(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Genitourinary (GU) Annual Symposium held in San Francisco, CA between February 13–15, 2025 was host to a rapid oral abstract prostate cancer session. Michael Schweizer, MD, presented the results of a randomized dose-expansion study evaluating the combination of mevrometostat (PF-06821497), an EZH2 inhibitor, plus enzalutamide in mCRPC patients.
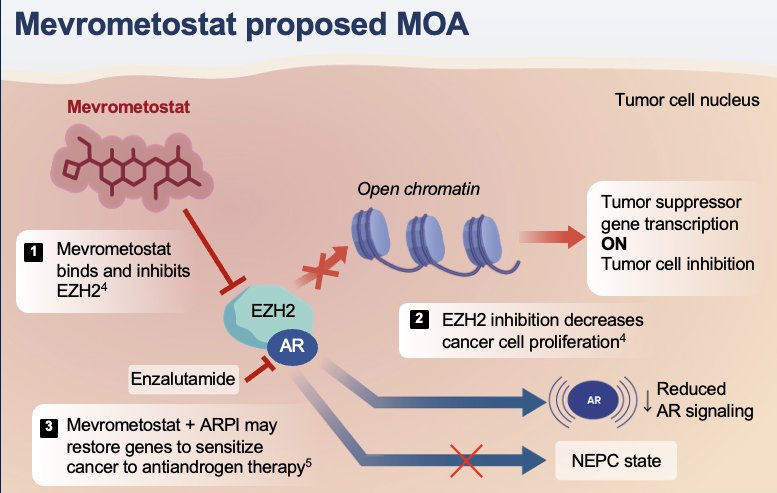
EZH2 is overexpressed in CRPC,1 and is associated with poor prognosis. Mevrometostat is a selective EZH2 inhibitor.2 Dose exploration of mevrometostat + enzalutamide + ADT in mCRPC patients has shown:3
- Manageable safety profile
- On-target pharmacodynamic inhibition of EZH2
- Preliminary evidence of clinical activity
In this presentation, Dr. Schweizer reported the clinical outcomes and impact of administration with food on pharmacokinetics and safety from the open-label, randomized, dose-expansion part of this study (NCT03460977).
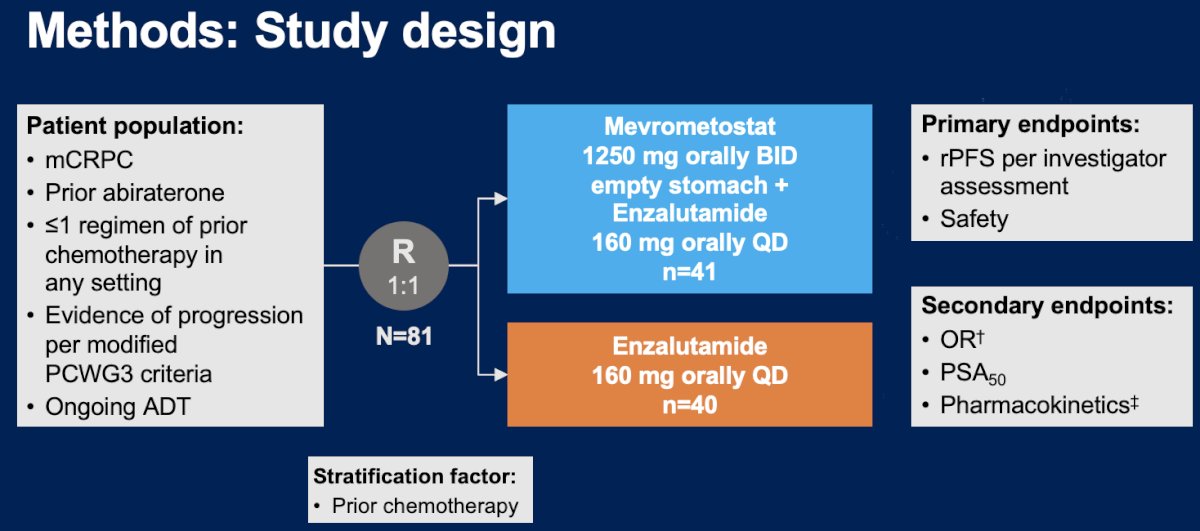
The study design is summarized below. This trial included mCRPC patients who had received prior abiraterone and ≤1 chemotherapy regimen in any setting and had evidence of disease progression per modified PCWG3 criteria. Eligible subjects (n=81) were randomized 1:1 to:
- Mevrometostat 1,250 mg orally twice daily on an empty stomach + enzalutamide 160 mg orally once daily (n=41)
- Enzalutamide 160 mg orally once daily (n=40)
The primary endpoints were:
- rPFS, per investigator assessment
- Safety
Secondary endpoints were:
- Objective response rate
- PSA50 response
- Pharmacokinetics
The baseline characteristics are summarized in the table below. The median patient age was 70–71.5 years. Most patients were White (75%). Approximately 45% of patients had received a prior taxane. Approximately 90% of patients had bone metastases.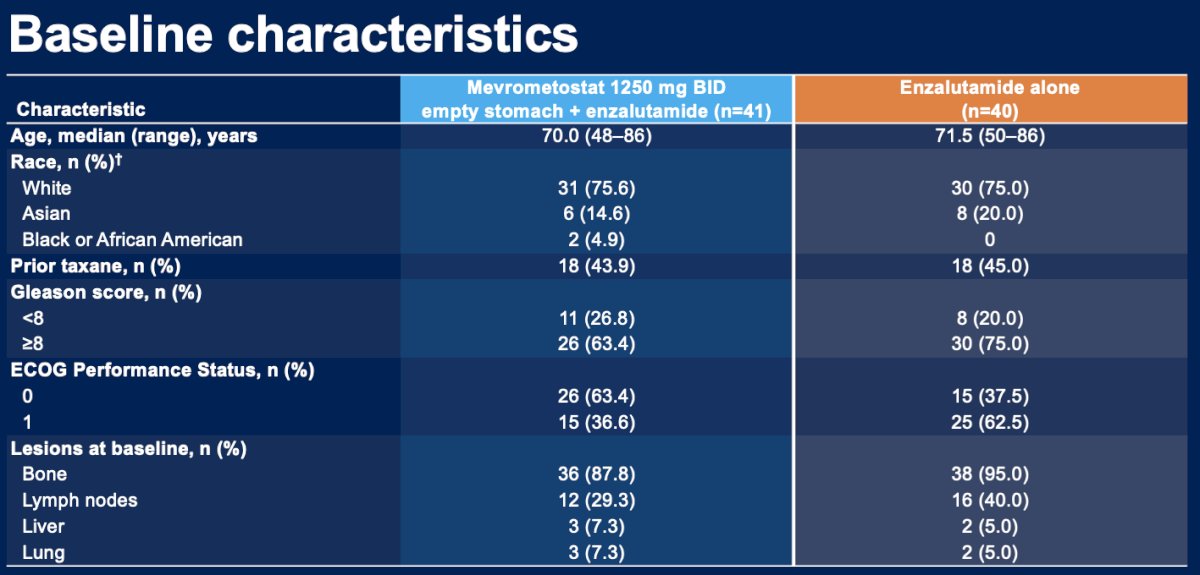
The combination of mevrometostat (1,250 mg BID on an empty stomach) + enzalutamide was associated with a 49% relative reduction in the rate of progression or death, corresponding to an ~8 month improvement in median rPFS (HR: 0.51, 90% CI: 0.28–0.95).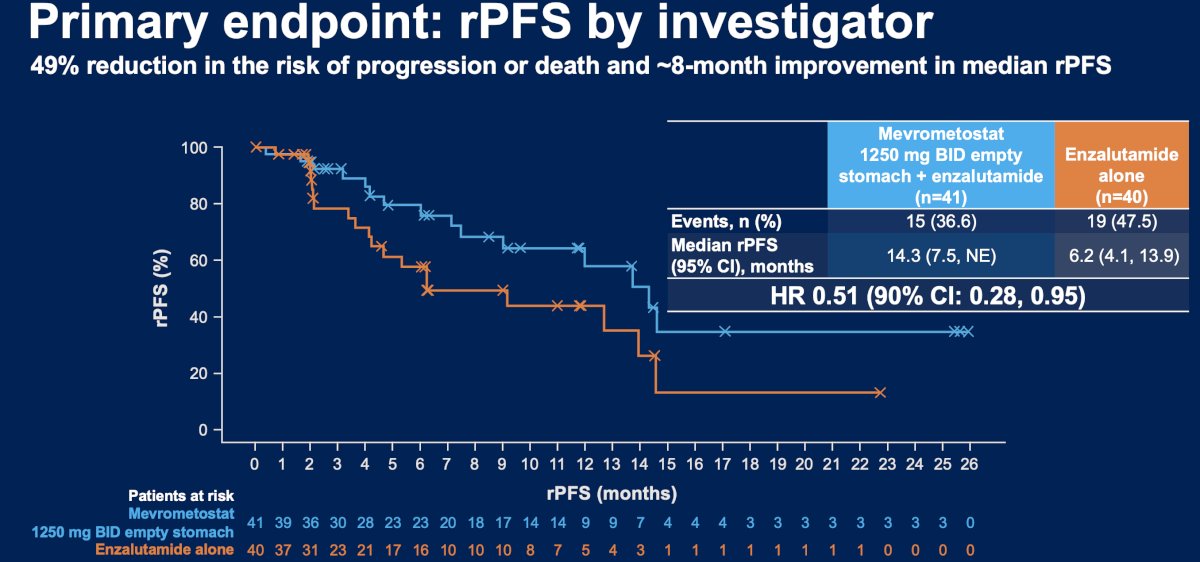
The combination approach was associated with superior objective response rates (27% versus 14%).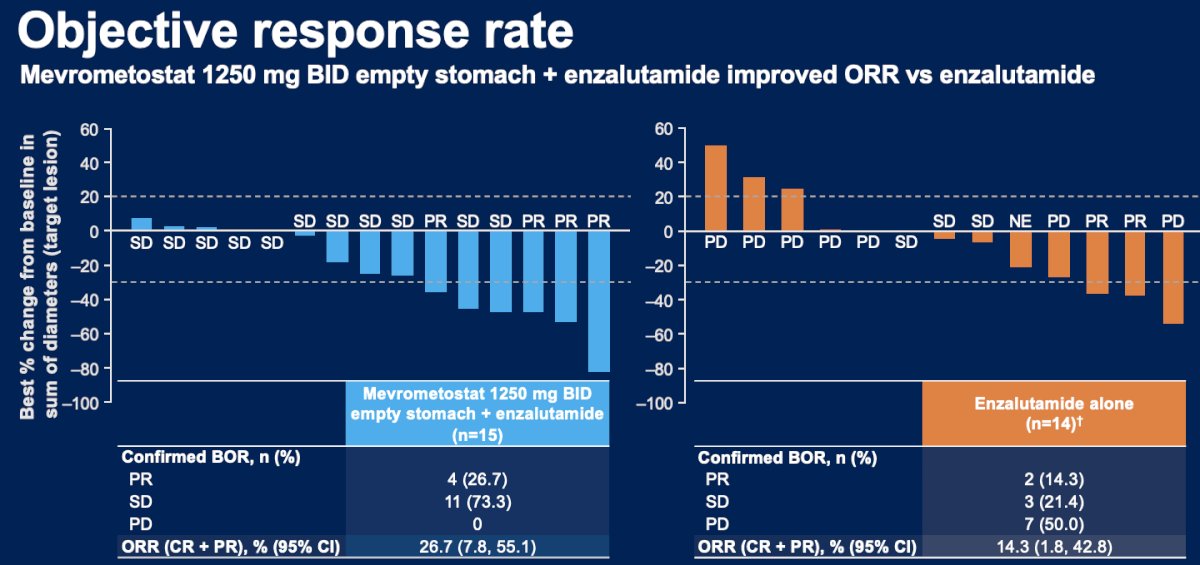
PSA50 response rates were observed in 34% and 15% of patients in the intervention and control arms, respectively.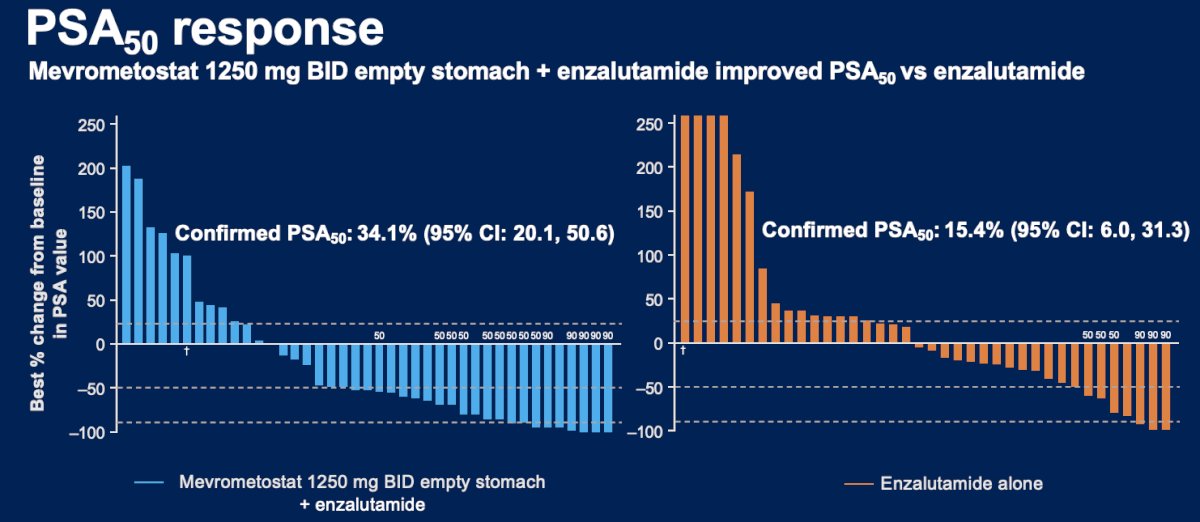
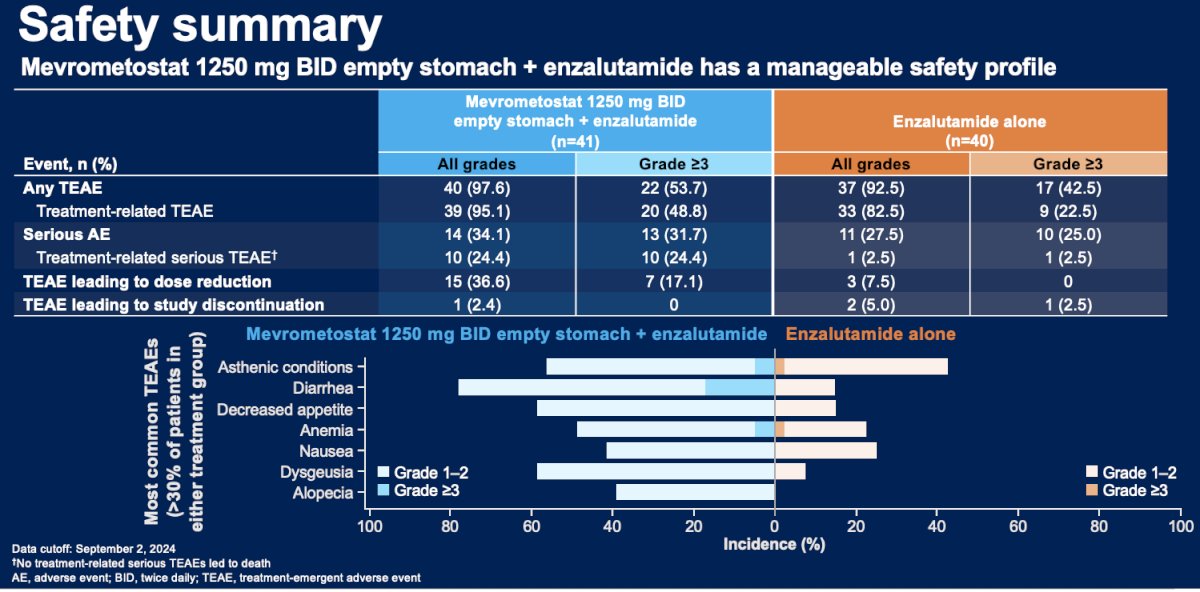
From a safety standpoint, grade ≥3 treatment-emergent adverse events were observed in 54% of patients receiving combination mevrometostat + enzalutamide, versus 43% of enzalutamide monotherapy patients. Serious adverse events were observed in 32% and 25% of patients, respectively. Treatment-emergent adverse events leading to dose reductions were noted in 17% of patients receiving combination therapy. None discontinued the combination therapy due to adverse events. The most common treatment-emergent adverse events with combination therapy were:
- Diarrhea
- Asthenia
- Decrease appetite
- Dysgeusia
- Anemia
- Nausea
- Alopecia
From a pharmacokinetic standpoint, plasma exposure with mevrometostat 875 mg with food was similar to that with mevrometostat 1,250 mg on an empty stomach. Patients treated with mevrometostat 875 mg with food had an improved safety profile, including better GI tolerability, compared with mevrometostat 1250 mg on an empty stomach.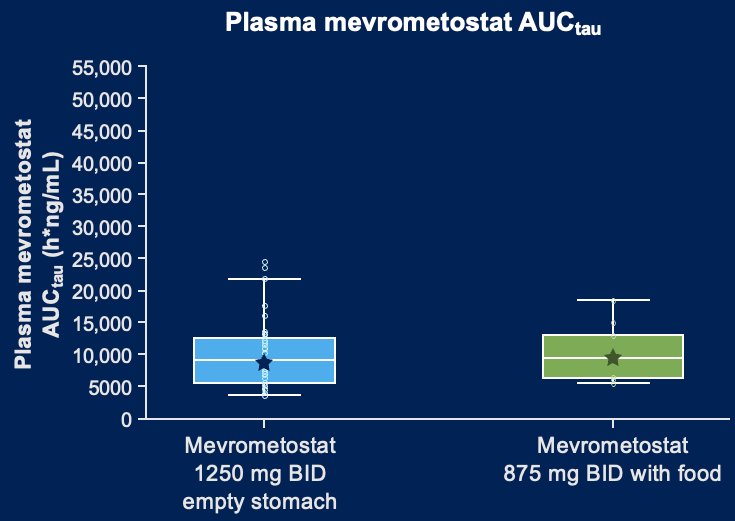
Dr. Schweizer concluded as follows:
- Mevrometostat in combination with enzalutamide showed promising antitumor activity and oncological outcomes, compared with enzalutamide alone in patients with mCRPC (rPFS: HR 0.5, 90% CI: 0.28–0.95)
- Mevrometostat 1,250 mg twice daily on an empty stomach in combination with enzalutamide has a manageable safety profile
- Plasma exposure with mevrometostat 875 mg with food was similar to 1,250 mg empty stomach, with an improved safety profile
- Mevrometostat 875 mg with food is the recommended phase 3 dose
- Pivotal phase 3 studies are in progress in patients with mCRPC previously treated with abiraterone (MEVPRO-1; NCT06551324) or who are ARPI-naïve (MEVPRO-2; NCT06629779)
Presented by: Michael Schweizer, MD, Associate Professor, Medical Oncologist, University of Washington and Fred Hutchinson Cancer Research Center, Seattle, WA
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
References:- Varambally S, Dhanasekaran SM, Zhou M, et al. The polycomb group protein EZH2 is involved in progression of prostate cancer. Nature. 2002; 419(6907):624–9.
- Kung PP, Bingham P, Brooun A, et al. Optimization of Orally Bioavailable Enhancer of Zeste Homolog 2 (EZH2) Inhibitors Using Ligand and Property-Based Design Strategies: Identification of Development Candidate (R)-5,8-Dichloro-7-(methoxy(oxetan-3-yl)methyl)-2-((4-methoxy-6-methyl-2-oxo-1,2-dihydropyridin-3-yl)methyl)-3,4-dihydroisoquinolin-1(2H)-one (PF-06821497). J Med Chem. 2018; 61(3):650-65.
- Schweizer MT, et al. J Clin Oncol. 2024;42(16_suppl):5061