(UroToday.com) The 2025 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA between February 13th and 15th 2025, was host to the Poster Session A: Prostate Cancer. Dr. Abhiraj Saxena presented Abstract 128: Prevalence of adverse events following T-cell engaging bispecific antibodies (bsAbs) and chimeric antigen receptor (CAR) T-cell therapy in patients with metastatic castrate-resistant prostate cancer (mCRPC): A meta-analysis.
Dr. Saxena began their poster by highlighting the transformative potential of T-cell engaging bispecific antibodies (bsAbs) and chimeric antigen receptor (CAR) T-cell therapies in oncology. These immunotherapies have demonstrated remarkable success in treating hematologic malignancies, with multiple bsAbs and CAR-T products gaining FDA approval for diseases such as multiple myeloma and certain leukemias. More recently, bsAbs have been FDA-approved for uveal melanoma and small cell lung cancer, providing proof-of-concept that immune-based therapies beyond checkpoint inhibitors can be effective in solid tumors.
Given these advancements, bsAbs and CAR-T therapies are now being investigated for metastatic castration-resistant prostate cancer (mCRPC), an area where immune checkpoint inhibitors have shown limited efficacy historically. Ongoing clinical trials are exploring various bispecific constructs targeting prostate-specific membrane antigen (PSMA) or other prostate cancer-associated antigens, as well as CAR-T therapies engineered to enhance T-cell infiltration in the tumor microenvironment.
However, despite early signs of clinical activity, these therapies present multiple challenges that must be addressed for successful translation into routine practice. Key concerns include dose-limiting toxicities, ‘on-target, off-tumor’ effects that can impact normal tissues, and immune-effector cell-related toxicities such as cytokine release syndrome (CRS) and immune effector cell-associated neurotoxicity syndrome (ICANS). Managing these toxicities while maintaining efficacy remains a critical focus of ongoing research.
To better understand the safety profile of these emerging immunotherapies in prostate cancer, Dr. Saxena and colleagues conducted a systematic review analyzing publicly available safety data from ongoing clinical trials. Their review aims to provide insight into the frequency and severity of treatment-related adverse events, patterns of toxicity across different bispecific and CAR-T platforms, and strategies being implemented to mitigate risks while optimizing clinical benefit for patients with mCRPC.
Dr. Saxena and colleagues conducted a comprehensive electronic systematic search across multiple databases, including PubMed, CINAHL, Scopus, and Ovid, to identify phase I/II clinical trials evaluating bsAbs or CAR-T therapy in patients with mCRPC. Their search included all relevant studies reported prior to September 2024.
The primary focus of their analysis was on treatment-related adverse events (TRAEs), particularly comparing the prevalence and severity of toxicities observed with bsAbs versus CAR-T therapies. Given the inherent differences in mechanisms of action between these two immunotherapy platforms—bsAbs acting as immune cell engagers and CAR-T cells involving autologous T-cell modification—variability in toxicity profiles was anticipated.
To account for heterogeneity across studies, a random effects model from the “meta” package in R software was used for statistical analysis.
Dr. Saxena and colleagues identified a total of 11 phase I/II clinical trials evaluating bsAbs (11 trials, 511 patients) and CAR-T therapies (5 trials, 55 patients) in mCRPC. The mean patient age across all studies was 67 years. The table below summarizes the 17 trials included in this analysis.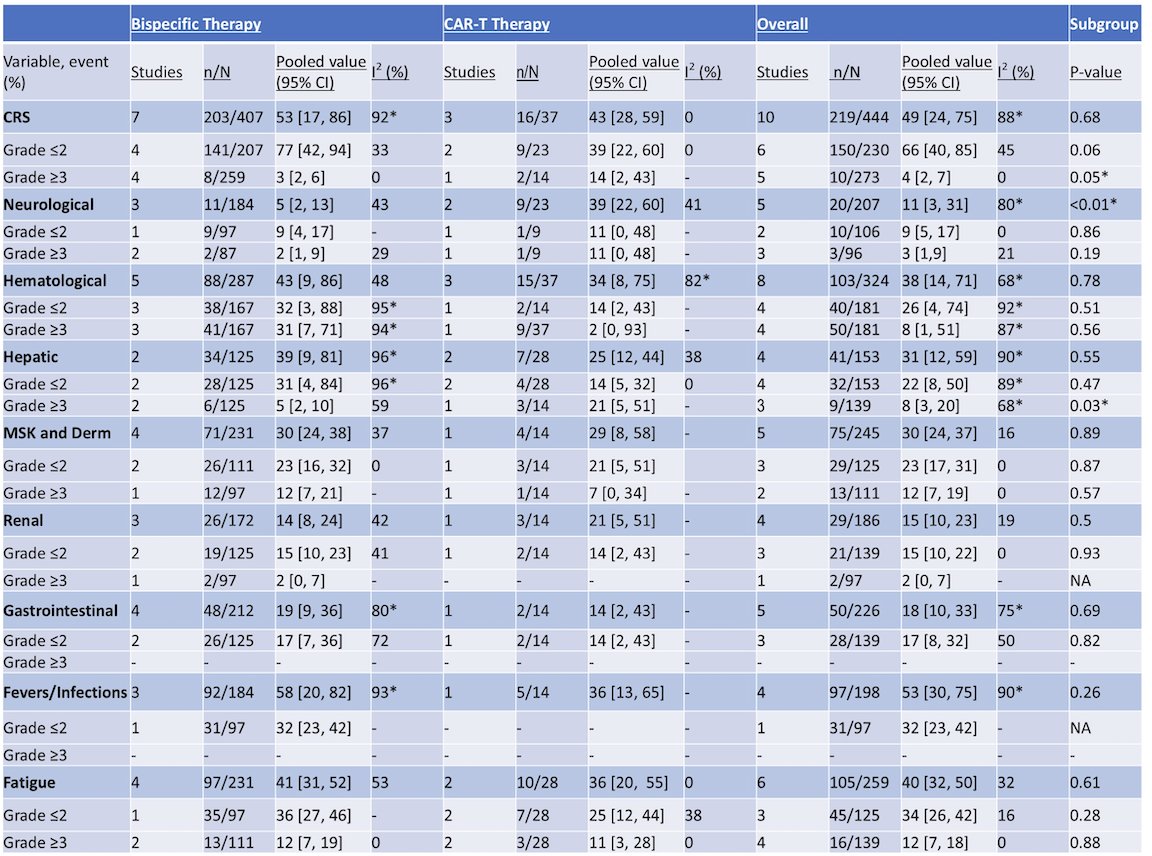
Cytokine Release Syndrome
CRS was reported in 49% of all patients, with a higher occurrence in those treated with bsAbs (53%) compared to CAR-T (43%). However, severe CRS (grade ≥3) was significantly more common in CAR-T patients (14%) compared to bsAbs (3%) (p=0.05), highlighting a greater risk of high-grade immune activation with CAR-T therapy.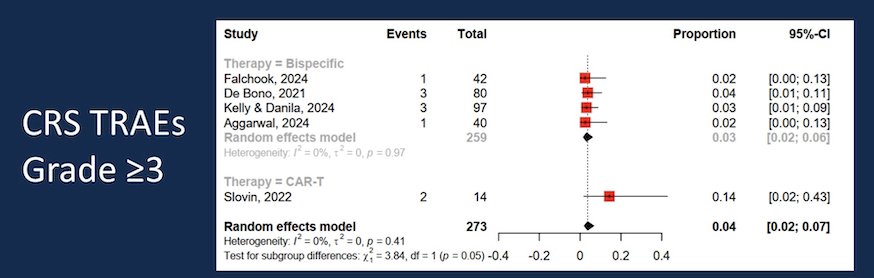
Neurologic TRAEs
Neurologic toxicities were reported in 11% of patients overall but were significantly more frequent in the CAR-T cohort (39%) compared to bsAbs (5%) (p<0.01). This difference suggests that CAR-T therapy carries a higher risk of neurotoxicity, which is consistent with findings from hematologic malignancies where CAR-T-associated immune effector cell-associated neurotoxicity syndrome (ICANS) is a known complication.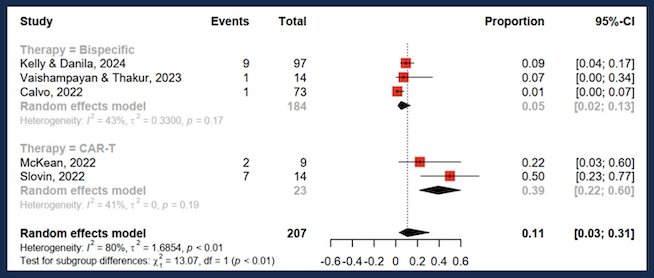
Hematologic and Hepatic TRAEs
Hematologic TRAEs occurred in 38% of patients, with a slightly higher prevalence in the bsAbs group (43%) compared to CAR-T (34%).
Similarly, hepatic TRAEs were observed in 31% of patients, with bsAbs-associated events (39%) occurring more frequently than CAR-T-related hepatic toxicities (25%) (p=0.55). Notably 8% had Grade ≥3 hepatic TRAEs, with 21% on CAR-T versus 5% on BiTEs (p=0.03).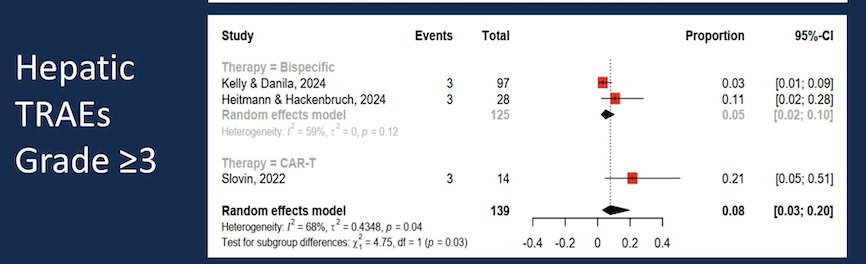
Dr. Saxena concluded with the following key takeaways:
- bsAbs and CAR-T therapies in mCRPC demonstrate similar rates of hematologic, musculoskeletal/dermatologic, renal, and gastrointestinal TRAEs.
- CAR-T therapy is associated with significantly higher rates of all-grade neurologic TRAEs, grade ≥3 CRS, and grade ≥3 hepatic TRAEs compared to bsAbs.
- These findings underscore the importance of recognizing the distinct toxicity profiles of bsAbs and CAR-T therapies. Clinicians should maintain appropriate vigilance, particularly regarding immune-related toxicities, to optimize patient safety and treatment outcomes.
Presented by: Abhiraj Saxena, MD, Internal Medicine Specialist at Robert Wood Johnson University Hospital. New Brunswick, NJ.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.