(UroToday.com) The 2025 GU ASCO annual meeting featured a prostate cancer session and a presentation by Dr. Xin Gao discussing lead-in phase results of the ARAMON trial assessing darolutamide monotherapy in patients with castration-sensitive prostate cancer (CSPC) after biochemical recurrence. Darolutamide is structurally different by design, with low blood brain barrier penetration and limited potential for drug-drug interactions compared to other androgen receptor inhibitors. It has been hypothesized that the lower blood brain barrier penetration may result in lower reactive elevation in serum testosterone and reduced conversion to estrogen, potentially leading to fewer feminizing adverse events. Treatment of a biochemical recurrence typically starts with ADT, which is limited by treatment emergent adverse events that adversely impact a patient’s quality of life. The second-generation androgen receptor inhibitors, enzalutamide and apalutamide, were explored in patients with biochemical recurrence, demonstrating a reduction in PSA but an increase in testosterone levels from baseline at week 25 of 114% and 134% [1-2]. Given the strong efficacy and favorable tolerability of darolutamide, the open-label, phase 2 ARAMON study (NCT05526248) was conducted to investigate the reactive testosterone increase associated with darolutamide monotherapy in patients with CSPC after biochemical recurrence. At GU ASCO 2025, Dr. Gao and colleagues report results from the lead-in phase of ARAMON.
Eligible patients for ARAMON had confirmed CSPC and a prior radical prostatectomy or radiotherapy, with a rising PSA doubling time ≤20 months, <5 asymptomatic metastatic lesions, serum testosterone >150 ng/dL, and ECOG performance status of 0/1. Patients received darolutamide 600 mg twice daily for 52 weeks. Notably, ADT was not allowed:
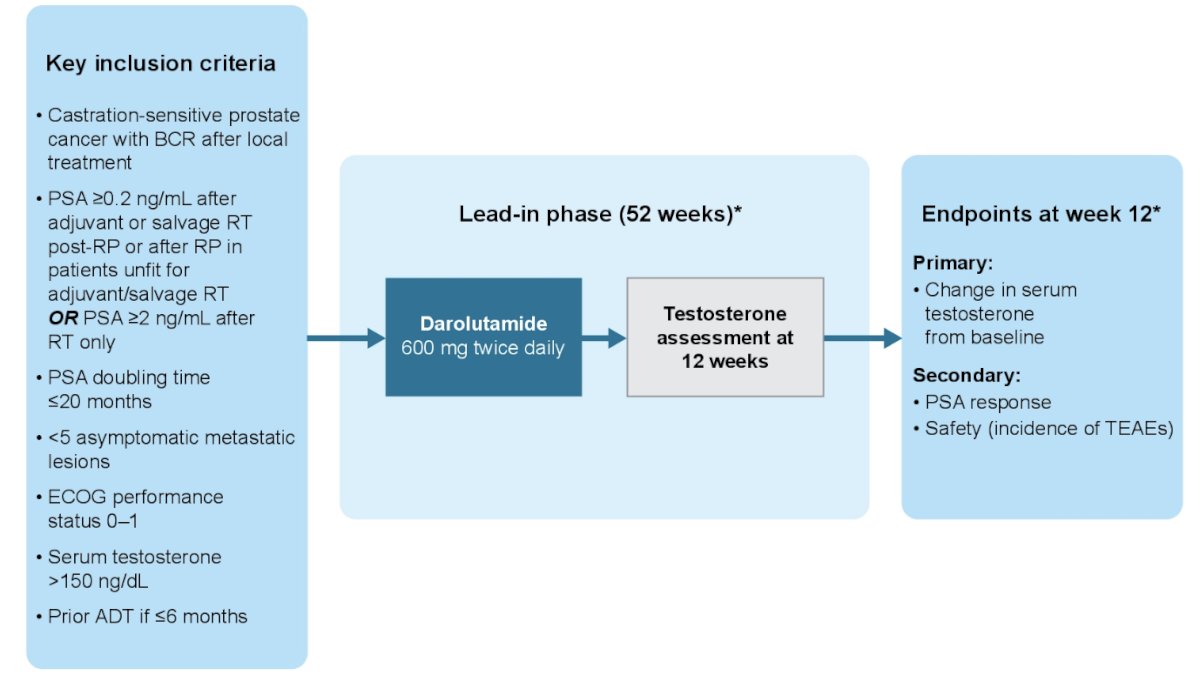
Conventional or PSMA PET imaging was permitted to determine disease stage at baseline. The primary endpoint was the change in testosterone from baseline to week 12 as geometric means. Secondary endpoints were PSA response (PSA50 and PSA90) and treatment emergent adverse events up to January 17, 2024 are also reported.
Of 23 evaluable patients, the median age was 74 (range, 54–84) years, the majority were white (n = 14), had an ECOG performance status of 0 (n = 21), and Gleason score <8 (n = 20). At study entry, the median PSA was 6.0 (range, 2.1–27.4) ng/mL, and most patients had nonmetastatic CSPC (n = 15), 5 patients had oligometastatic disease (bone metastatic lesions <5), and 3 patients had soft tissue metastases (all <2 cm):

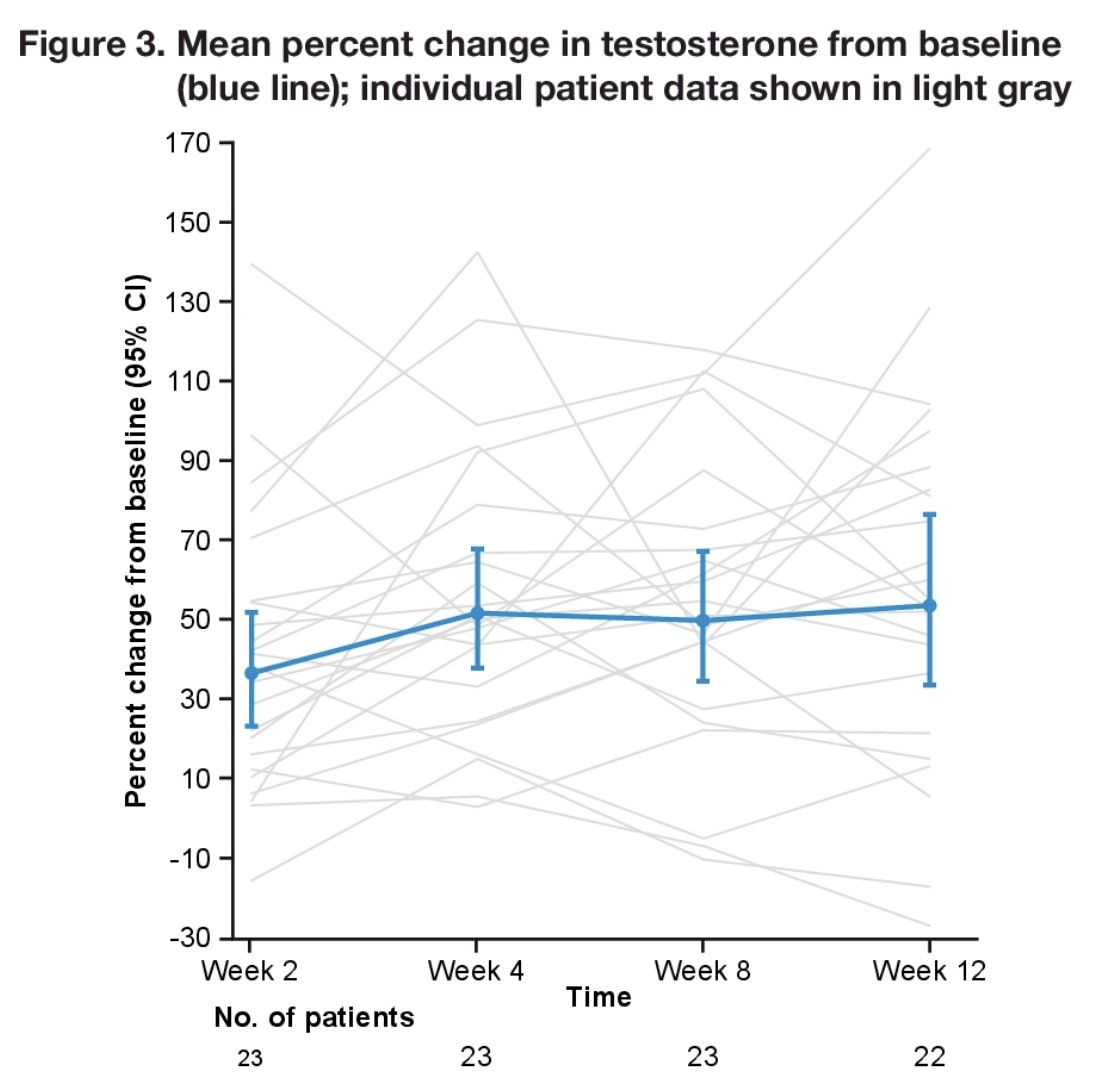
At week 12, the mean percent increase in testosterone from baseline was 53.5% (95% CI, 33.4–76.5):
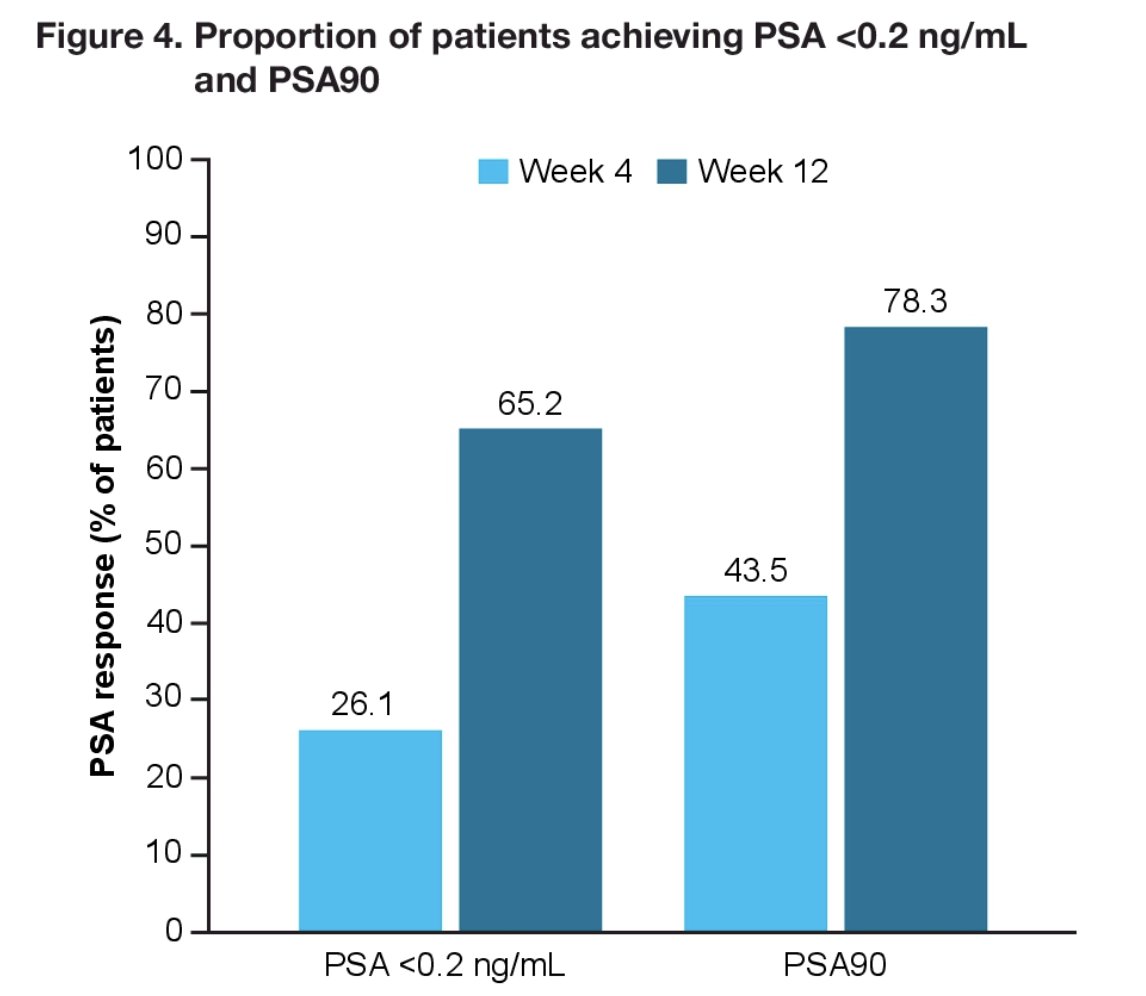
Deep PSA responses to <0.2 ng/mL were observed in 15 patients (65.2%) at week 12. All patients achieved a PSA50 and 78.3% of patients achieved a PSA90:
Treatment emergent adverse events were reported in 22 or 24 patients in the safety analysis set, most were grade 1 or 2, with 3 patients report grade 3 events:

Feminizing treatment emergent adverse events (gynecomastia, breast pain, breast tenderness, nipple pain, breast enlargement, breast mass, breast swelling, and hot flush) occurred in 18 patients and were grade 1 or 2 in 17 patients, 4 patients had dose modifications due to feminizing treatment emergent adverse events, and 2 patients received tamoxifen for gynecomastia. At week 12, none of the patients had discontinued darolutamide due to treatment emergent adverse events. One patient discontinued darolutamide due to gynecomastia after week 12. Fatigue and hypertension occurred in 5 and 4 patients, all of which all events were grade 1/2 in severity.
Dr. Gao concluded his presentation discussing lead-in phase results of the ARAMON trial assessing darolutamide monotherapy in patients with CSPC after biochemical recurrence with the following take-home points:
- In patients with CSPC, darolutamide monotherapy increased baseline testosterone levels to a lesser degree than previously reported for other androgen receptor inhibitor agents administered as monotherapy
- Darolutamide provided deep PSA responses at week 12
- Darolutamide was well tolerated, with a low rate and severity of treatment emergent adverse events, including those commonly associated with androgen receptor pathway inhibitors
- The ARAMON lead-in phase is limited by its single-arm, open-label design, and small sample size
- Upon study completion, data at the 52 week time point will be reported to further evaluate the effect of darolutamide monotherapy in patients with CSPC, although additional studies in larger populations may be needed to understand changes in testosterone levels and related treatment emergent adverse events
Presented by: Xin Gao, MD, Massachusetts General Hospital, Harvard Medical School, Boston, MA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
Related content: Darolutamide Monotherapy in Prostate Cancer: A Phase II Trial Overview - Xin Gao
- Tombal B, Borre M, Rathenborg P, et al. Enzalutamide monotherapy in hormone-naïve prostate cancer: Primary analysis of an open-label, single-arm, phase 2 study. Lancet Oncol. 2014 May;15(6):592-600.
- Maluf FC, Schutz FA, Cronemberger EH, et al. A phase 2 randomized clinical trial of abiraterone plus ADT, apalutamide, or abiraterone, and apalutamide in patients with advanced prostate cancer with non-castrate testosterone levels (LACOG 0415). Eur J Cancer. 2021 Oct 13;158:63-71.