(UroToday.com) The 2025 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA between February 13th and 15th 2025, was host to the Poster Session A: Prostate Cancer. Dr. Alexander Sherry presented Abstract 140: Metastasis-directed therapy (MDT) plus androgen deprivation therapy (ADT) for oligometastatic prostate cancer (omPC): Primary results of the EXTEND continuous ADT (cADT) basket plus combined analysis with the updated intermittent ADT (iADT) basket and immune correlatives.
The External Beam Radiation to Eliminate Nominal Metastatic Disease (EXTEND) (NCT03599765): trial is a phase 2, basket randomized clinical trial evaluating the addition of metastasis-directed therapy (MDT) to standard-of-care systemic therapy across multiple solid tumors. The trial demonstrated that MDT combined with intermittent ADT (iADT) improved progression-free survival (PFS) and eugonadal PFS compared to iADT alone.1
Dr. Sherry presented the primary results of the EXTEND continuous ADT (cADT) oligometastatic prostate cancer cohort, along with a pre-specified combined analysis incorporating updated data from the iADT cohort. Patients with 1 to 5 oligometastatic sites were randomized 1:1 to MDT + cADT versus cADT alone in the EXTEND study (NCT03599765). MDT consisted of definitive local therapy, while cADT included ADT with or without second-generation anti-androgens. The primary endpoint was per-protocol PFS, defined by biochemical progression (Prostate Cancer Working Group 3), radiologic progression (RECIST v1.1), clinical progression, or death. The study schema is shown below.
A total of 87 patients were required to demonstrate superiority at a one-sided P of 0.10 using a log-rank test and therefore were included in the cADT basket. To assess immune modulation, CDR3 regions of rearranged T cell receptor (TCR) β-chains were sequenced from pre- and post-enrollment peripheral blood using immunoSEQ (Adaptive Biotech). TCR repertoire modulation was defined as the presence of both TCR expansion and contraction, determined using a false-discovery-corrected beta-binomial model. Additionally, TCR sequencing data from the ORIOLE trial (NCT02680587) were analyzed for external validation.
A total of 87 patients were randomized and treated per protocol (MDT + cADT n=45; vs. cADT n=42) between 2018 and 2022. Among them, 39% had oligometastatic castration-resistant prostate cancer. MDT consisted of definitive radiotherapy in all cases.
MDT + ADT vs. ADT alone, was associated with improved radiologic PFS (HR 0.63; 95% CI 0.40–0.97; P = 0.04) and castration-resistance-free survival (HR 0.40; 95% CI 0.19–0.82; P = 0.013).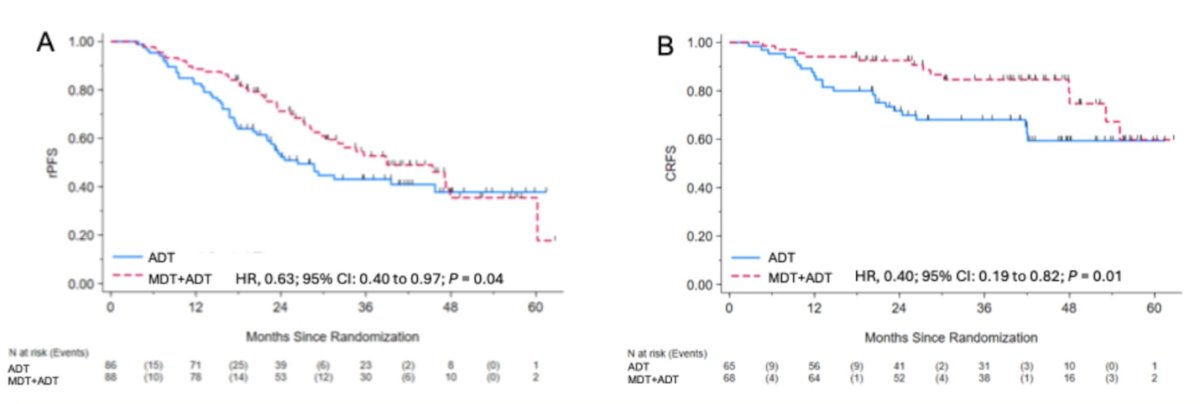
Moreover, MDT + ADT significantly improved PFS (HR 0.45; 95% CI 0.30–0.69; P < 0.001) vs. ADT alone. Similarly, MDT+ ADT improved PFS compared to cADT (HR 0.50; 95% CI 0.23–1.08; P =0.036).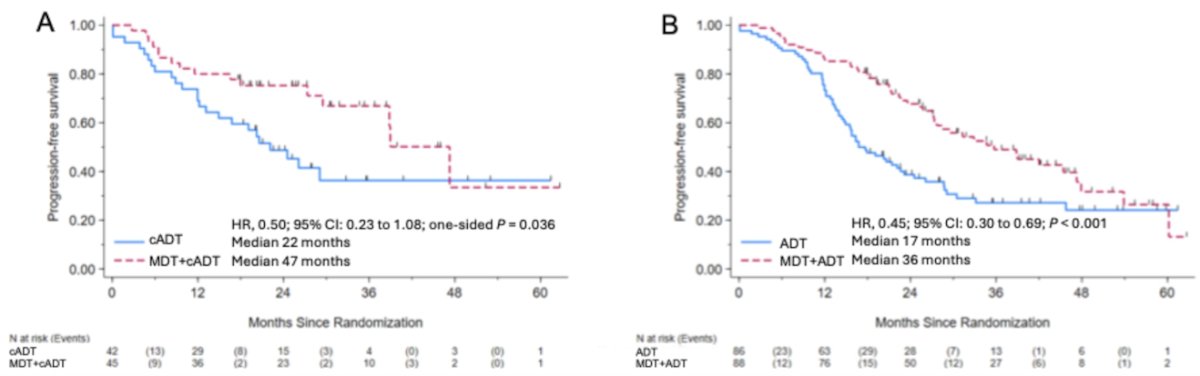
MDT + ADT was associated with significantly higher odds of TCR repertoire modulation compared to ADT alone (55% vs 15%, P < 0.001), a finding validated in the ORIOLE trial population (MDT: 57% vs observation: 19%, P = 0.03).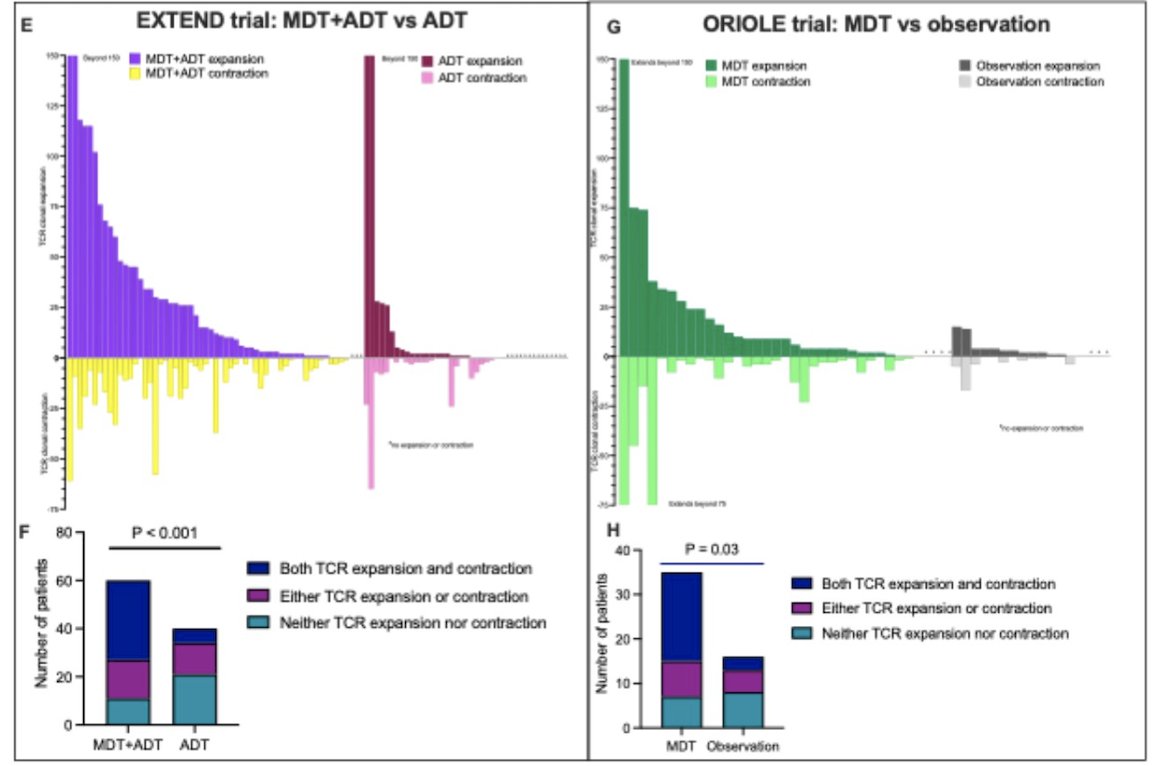
In the analysis of patients with extreme responses, random forest modeling of 37 clinical and immune variables identified TCR repertoire modulation as the most important predictor. Notably, MDT + ADT induced TCR repertoire modulation in all patients with favorable responses (PFS > 4 years) and in none with unfavorable responses (PFS < 1 year).
Among all patients randomized to MDT + ADT, TCR repertoire modulation was significantly associated with longer PFS (HR 0.21; 95% CI 0.06–0.76; P = 0.02) as illustrated below: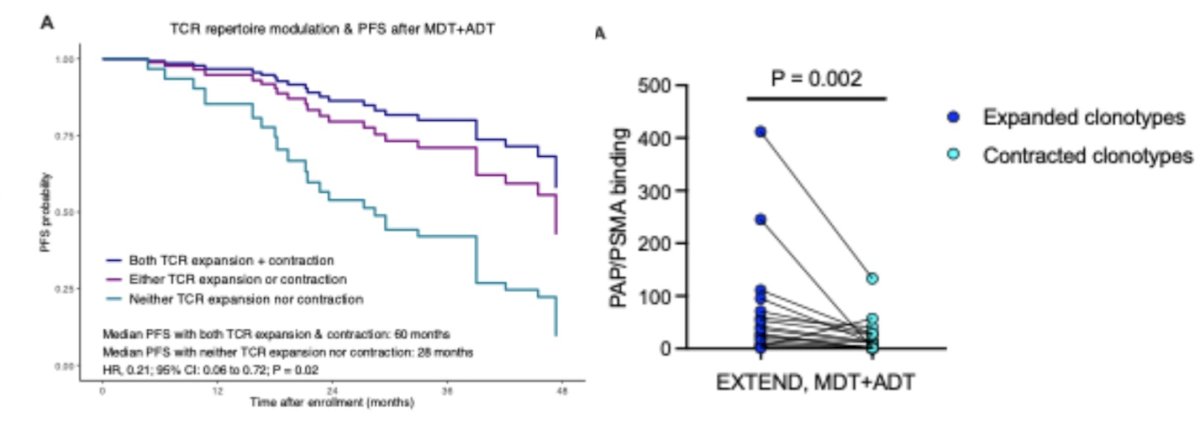
Dr. Sherry concluded their poster presentation with the following key messages:
- MDT + ADT met the primary PFS endpoint of the phase II EXTEND trial, supporting the need for phase III testing.
- MDT + ADT may also improve clinical outcomes, including radiologic PFS and castration-resistance-free survival compared to ADT alone
- These findings validate association between MDT and systemic immune response from the ORIOLE trial
- Improved outcomes may be driven by MDT-induced immunomodulation, and MDT-induced immune responses may be prognostic and could have implications for future trial design.
Presented by: Alexander Sherry, MD, Department of Radiation Oncology at the University of Texas, MD Anderson Cancer Center, Houston, TX. United States.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
Reference: