(UroToday.com) The 2025 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA between February 13th and 15th 2025, was host to the Poster Session A: Prostate Cancer. Dr. Abhishek Tripathi presented Abstract 167: Impact of PSA nadir on long-term survival in metastatic hormone-sensitive prostate cancer: Final 10-year analysis of the ECOG-ACRIN E3805 CHAARTED trial.
The addition of docetaxel to ADT has been shown to improve overall survival (OS) in metastatic hormone-sensitive prostate cancer (mHSPC) and was established as a standard of care for these patients. The ECOG-ACRIN E3805 CHAARTED trial (NCT00309985), randomized men with mHSPC to receive either ADT plus docetaxel (75 mg/m² every 3 weeks for six cycles) or ADT alone, demonstrating a significant OS benefit with the addition of docetaxel. (1) Dr. Tripathi presented a post hoc OS analysis of CHAARTED reporting 10-year OS outcomes and causes of death based on baseline clinical factors and PSA nadir at 6 months in mHSPC patients treated with ADT with or without docetaxel.
The investigators performed an updated survival analysis in July 2024. Patients were categorized based on the timing of metastatic disease (metachronous with prior local therapy vs. synchronous without prior local therapy) and disease burden (low volume [LV] vs. high volume [HV]). Overall survival (OS) was measured from six months post-randomization to death using the Kaplan-Meier method and compared between PSA nadir groups (<0.2 vs. ≥0.2) with the log-rank test.
At a median follow-up of 9.9 years, 225 of the 790 patients from CHAARTED were still alive. In the overall population, 10-year OS was significantly higher in the docetaxel arm compared to ADT alone, with a 22% reduction in the risk of death (HR 0.78; 95% CI 0.66–0.93; P=0.004).
A total of 334 patients in this analysis achieved a PSA nadir of <0.2 at any time, with a median time to nadir of 4.8 months. At the 6-month mark, 204 patients (26.8%) had reached a PSA nadir <0.2., 127 in the ADT+ Docetaxel group and 77 in the ADT alone group.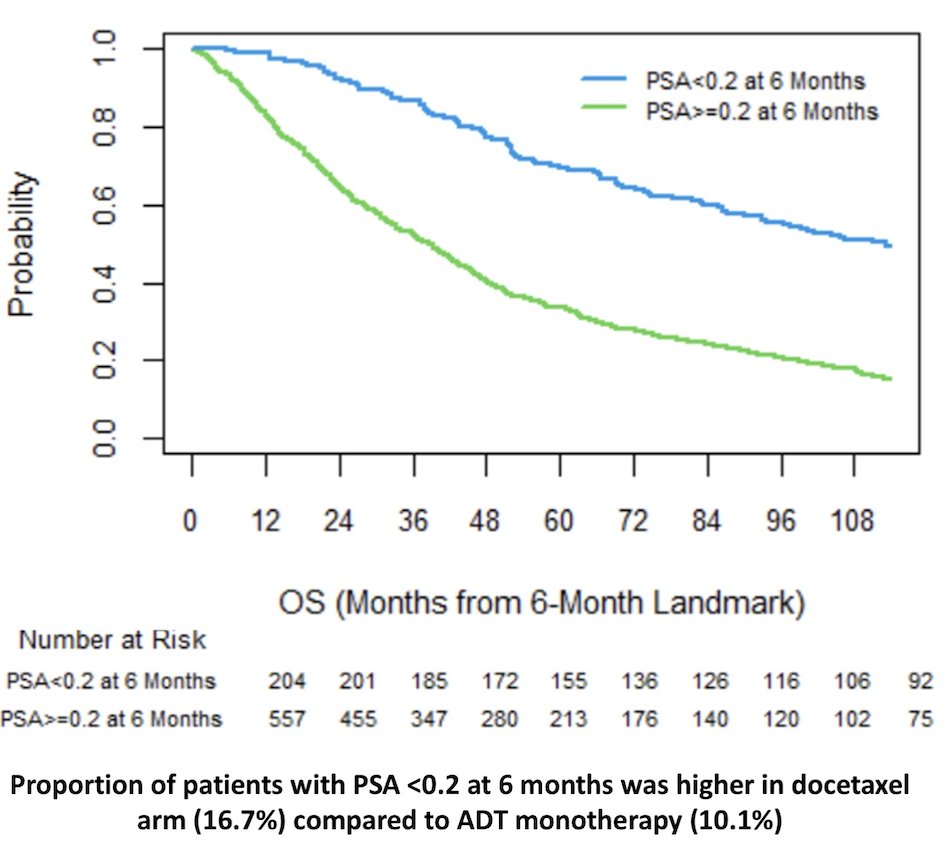
Patients with a PSA nadir <0.2 had significantly longer median OS in both the ADT + docetaxel (100.3 vs. 45.4 months; P < 0.0001) and ADT alone (116.8 vs. 31.8 months; P < 0.0001) arms. This prognostic impact remained significant across all prespecified subgroups as shown below.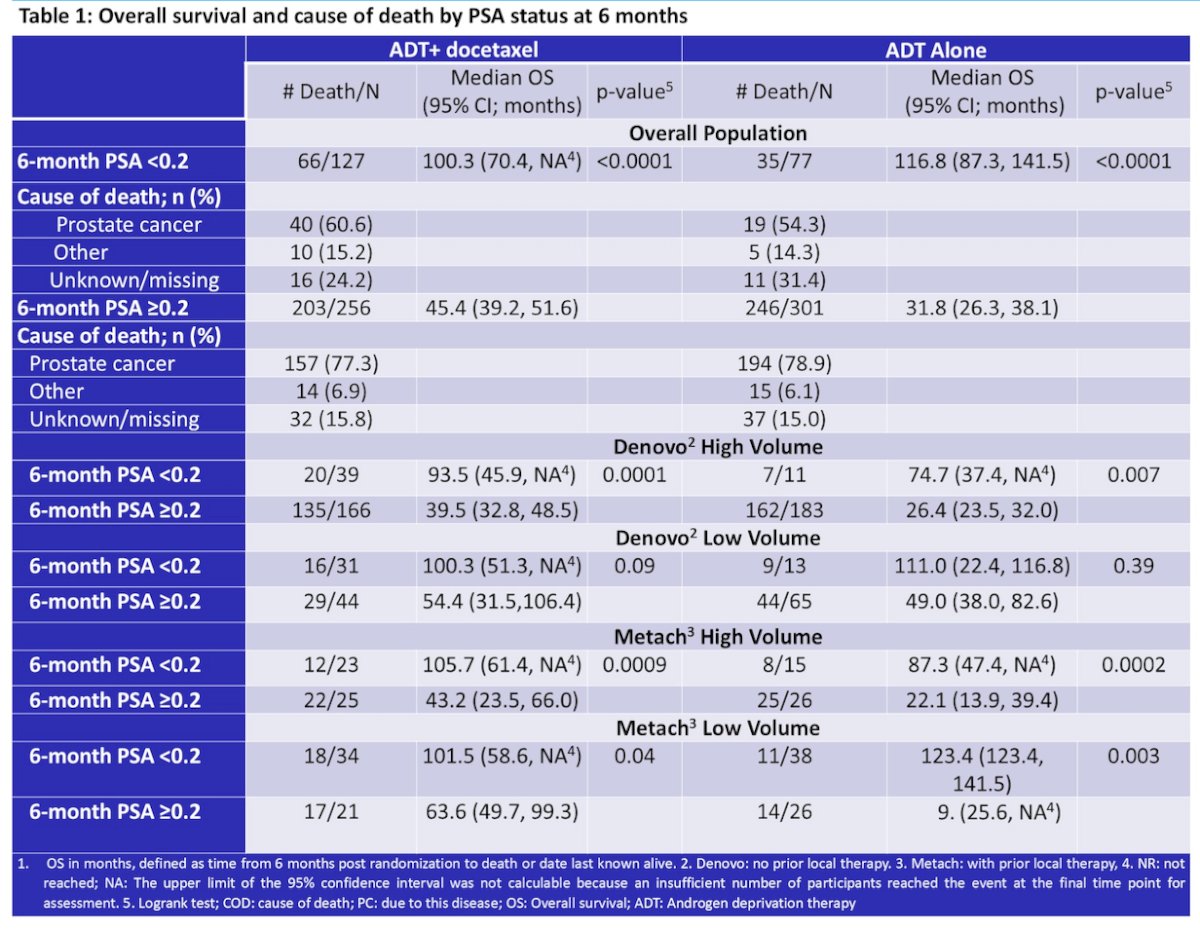
Amongst patients who achieved a PSA <0.2 at 6 months, prostate cancer was the cause of death in 58.4%, ‘other’ causes in 15%, and 27% were unknown. Notably, among the unknown/missing cases, 10 of 27 patients died without a documented progression. In contrast, for those with a PSA nadir ≥0.2, prostate cancer accounted for 78.2% of deaths.
Dr. Tripathi concluded their presentation with the following key takeaways:
- Early docetaxel was associated with higher proportion of patients achieving PSA<0.2 after 6 months of therapy
- Patients in CHAARTED who achieved a PSA nadir <0.2 at 6 months had significantly fewer prostate cancer-specific deaths compared to those with a PSA ≥0.2.
- A PSA nadir <0.2 was associated with significantly longer median OS in both the ADT + docetaxel and ADT alone groups.
- Patients with a PSA nadir <0.2 saw more than a doubling of median OS, with nearly 50% of them still alive at 8 years.
- These findings support the use of PSA nadir as an on-therapy selection criterion for future de-escalation trials.
Presented by: Abhishek Tripathi, MD, Medical Oncologist at The Department of Medical Oncology & Experimental Therapeutics, City of Hope Comprehensive Cancer Center, Duarte, CA, USA
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
References: