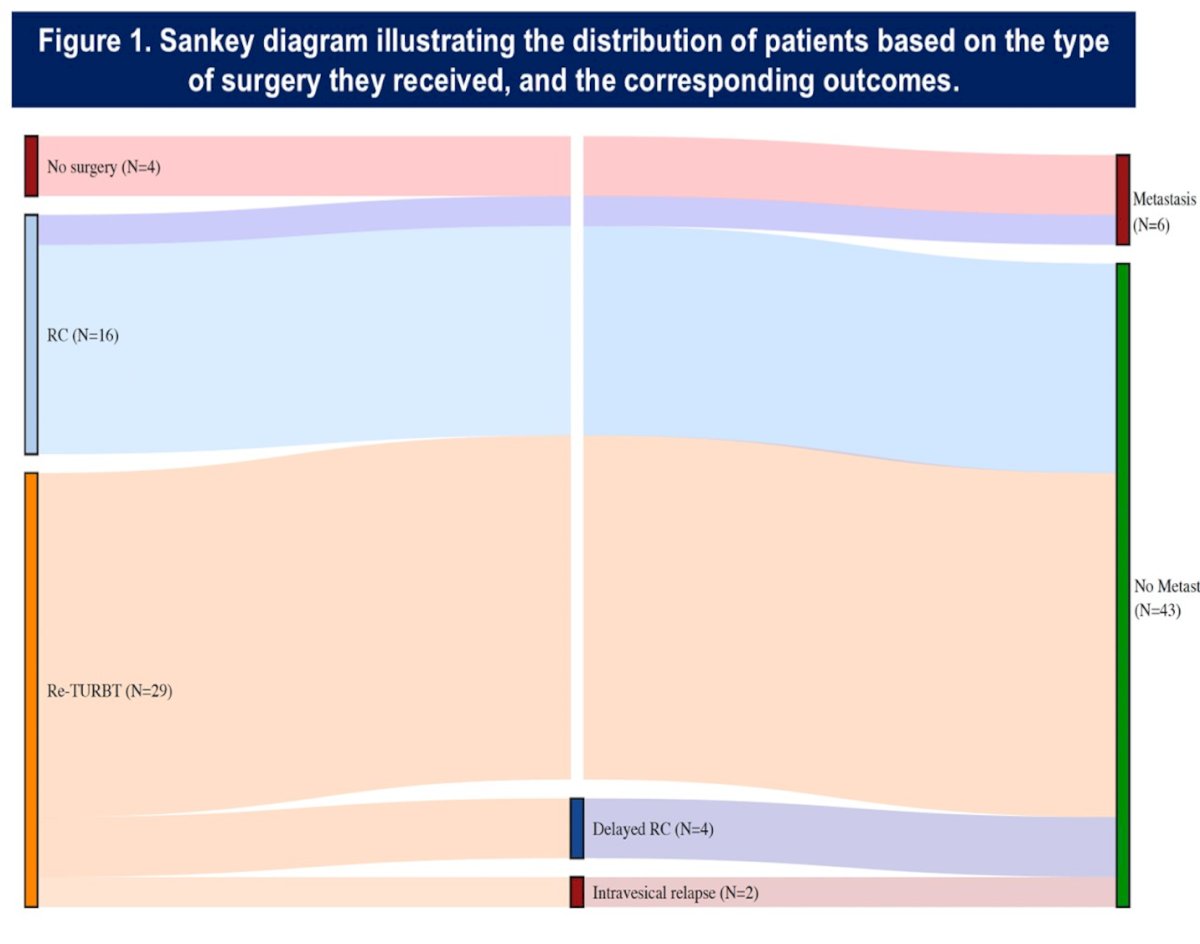
With a median follow-up of 14 months (IQR 8–18), all patients who achieved a clinical complete response (cCR) remained metastasis-free, although two experienced intravesical relapses (one ypT1 and one ypT2). In the ITT population, the 12-month metastasis-free survival (MFS) rate was 74.1% (95% CI 60.1–91.2), and the 12-month bladder-intact event-free survival (BI-EFS) rate was 38.4% (95% CI 24.9–59.1), increasing to 90.9% (95% CI 75.4–100) among cCR patients. Overall, six patients developed distant metastases. Among patients managed with re-TURBT, four underwent delayed radical cystectomy, and notably, none in the re-TURBT cohort developed distant metastatic disease as shown in the Sankey diagram below.
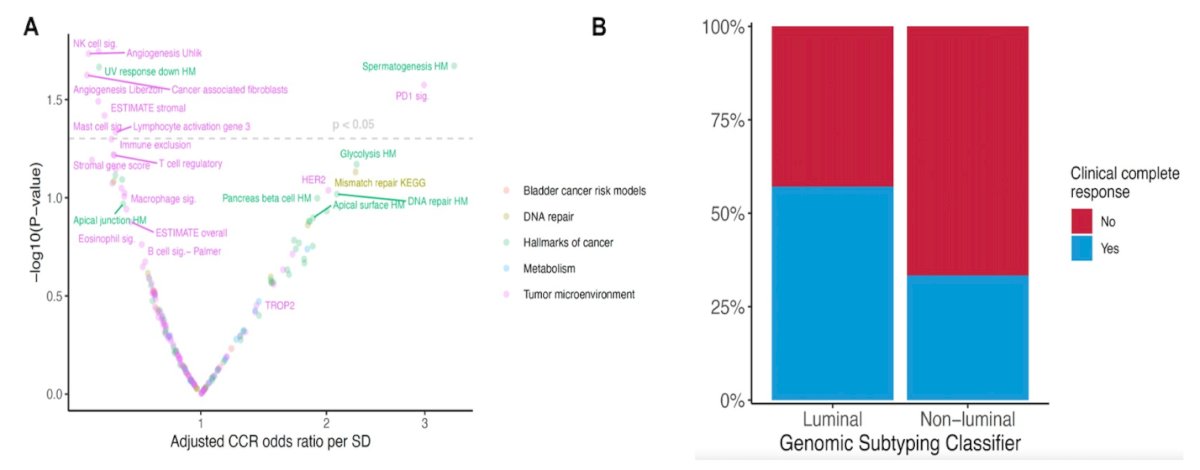
Multivariable analyses adjusted for clinical T stage demonstrated that several hallmark GRID signatures were significantly associated with clinical complete response (cCR). Immune-related and tumor microenvironment signatures such as NK-cell, lymphocyte activation, stromal, and angiogenesis-related pathways showed strong associations with response, whereas select DNA repair and metabolic pathways also demonstrated signal (as shown in the Volcano plot below). Additionally, genomic subtyping revealed differential response patterns, with luminal tumors exhibiting a higher proportion of cCR compared with non-luminal tumors, supporting the potential predictive value of molecular classification in baseline TURBT specimens.
The regimen was manageable from a safety standpoint. Grade 3 or higher treatment-related adverse events occurred in 16.3% of patients. No grade 5 treatment-related adverse events were observed.
Extensive biomarker analyses were performed on baseline tumor samples. Comprehensive genomic profiling showed ERBB2 mutations or amplifications in 42.1% of cCR patients compared with 13.7% of non-cCR patients. Median tumor mutational burden was higher in responders (12.1 vs 7.9). Transcriptomic analyses demonstrated that Luminal tumors had higher TROP2 and ERBB2 expression and greater enrichment of mismatch repair–related signatures. Clinical complete response rates were higher in Luminal subtypes (62%) compared with non-Luminal tumors (31%). A higher KEGG mismatch repair signature was significantly associated with longer event-free survival, with 100% 12-month EFS in that subgroup.
Dr. Necchi concluded:
- Neoadjuvant sacituzumab govitecan plus pembrolizumab achieved a compelling 38.8% clinical complete response rate in chemotherapy-ineligible MIBC.
- Approximately 40% of patients were able to pursue bladder preservation with sustained remission.
- The safety profile was manageable, with relatively low rates of high-grade toxicity.
- Biomarker analyses suggest enrichment of response in Luminal tumors, particularly those with ERBB2 alterations and higher mismatch repair signatures.
- These findings support the feasibility and safety of offering a patient-driven bladder sparing option, primarily dictated by clinical response to combined ADC and ICI treatment.
Presented by: Andrea Necchi, MD, IRCCS San Raffaele Hospital, Vita-Salute San Raffaele University, Milan, Italy
Written by: Julian Chavarriaga, MD – Urologic Oncologist, Department of Urology at Penn State Health. @chavarriagaj on Twitter during the 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026.
Related content: SURE-02 Trial Investigates Sacituzumab Plus Pembrolizumab in Bladder Preservation Approach - Andrea Necchi
References:
- Necchi A, Anichini A, Raggi D, Briganti A, Massa S, Lucianò R, Colecchia M, Giannatempo P, Mortarini R, Bianchi M, Farè E, Monopoli F, Colombo R, Gallina A, Salonia A, Messina A, Ali SM, Madison R, Ross JS, Chung JH, Salvioni R, Mariani L, Montorsi F. Pembrolizumab as Neoadjuvant Therapy Before Radical Cystectomy in Patients With Muscle-Invasive Urothelial Bladder Carcinoma (PURE-01): An Open-Label, Single-Arm, Phase II Study. J Clin Oncol. 2018 Dec 1;36(34):3353-3360. doi: 10.1200/JCO.18.01148. Epub 2018 Oct 20. PMID: 30343614.
- Brigida Anna Maiorano et al. First survival outcomes and biomarker results of SURE-01: Neoadjuvant sacituzumab govitecan (SG) monotherapy, followed by radical cystectomy (RC), in patients with muscle-invasive urothelial bladder cancer (MIBC). J Clin Oncol 43, 4591-4591(2025). DOI:10.1200/JCO.2025.43.16_suppl.4591