(UroToday.com) The 2025 GU ASCO annual meeting featured a prostate cancer session and a presentation by Dr. Karim Fizazi discussing the final overall survival with talazoparib + enzalutamide as first-line treatment in patients with homologous recombination repair (HRR)-deficient metastatic castration-resistant prostate cancer (mCRPC) in the phase 3 TALAPRO-2 trial. HRR gene alterations are associated with poor survival outcomes in patients with mCRPC. Approximately one-quarter of advanced prostate cancers have alterations in DNA damage response genes directly or indirectly involved with HRR that can sensitize them to treatment with PARP inhibitors. The phase 3 TALAPRO-2 trial met its primary endpoint, showing improved radiographic progression-free survival for talazoparib + enzalutamide versus placebo + enzalutamide as first line treatment in patients with mCRPC in the HRR-deficient cohort (cohort 2).1 At the first interim analysis, immature overall survival data favored talazoparib + enzalutamide versus placebo + enzalutamide. Based on these results, talazoparib + enzalutamide has been approved in the US for adult patients with HRR gene-mutated mCRPC and the European Union for adult patients with mCRPC, with or without HRR genes, for those who cannot receive chemotherapy. At GU ASCO 2025, Dr. Fizazi and colleagues reported the final overall survival data, a descriptive update of radiographic progression-free survival, and extended safety follow-up in cohort 2.
Patients with HRR-deficient tumors were randomized 1:1 to enzalutamide 160 mg + either talazoparib 0.5 mg (0.35 mg if moderate renal impairment) or placebo once daily and stratified by prior abiraterone or docetaxel (yes/no) for castration-sensitive prostate cancer. Key eligibility criteria included asymptomatic or mildly symptomatic mCRPC, ECOG PS ≤1, ongoing androgen deprivation therapy, and no prior life-prolonging therapy for CRPC:
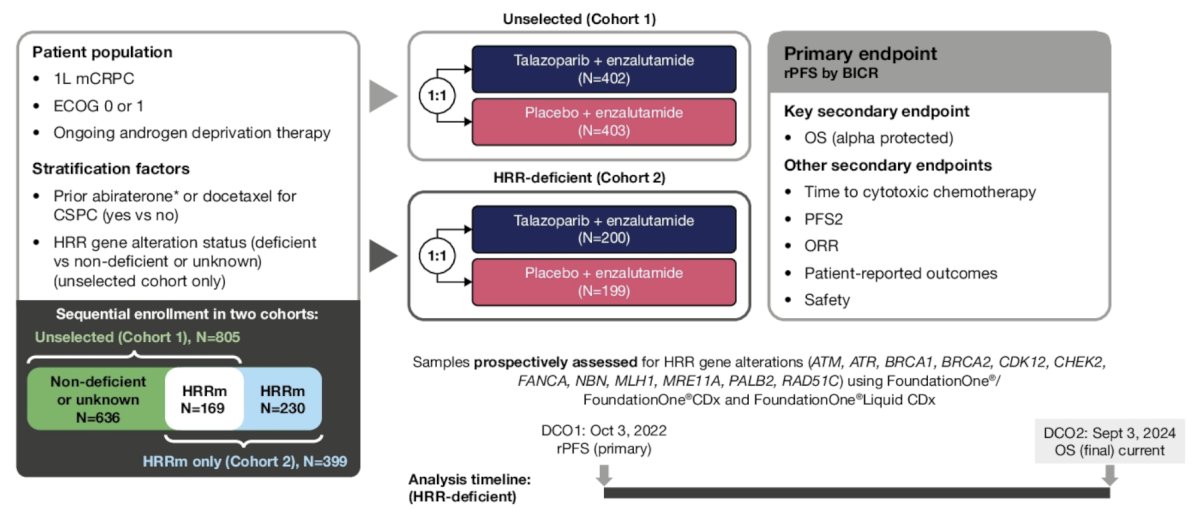
The primary endpoint was radiographic progression-free survival by blinded independent central review. Overall survival was an alpha-protected key secondary endpoint. To achieve statistical significance at the final overall survival analysis, the stratified log-rank 2-sided p value needed to be ≤0.024 using a group sequential design with O’Brien-Fleming spending function.
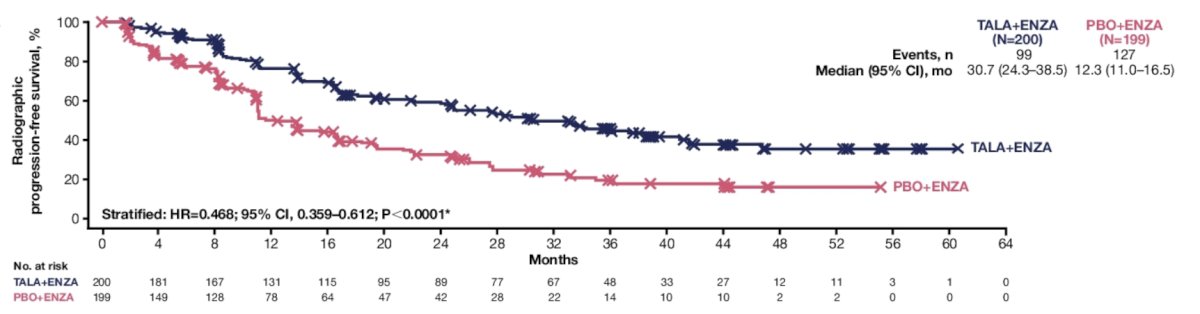
Overall, 399 patients were randomized (n = 200, talazoparib + enzalutamide; n = 199, placebo + enzalutamide). At data cutoff (September 3, 2024), 93 patients (46%) in the talazoparib + enzalutamide arm and 126 patients (63%) in the placebo + enzalutamide arm had died over a median follow-up of 44.2 and 44.4 months, respectively. Updated radiographic progression-free survival data were consistent with the primary analysis, favoring the talazoparib + enzalutamide versus placebo + enzalutamide arm (HR 0.468, 95% CI 0.359–0.612) with a median radiographic progression-free survival of 30.7 versus 12.3 months, respectively:
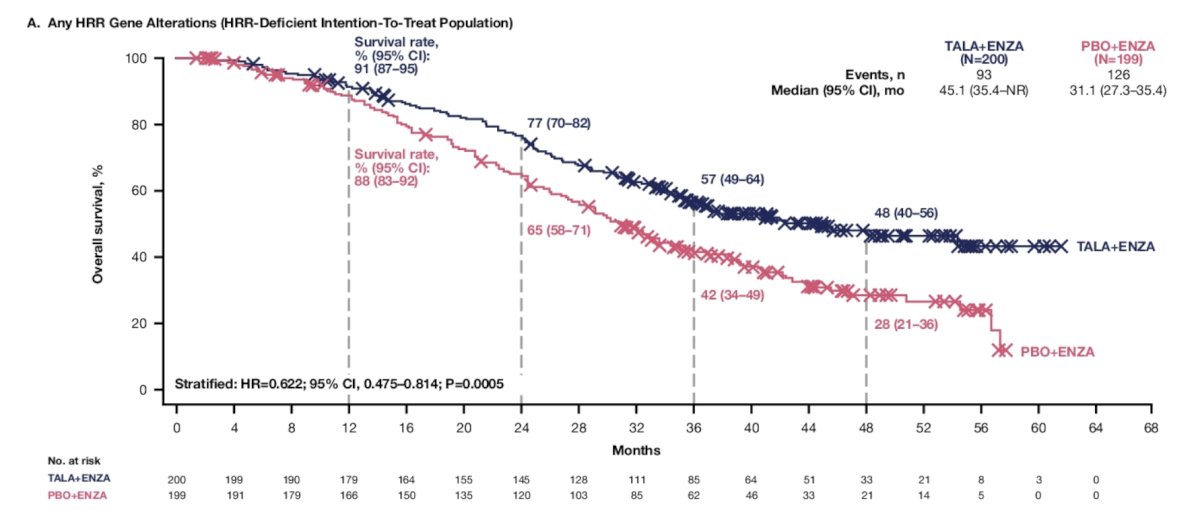
The hazard ratio for overall survival with talazoparib + enzalutamide versus placebo + enzalutamide was 0.622 (95% CI, 0.475–0.814; 2-sided), with a median overall survival of 45.1 months (95% CI 35.4–not reached) versus 31.1 months (95% CI 27.3–35.4 months), respectively:
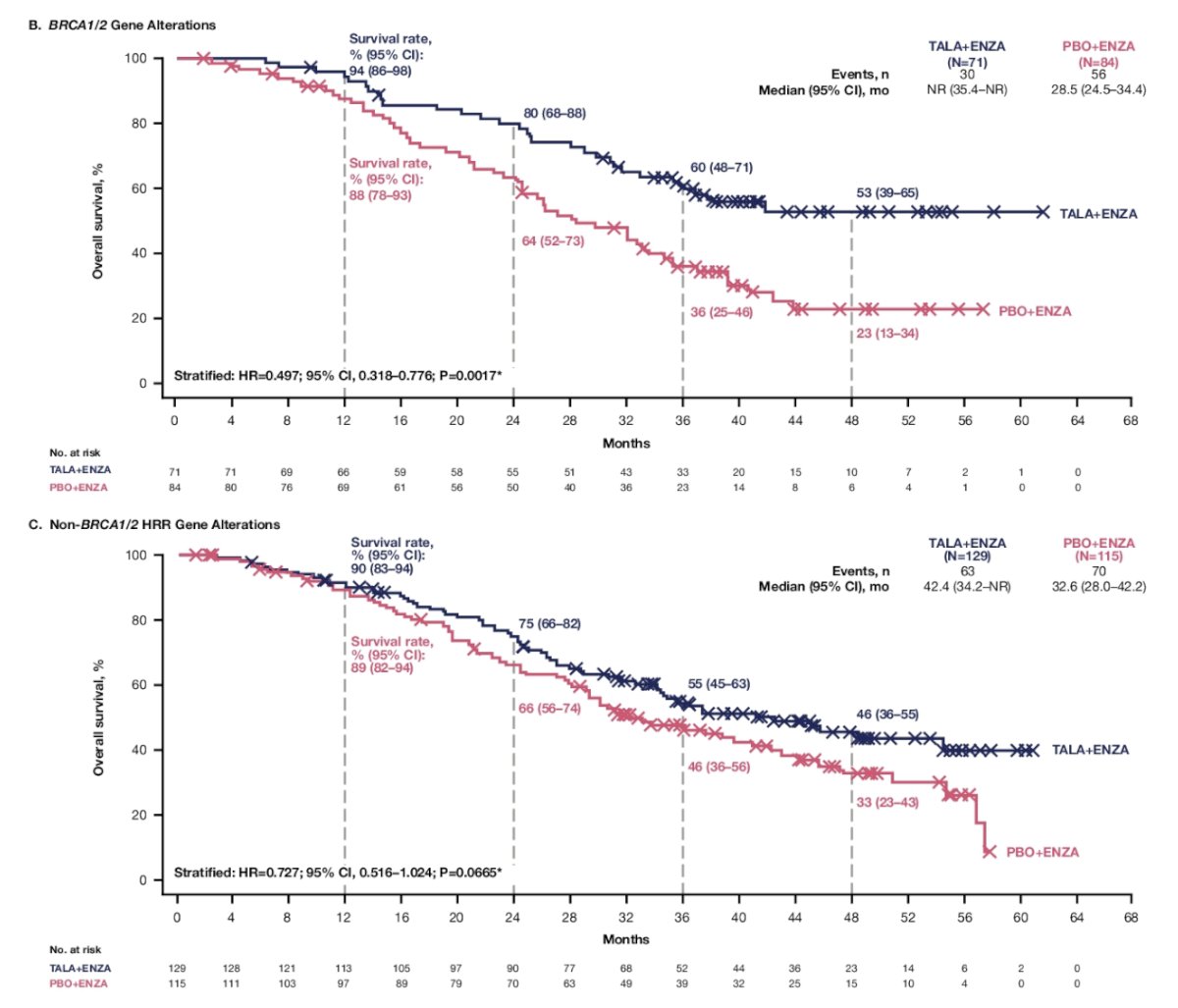
In exploratory analyses, overall survival favored talazoparib + enzalutamide versus placebo + enzalutamide in patients with BRCA1/2 alterations (n = 155; HR 0.497, 95% CI 0.318–0.776) and patients without BRCA1/2 alterations (n = 244; HR 0.727, 95% CI 0.516–1.024):
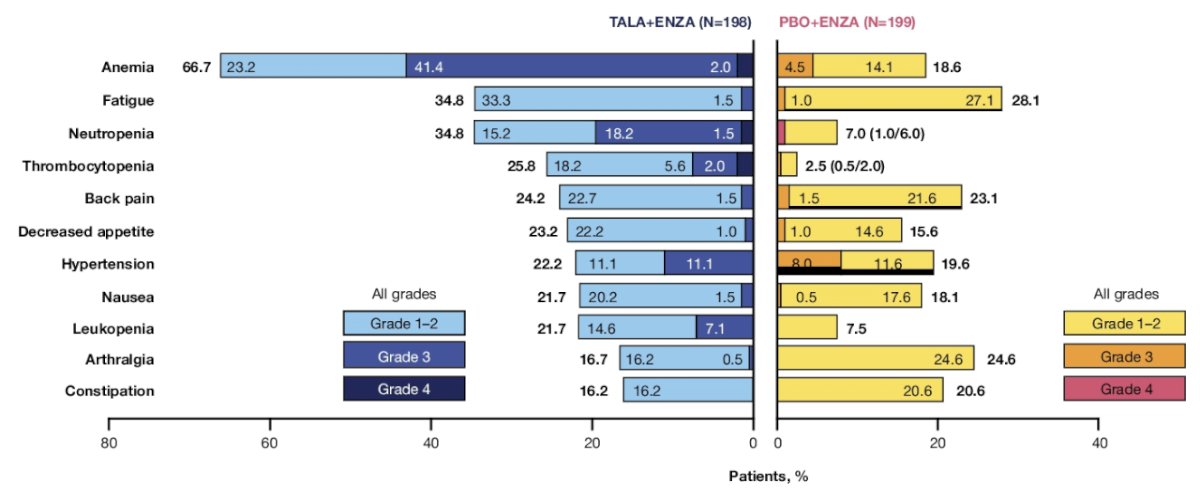
The median duration of treatment of talazoparib was 20.3 months (range: 0.3-61.1). Consistent with primary results, the most common grade 3–4 treatment emergent adverse events with talazoparib + enzalutamide was anemia (43%) and neutropenia (20%). Treatment emergent adverse events were generally manageable, with 26 patients (13%) discontinuing talazoparib due to treatment emergent adverse events:
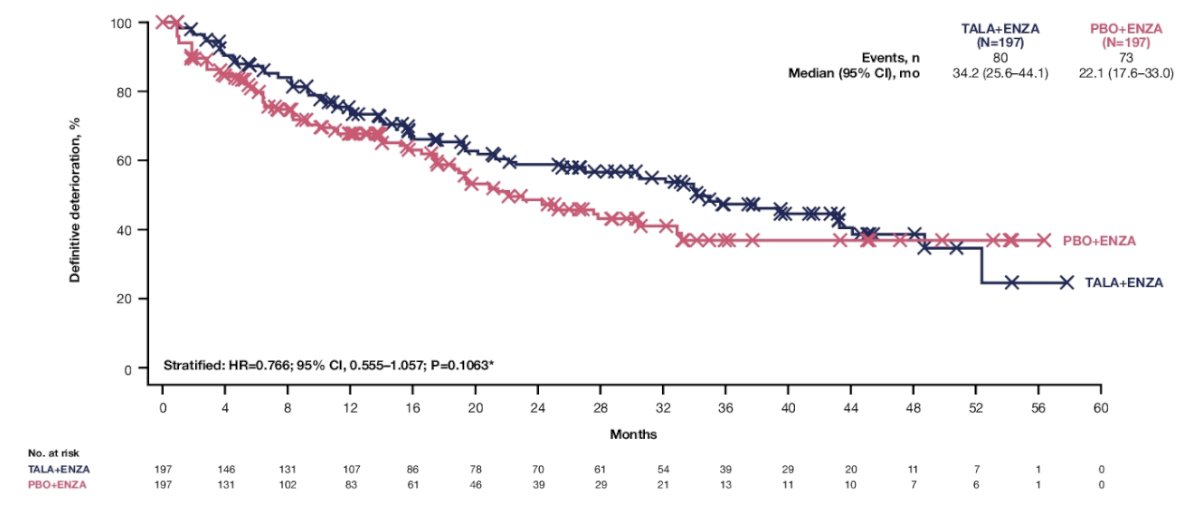
In an updated analyses of patient reported outcomes, the median time to definitive deterioration in patient reported GHS/QoL was 34.2 months (95% CI 25.6-44.1) with talazoparib + enzalutamide versus 22.1 months (95% CI 17.6-33.0) with enzalutamide plus placebo (HR 0.766, 95% CI 0.555-1.057):
Dr. Fizazi concluded his presentation discussing the final overall survival with talazoparib + enzalutamide as first-line treatment in patients with HRR-deficient mCRPC in the phase 3 TALAPRO-2 trial with the following take-home points:
- Talazoparib + enzalutamide demonstrated a statistically significant and clinically meaningful improvement in overall survival versus enzalutamide, which is the longest median overall survival reported in men with HRR-deficient mCRPC and is similar to the median overall survival in the unselected cohort of patients from TALAPRO-2
- These data establish talazoparib + enzalutamide as a standard of care for first line treatment in patients with HRR-deficient mCRPC
- Radiographic progression-free survival continued to favor talazoparib + enzalutamide
- Safety was consistent with previous reports and no new safety signals were identified
Presented by: Karim Fizazi, MD, Institut Gustave Roussy, Villejuif, France
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
References:
- Agarwal N, Azad AA, Carles J, et al. Talazoparib plus enzalutamide in men with first-line metastatic castration-resistant prostate cancer (TALAPRO-2): A randomized, placebo-controlled, phase 3 trial. Lancet. 2023 Jul 22;402(10398):291-303.