(UroToday.com) The 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026, was host to the Poster Session B: Prostate Cancer and Urothelial Carcinoma. Dr. Jeannie Hoffman-Censits presented the poster: Avelumab in combination with other anticancer agents as 1L maintenance treatment of advanced UC: Primary analysis from the JAVELIN Bladder Medley phase 2 trial.
Dr. Hoffman-Censits reviewed the role of avelumab first-line maintenance in advanced urothelial carcinoma, which is recommended for patients without progression after platinum-based chemotherapy, based on the phase 3 JAVELIN Bladder 100 trial. With at least two years of follow-up, avelumab plus best supportive care significantly improved overall survival compared with best supportive care alone, with a median OS of 23.8 versus 15.0 months (HR 0.76; p=0.0036), and improved progression-free survival, with a median PFS of 5.5 versus 2.1 months (HR 0.54; p<0.0001).1
She also highlighted the interim results from the phase 2 JAVELIN Bladder Medley trial, where avelumab combined with sacituzumab govitecan, a Trop-2–directed antibody–drug conjugate, improved PFS compared with avelumab monotherapy, meeting the primary endpoint. Median PFS was 11.17 months with the combination versus 3.75 months with avelumab alone (HR 0.49). (2) Although sacituzumab govitecan previously demonstrated activity in advanced urothelial carcinoma, its accelerated approval in the post–platinum and post–PD-(L)1 setting was voluntarily withdrawn in October 2024 after the TROPiCS-04 phase 3 trial failed to show an overall survival benefit over chemotherapy, potentially influenced by early toxicity-related complications. In addition to the avelumab plus sacituzumab arm, JAVELIN Bladder Medley also evaluated avelumab in combination with M6223, an anti-TIGIT antibody, and NKTR-255, a polymer-conjugated IL-15 agonist, in the first-line maintenance setting.
For this analysis of the JAVELIN Bladder Medley trial, eligible patients had unresectable locally advanced or metastatic urothelial carcinoma, ECOG performance status 0–1, and no progression after 4–6 cycles of first-line platinum-based chemotherapy. Patients were randomized 2:2:2:1 to receive 1L maintenance treatment with avelumab + SG, avelumab + M6223, avelumab + NKTR-255, or avelumab monotherapy (control), stratified by the presence of visceral metastases. The primary endpoints were investigator-assessed progression-free survival and safety; overall survival was a secondary endpoint. For time-to-event analyses, outcomes in the monotherapy arm were extended using propensity score–weighted data from JAVELIN Bladder 100 per protocol. The study design is shown below.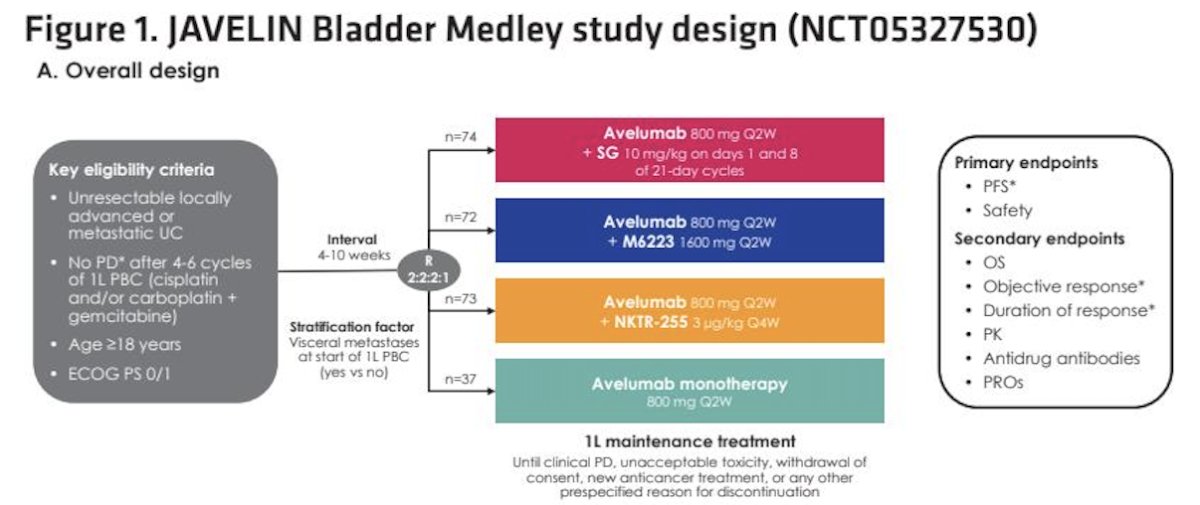
Per protocol, progression-free and overall survival data for the avelumab monotherapy arm were extended using propensity score–weighted data from the JAVELIN Bladder 100 phase 3 trial. Baseline characteristics were used to weight the JAVELIN Bladder 100 population to account for differences between study cohorts, and the data were subsequently downweighted to reflect the number of randomized patients in the Medley trial, creating an extended control arm for comparative PFS and OS analyses.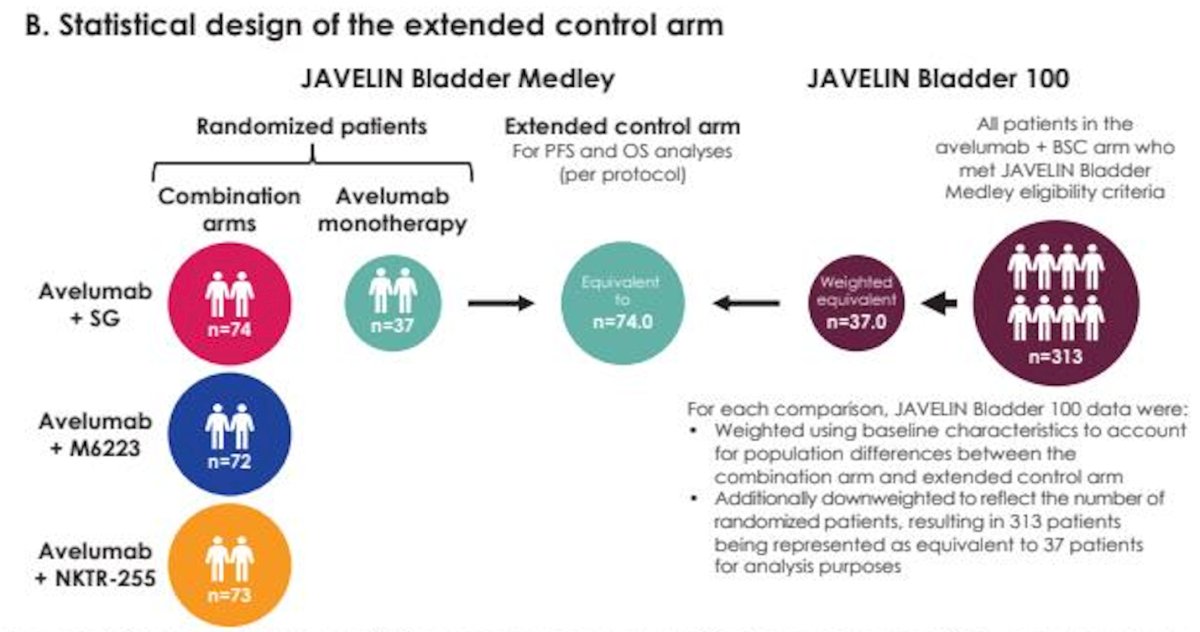
In total, 256 patients were randomized across the four study arms. Baseline characteristics were generally well balanced between treatment groups, including age, ECOG performance status, PD-L1 status, metastatic burden, prior platinum-based chemotherapy regimen, and best response to first-line chemotherapy. Approximately half of patients had visceral disease at study entry, and most had achieved a complete or partial response to first-line platinum-based chemotherapy.
At the data cutoff of April 28, 2025, the median follow-up for overall survival was at least 16.8 months across all arms, supporting the maturity of the survival analyses.

In the Avelumab + SG arm, median progression-free survival was 11.17 months with avelumab plus SG compared with 3.75 months with avelumab monotherapy, corresponding to a hazard ratio (HR, 0.54 [95% CI, 0.36-0.81]). This represents a clinically meaningful improvement in PFS with the combination. Overall survival data were immature at the time of analysis. Median OS had not yet been reached in the combination arm and was 22 months in the monotherapy arm, with a hazard ratio of 0.69 (95% CI 0.41–1.17).![In the Avelumab + SG arm, median progression-free survival was 11.17 months with avelumab plus SG compared with 3.75 months with avelumab monotherapy, corresponding to a hazard ratio (HR, 0.54 [95% CI, 0.36-0.81]). This represents a clinically meaningful improvement in PFS with the combination. Overall survival data were immature at the time of analysis. Median OS had not yet been reached in the combination arm and was 22 months in the monotherapy arm, with a hazard ratio of 0.69 (95% CI 0.41–1.17).](/images/com-doc-importer/248-asco-gu-2026/asco-gu-2026-avelumab-in-combination-with-other-anticancer-agents-as-1l-maintenance-treatment-of-advanced-uc-primary-analysis-from-the-javelin-bladder-medley-phase-2-trial/image-4.jpg)
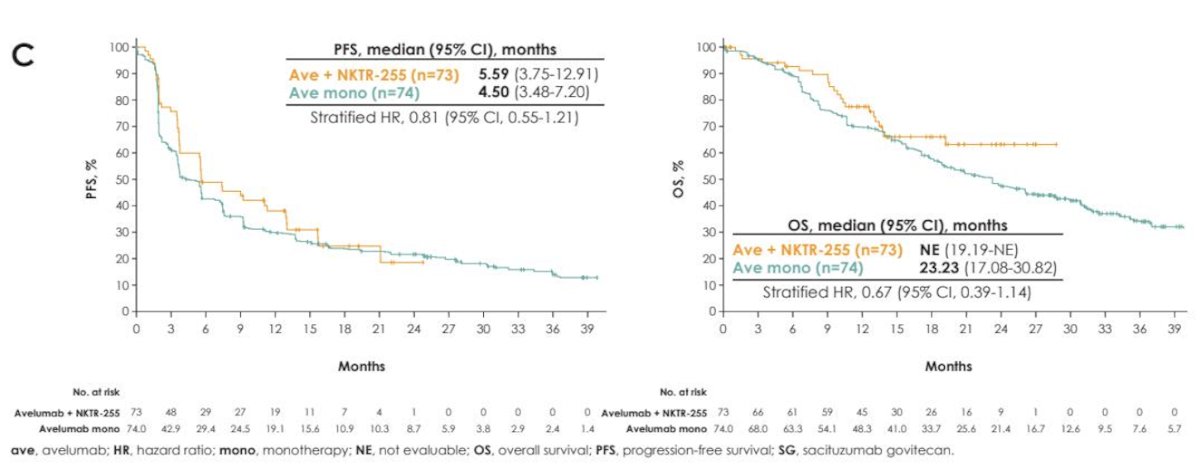
In the avelumab plus M6223 arm compared with avelumab monotherapy, median progression-free survival was 5.42 versus 4.50 months (HR 0.95; 95% CI 0.64–1.39). Median overall survival was not reached in the combination arm compared with 23.23 months with avelumab alone (HR 0.75; 95% CI 0.44–1.27), suggesting a numerical OS improvement without a clear PFS advantage.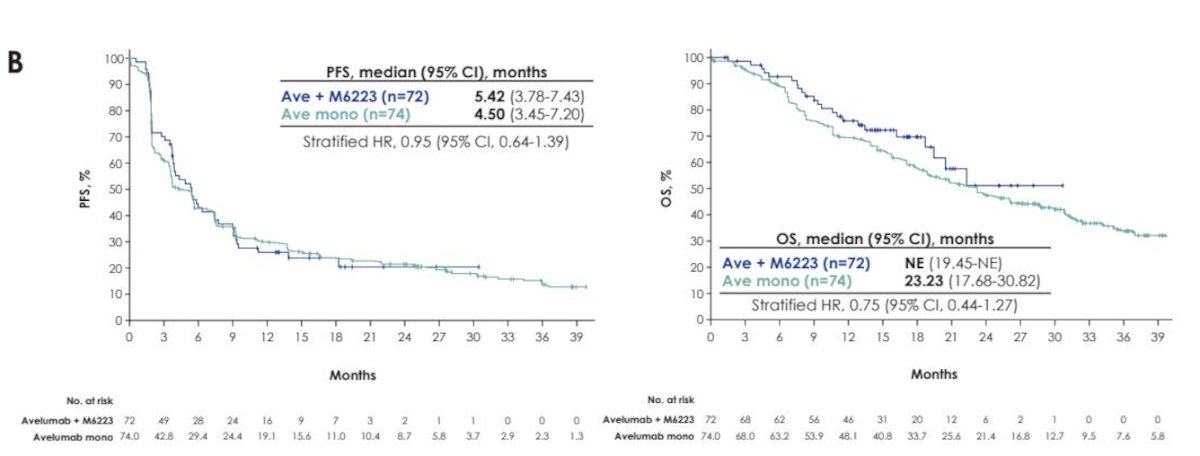
Moreover, in the avelumab plus NKTR-255 arm compared with avelumab monotherapy, median progression-free survival was 5.59 versus 4.50 months (HR 0.81; 95% CI 0.55–1.21). Median overall survival was not reached in the combination arm compared with 23.23 months in the monotherapy arm (HR 0.67; 95% CI 0.39–1.14), indicating a trend toward improved OS with the addition of NKTR-255.
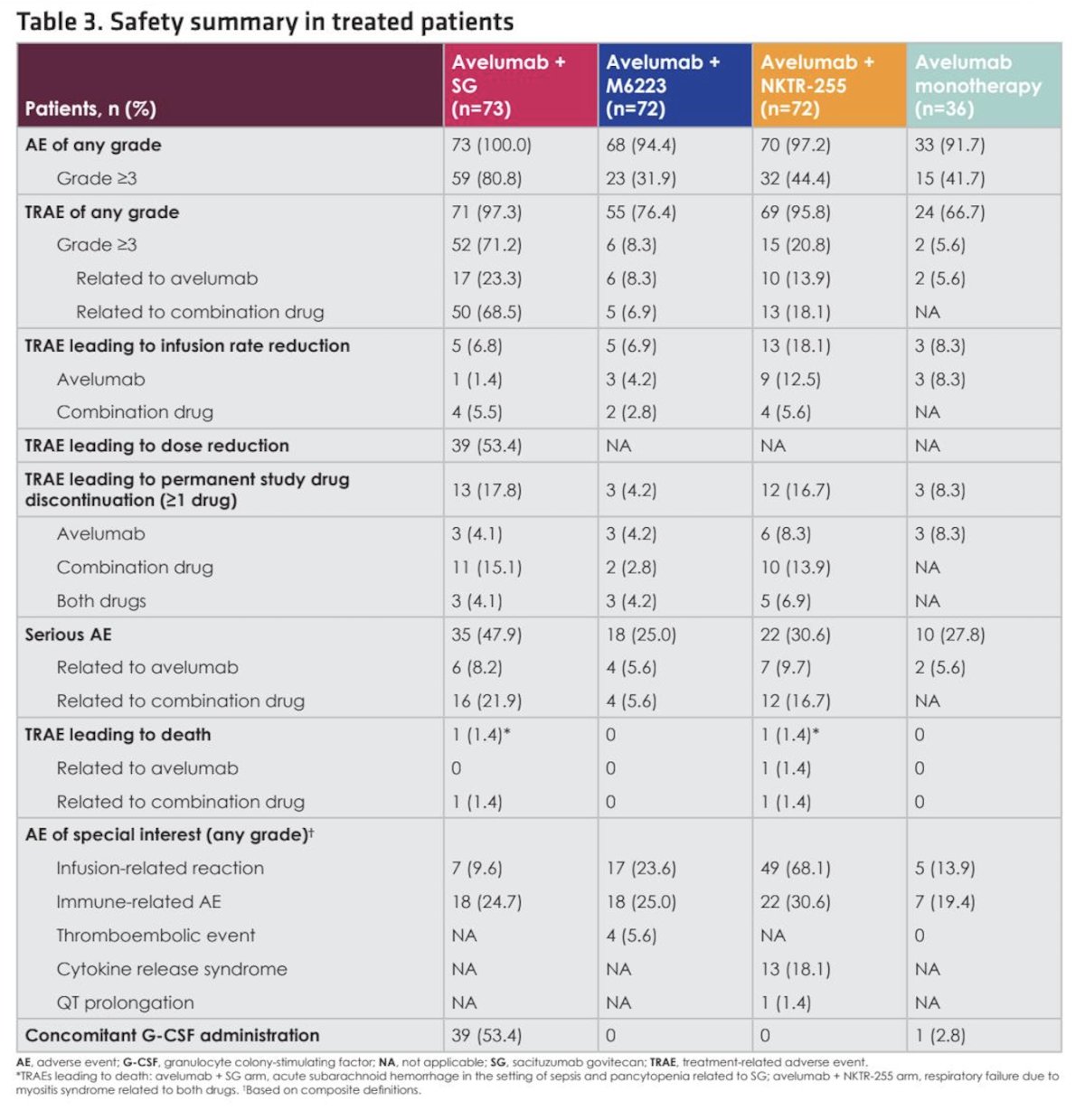
As expected, toxicity rates were higher with combination therapy. Treatment-related adverse events of any grade occurred in 97.3% of patients receiving avelumab plus sacituzumab govitecan, 76.4% in the avelumab plus M6223 arm, and 95.8% in the avelumab plus NKTR-255 arm, compared with 66.7% in the avelumab monotherapy arm. Grade 3 or higher treatment-related adverse events occurred in 8.3% of patients receiving avelumab plus M6223, 20.8% in the avelumab plus NKTR-255 arm, and 5.6% in the avelumab monotherapy arm, as shown in the table below.
Lastly, the toxicity profile varied by combination partner. In the avelumab plus sacituzumab govitecan arm, combination drug–related adverse events included alopecia, diarrhea, neutropenia, nausea, anemia, and febrile neutropenia, with higher rates of hematologic toxicity compared with other arms. In the avelumab plus M6223 arm, treatment-related events were generally consistent with immune checkpoint inhibition, including pruritus and asthenia. In the avelumab plus NKTR-255 arm, infusion-related reactions and cytokine release syndrome were observed, reflecting the immunostimulatory mechanism of the IL-15 agonist. Overall, adverse events were manageable and aligned with the expected safety profiles of the respective agents.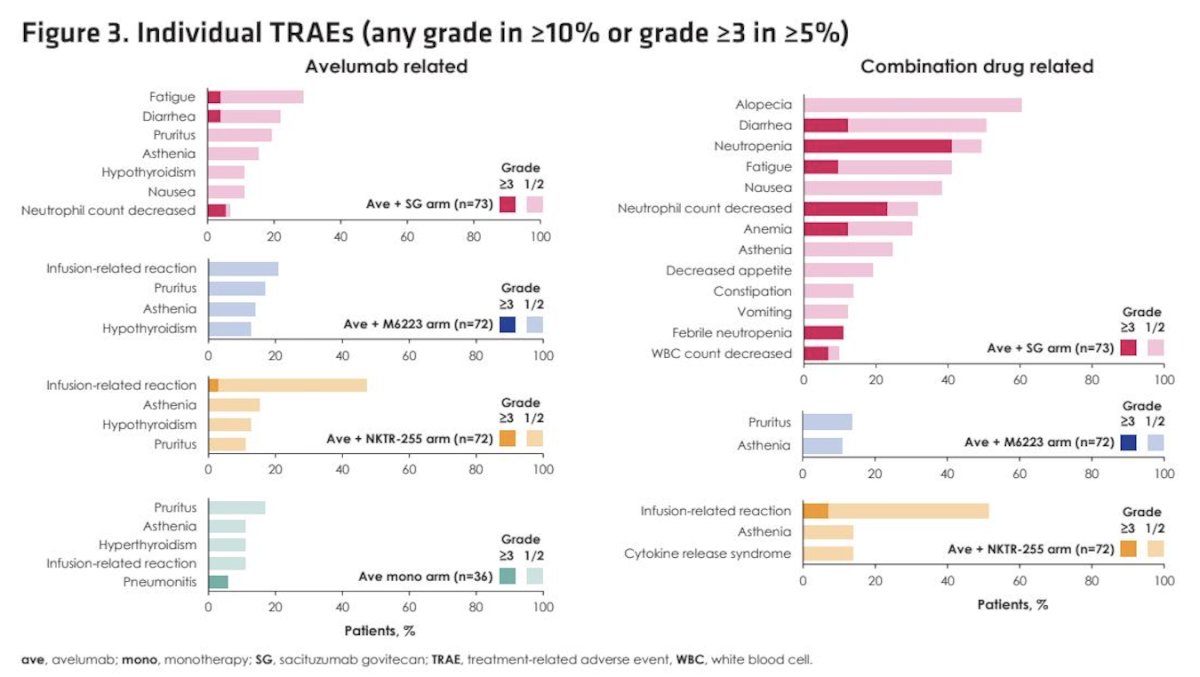
Dr. Hoffman-Censits concluded her presentation with the following key messages:
- In the primary analysis of JAVELIN Bladder Medley, first-line maintenance with avelumab plus sacituzumab govitecan significantly improved progression-free survival compared with avelumab monotherapy (HR 0.54), consistent with prior interim results.
- The addition of M6223 or NKTR-255 to avelumab did not demonstrate a clear PFS benefit over monotherapy, with hazard ratios of 0.95 and 0.81, respectively.
- Overall survival data remain immature; however, trends favored all combination arms over avelumab alone, including avelumab plus sacituzumab govitecan, avelumab plus M6223, and avelumab plus NKTR-255.
- Grade 3 or higher treatment-related adverse events were more frequent with combination therapy, particularly with avelumab plus sacituzumab govitecan, but no new safety signals were identified.
- Ongoing follow-up for survival and safety, along with translational analyses, will further clarify the role of these combinations.
- Overall, these findings support continued investigation of avelumab-based combinations as a strategy to improve outcomes in advanced urothelial carcinoma.
Presented by: Jeannie Hoffman-Censits, MD, The Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins, Johns Hopkins Greenberg Bladder Cancer Institute, Baltimore, MD
Written by: Julian Chavarriaga, MD – Urologic Oncologist, Department of Urology at Penn State Health. @chavarriagaj on Twitter during the 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026.
Related content: JAVELIN Bladder Medley: Evaluating Checkpoint Inhibitor Combinations After Chemotherapy - Jeannie Hoffman-Censits
- Powles T, Park SH, Caserta C, Valderrama BP, Gurney H, Ullén A, Loriot Y, Sridhar SS, Sternberg CN, Bellmunt J, Aragon-Ching JB, Wang J, Huang B, Laliberte RJ, di Pietro A, Grivas P. Avelumab First-Line Maintenance for Advanced Urothelial Carcinoma: Results From the JAVELIN Bladder 100 Trial After ≥2 Years of Follow-Up. J Clin Oncol. 2023 Jul 1;41(19):3486-3492. doi: 10.1200/JCO.22.01792. Epub 2023 Apr 18. PMID: 37071838; PMCID: PMC10306435.
- Hoffman-Censits J, Tsiatas M, Chang PM, Kim M, Antonuzzo L, Shin SJ, Gakis G, Blais N, Kim SH, Smith A, Arranz Arija JA, Su YL, Zagouri F, Maruzzo M, Tournigand C, Forget F, Schneider A, Tyroller K, Jacob N, Grivas P, Valderrama BP. Avelumab plus sacituzumab govitecan versus avelumab monotherapy as first-line maintenance treatment in patients with advanced urothelial carcinoma: JAVELIN Bladder Medley interim analysis. Ann Oncol. 2025 Sep;36(9):1088-1095. doi: 10.1016/j.annonc.2025.05.010. Epub 2025 Jun 1. PMID: 40456670.