(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Genitourinary (GU) Annual Symposium held in San Francisco, CA was host to a prostate cancer poster session. Dr. Daniel George presented the results of a real-world analysis assessing the use and outcomes of darolutamide (DARO), enzalutamide (ENZA), and apalutamide (APA) for nonmetastatic castration-resistant prostate cancer (nmCRPC), stratified by race subgroup.
The main treatment goals for nmCRPC patients are to prolong survival and delay progression; however, most patients are asymptomatic, so it is essential to consider treatments with a tolerable adverse event profile. Three androgen receptor pathway inhibitors (ARPls) are approved for the treatment of nmCRPC: DARO, ENZA. and APA.1-3
A recent US-based study (DEAR; NCT05362149) using real-world data from a large network of community urologists suggested that patients treated with DARO had a longer treatment duration and delayed progression to metastatic CRPC (mCRPC), compared with those treated with ENZA and APA. DARO was also shown to have a well-tolerated safe profile, compared to ENZA and APA.4
The DEAR-EXT study (NCT06013475) provided evidence based on a further year of patient inclusion and follow-up and included three additional important clinical outcomes: prostate-specific antigen (PSA) response, metastasis-free survival (MFS), and overall survival. The objective of this study was to compare clinical outcomes for nmCRPC patients treated with DARO, ENZA, or APA in separate cohorts of Black and White patients.
DEAR-EXT is a retrospective chart review cohort study in men with nmCRPC from the Precision Point Specialty Analytics network of US urology practices.
The study inclusion criteria are as follow:
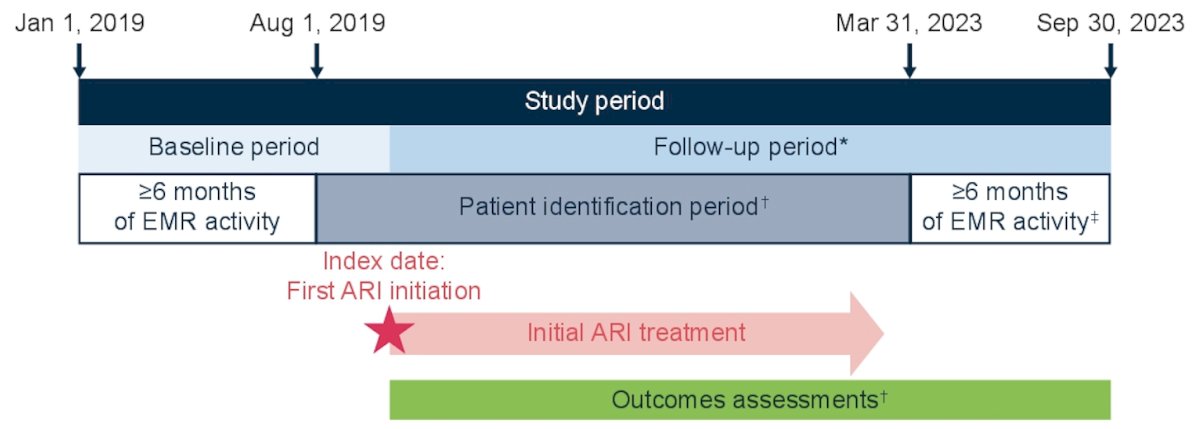
- Men aged ≥18 years who initiated treatment with DARO, ENZA, or APA for the first time for nmCRPC between August 2019 and March 2023 (index date)
- Evidence of nmCRPC before or within 90 days after the index date
- Has ≥6 months of electronic medical records (EMR) activity before and after the index date (unless the patient died earlier)
The exclusion criteria are as follows:
- Evidence of metastatic disease or a treatment prescribed specifically for mCRPC before or up to 30 days after the index date
- History of other primary cancers or participation in other clinical trials
The study outcomes are as follows:
- Time to and reasons for discontinuation of initial ARPI, defined as the earliest occurrence of any of the following: evidence of initial ARPI treatment stop (and no restart of the same treatment within 60 days), switch to another ARPI, or death while receiving treatment
- MFS, defined as time from the index date until progression to mCRPC or death
The statistical analytic plan is as follows:
- Patients were grouped into White and Black cohorts based on their self-reported race
- Time-to-event outcomes were compared using unadjusted Kaplan-Meier estimates and Cox proportional hazards models adjusted for baseline characteristics (age, race, insurance coverage, index year, PSA, time since nmCRPC diagnosis, and Gleason score)
- The analysis was an intention-to-treat analysis, meaning that patient data are analyzed according to their initially assigned index treatment group, regardless of their adherence to the index treatments
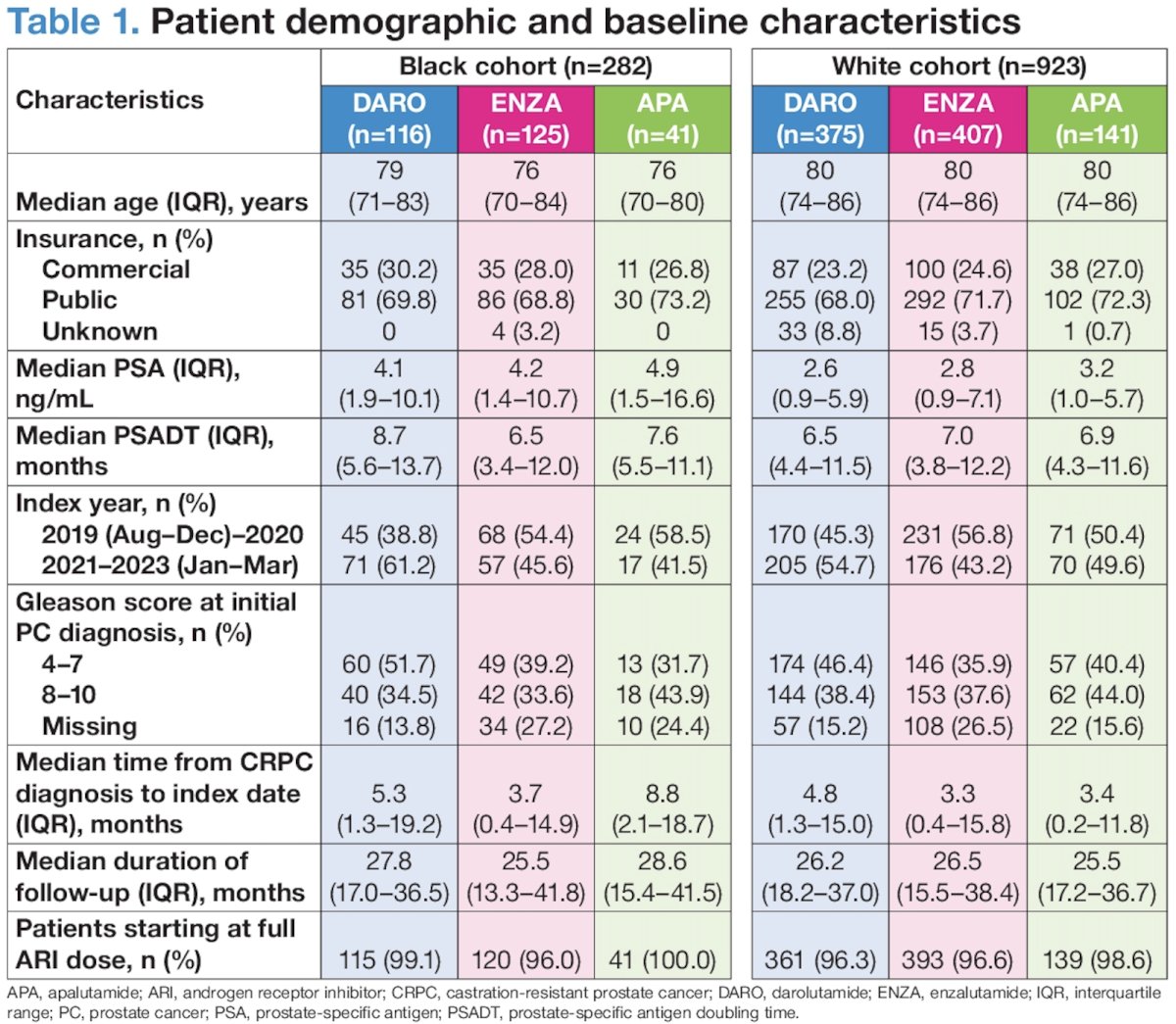
A total of 282 Black and 923 White patients were included, of whom 41% received DARO, 44% received ENZA, and 15% received APA, across both race cohorts. Baseline characteristics were well balanced across the treatment arms within each race cohort, except for the following:
- Compared with the DARO group, the ENZA and APA groups had more patients in earlier index years (2019-2020) in both the Black and White cohorts
- A Gleason score of 4-7 was more common in the DARO group compared with the ENZA and APA groups in both the Black and White cohorts
- Time from CRPC diagnosis to the index date was longer in the APA group in the Black cohort and longer in the DARO group in the White cohort
The duration of follow-up was consistent across treatment subgroups (26–29 months).
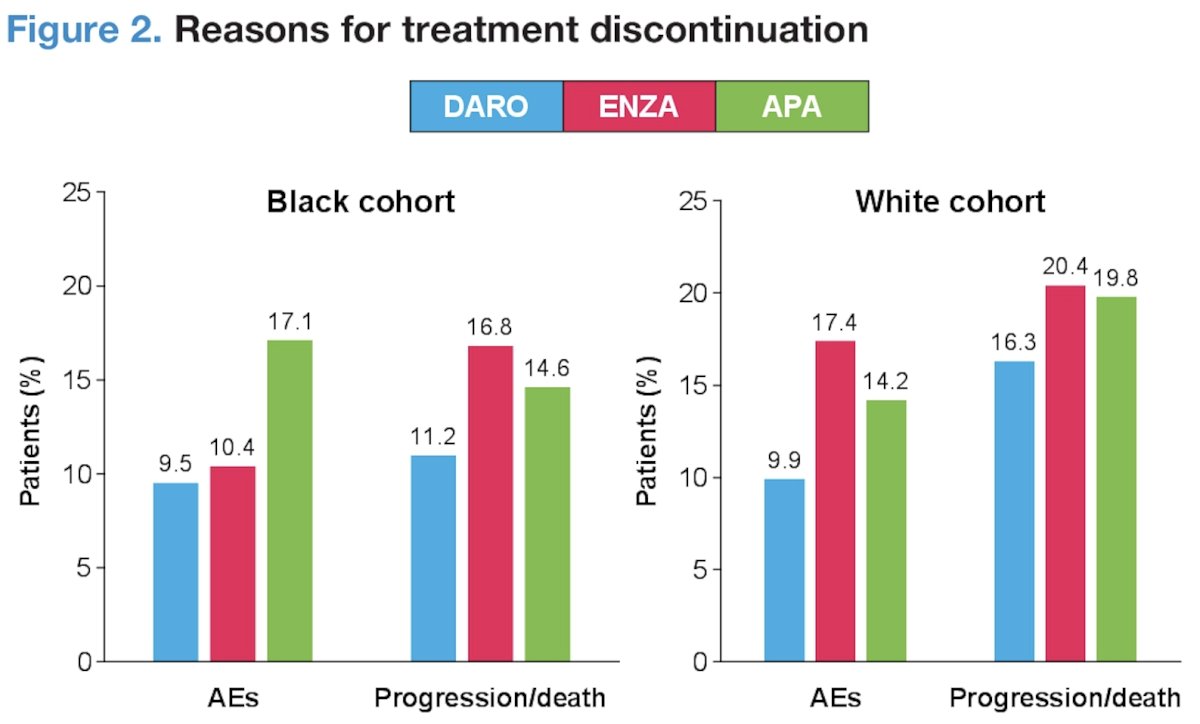
The most frequent reasons for discontinuation were treatment-emergent adverse events and disease progression/death in Black and White patients, both of which occurred less frequently in the DARO group than in the ENZA and APA groups.
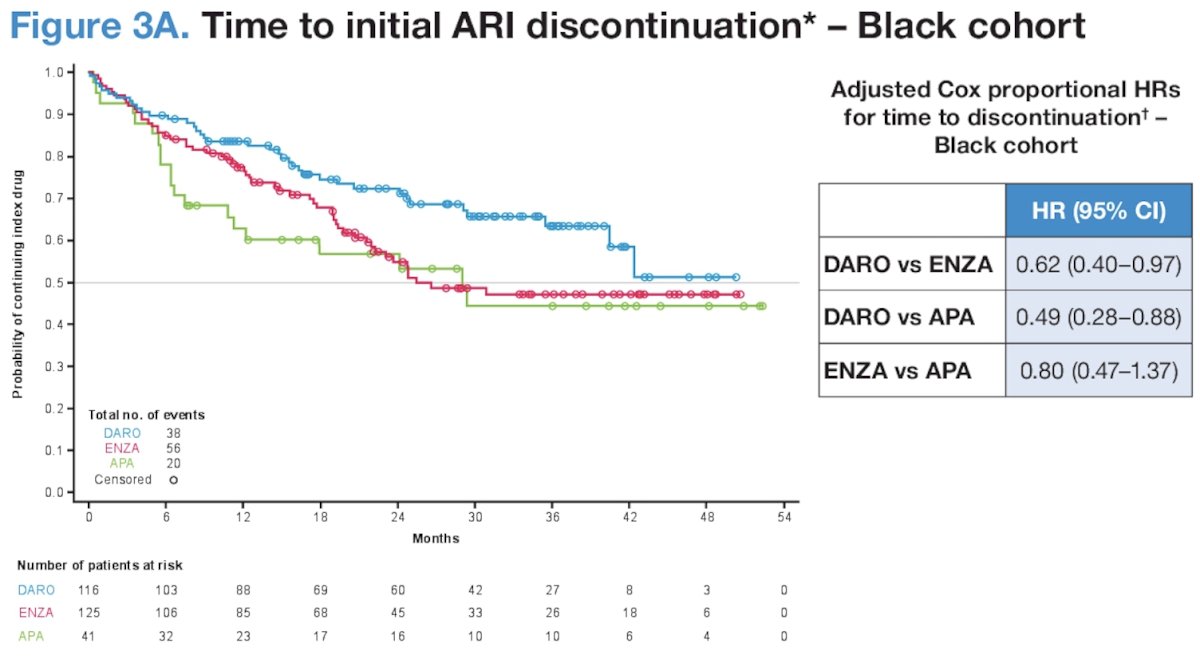
With regards to ARPI discontinuation in the Black cohort, overall, 114 Black patients (40.4%) discontinued their initial ARPI treatment during the study period. The proportion of patients who discontinued their initial ARPI treatment was lower in the DARO group (32.8%) than in the ENZA (44.8%) and APA (48.8%) groups. The median time to ARPI discontinuation was not reached in the DARO group, 25.5 months in the ENZA group, and 29 months in the APA group. Adjusted hazard ratios (HRs) showed that the risk of discontinuation in the DARO group was significantly lower compared with the ENZA and APA groups, whereas the difference between the ENZA and APA groups was not significant:
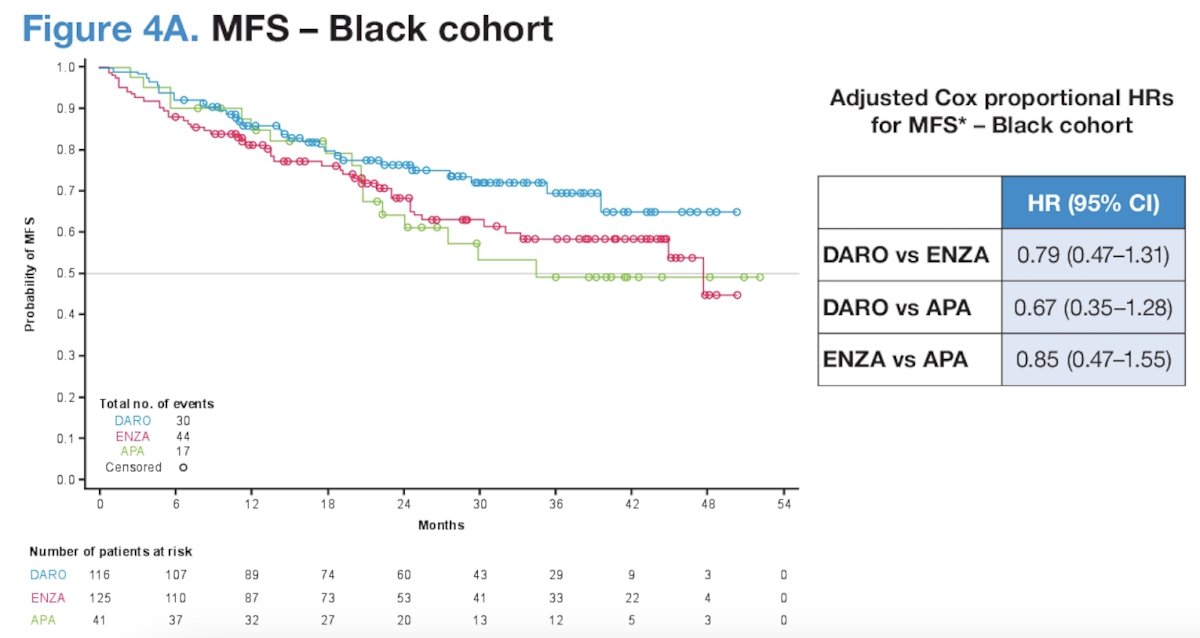
What about MFS in the Black cohort? Overall, 91 Black patients (32.3%) experienced an MFS event during the study period. The proportion was lower in the DARO group (26%) than in the ENZA (35%) and APA (41.5%) groups. The median MFS was not reached in the DARO group, 47.7 months in the ENZA group, and 34.5 months in the APA group. Adjusted HRs showed that the risk of metastasis or death was reduced with DARO by 21% versus ENZA and by 33% versus APA. The risk of metastasis or death was similar in the ENZA group versus the APA group:
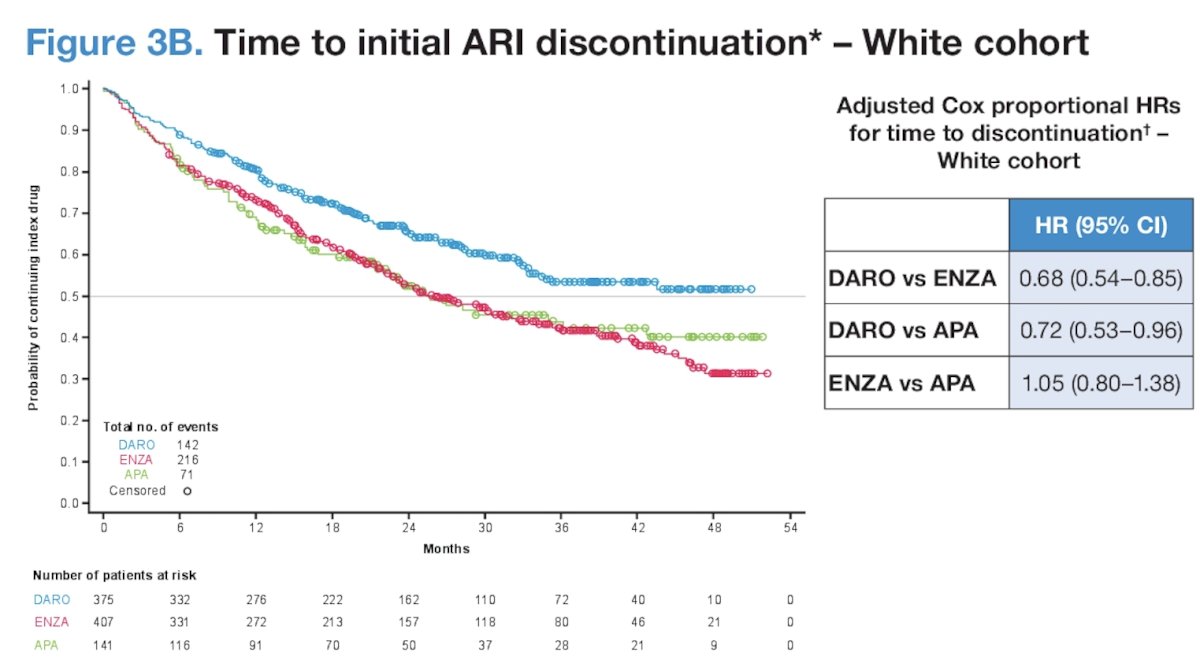
Next, shifting to discuss outcomes in the subgroup of White men, overall, 429 White patients (46.5%) discontinued their initial ARPI treatment during the study period. The proportion of patients who discontinued initial ARPI treatment was lower for the DARO group (38%) than the ENZA (53%) or APA (50.4%) groups. The median time to ARPI discontinuation was not reached for the DARO group, 26.1 months for the ENZA group, and 25.7 months for the APA group. Adjusted HRs show that the risk of discontinuation with DARO was significantly lower compared with ENZA and APA, while the difference between ENZA and APA was not significant:
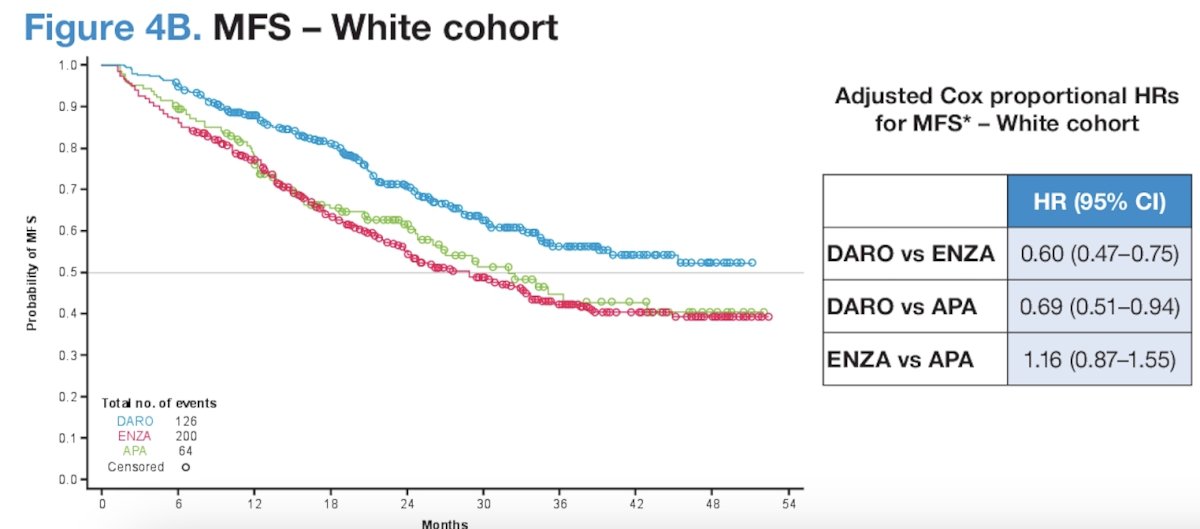
With regards to MFS in White patients, overall, 42.3% experienced an MFS event during the study period. MFS events (metastasis or death) were less frequent for the DARO group (33.6%) than the ENZA (49%) or APA (45.4%) groups. The median MFS was not reached for the DARO group, 29.2 months for the ENZA group, and 32.2 months for the APA group. Adjusted HRs showed that the risk of metastasis or death was reduced with DARO by 40% versus ENZA and by 31% versus APA. The risk of metastasis or death was similar with ENZA versus APA:
Dr. George noted the following strengths and limitations of this analysis:
- While the analysis adjusted for observed differences in baseline characteristics between the three ARPI treatment arms, unobserved confounding factors may also influence treatment duration and clinical outcomes in the absence of randomization
- A key strength of this study is that it is the first large database study to provide evidence regarding clinical outcomes with ARPls in Black and White patient cohorts
He concluded as follows:
- This race subgroup analysis demonstrates potentially greater clinical benefits for DARO versus ENZA and APA among separate cohorts of Black and White patients.
- The probability of discontinuation with DARO was significantly lower in both cohorts compared with ENZA and APA.
- The MFS probability was higher with DARO compared with ENZA and APA
Presented by: Daniel J. George, MD, Professor of Medicine, Department of Medicine, Co-Chair, DCI Center for Prostate & Urologic Cancers; Director of Genitourinary Oncology at Duke Cancer Institute, Durham, NC
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
References:
- Fizazi K, Shore N, Tammela TL, et al. Darolutamide in nonmetastatic castration-resistant prostate cancer. N Engl J Med. 2019;380(13):1235-1246.
- Hussain M, Fizazi K, Saad F, et al. Enzalutamide in men with nonmetastatic, castration-resistant prostate cancer. N Engl J Med. 2018 Jun 28;378(26):2465-2474.
- Smith MR, Saad F, Chowdhury S, et al. Apalutamide treatment and metastasis-free survival in prostate cancer. N Engl J Med 2018;378(15):1408-1418.
- George DJ, Morgans AK, Constantinovici N, et al. Androgen Receptor Inhibitors in Patients With Nonmetastatic Castration-Resistant Prostate Cancer. JAMA Netw Open. 2024; 7(8):e2429783.