(UroToday.com) The 2025 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA was host to the Case-Based Session: Management of Biochemical Recurrence after Radiation Therapy for Localized Prostate Cancer. Dr. Michael Cookson discussed the evaluation, management, and outcomes in patients with recurrence after radiation therapy.
Dr. Cookson opened this case-based panel session by discussing the evaluation of biochemical recurrence after radiotherapy. He highlighted the 2024 AUA/ASTRO/SUO clinical practice guideline on salvage therapy for prostate cancer, which recommends that clinicians obtain a PSMA PET scan instead of conventional imaging or after negative conventional imaging when evaluating suspected non-metastatic recurrence following primary radiation treatment. Additionally, the guideline panel suggests obtaining a pelvic MRI alongside PET/CT for a more comprehensive assessment of local recurrence.1 These recommendations are based on evidence demonstrating the superior accuracy of PSMA PET-CT compared to conventional imaging in men with biochemical recurrence, aiming to improve local staging and guide biopsy before selecting salvage therapy.
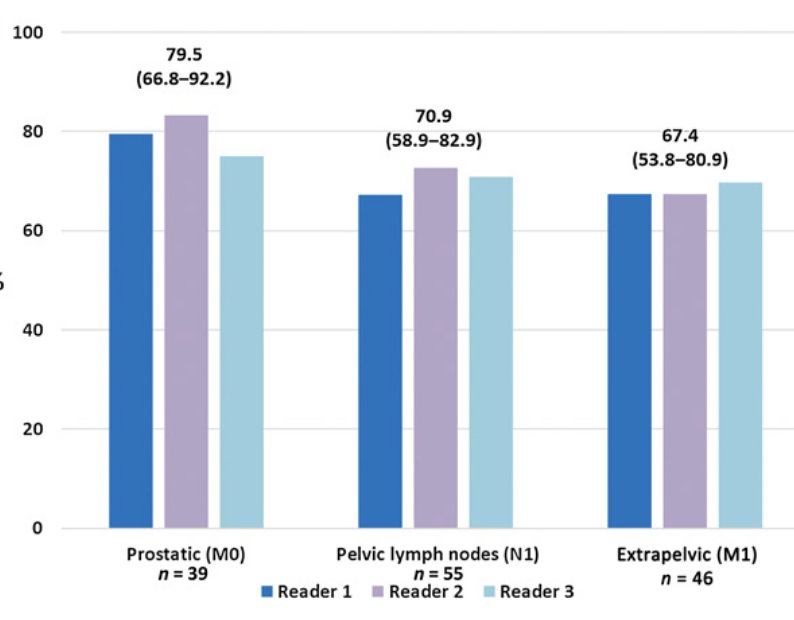
The CONDOR phase III multicenter study evaluated men with biochemical recurrence of prostate cancer who had a PSA >0.2 ng/mL after radical prostatectomy (RP) or >2 ng/mL above nadir after radiotherapy (XRT) and uninformative conventional imaging. The primary endpoint was the correct localization rate of disease recurrence. Among 208 men evaluated (median PSA: 0.8 ng/mL), the disease detection rate ranged from 59% to 66%, while the correct localization rate ranged from 84.8% to 87%, demonstrating the effectiveness of molecular imaging in identifying sites of recurrence.2
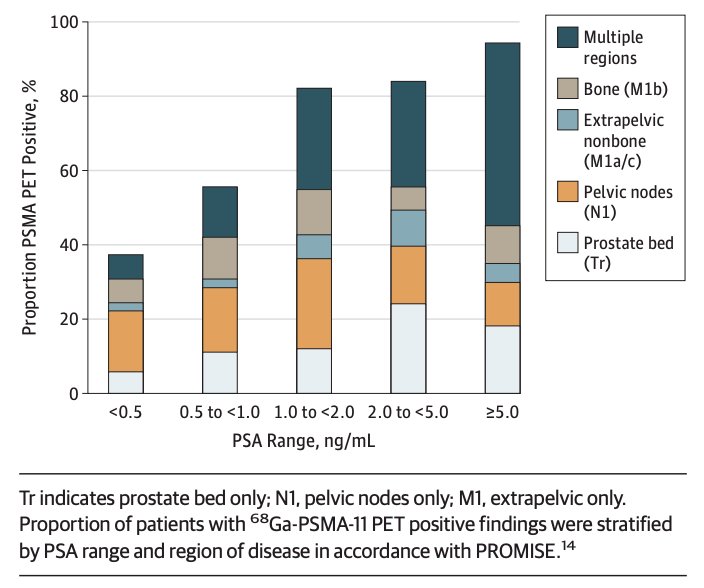
A prospective trial at UCSF evaluated 635 men with biochemical recurrence of prostate cancer after RP, XRT, or both. PSMA PET successfully localized recurrent cancer in 475 of 635 patients (75%).3 The detection rate significantly increased with rising PSA levels as shown in the graphic below:
Moreover, the AUA/ASTRO/SUO guideline on salvage therapy for prostate cancer recommends performing a prostate biopsy to evaluate for local recurrence in men without metastatic disease who are candidates for local salvage therapy. If the biopsy confirms recurrent prostate cancer, these patients may be offered:
- Salvage prostatectomy
- Cryoablation
- High-intensity focused ultrasound (HIFU)
- Re-irradiation
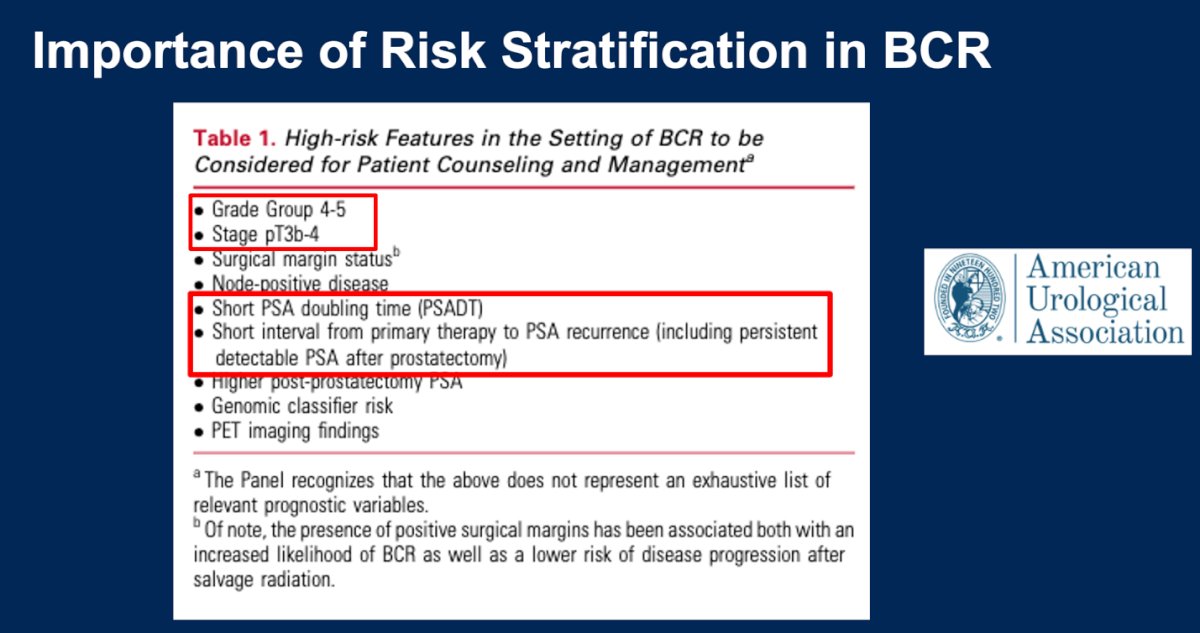
Dr. Cookson highlighted the importance of risk stratification in biochemical recurrence (BCR) and presented the AUA-recommended high-risk features that should be considered for patient counseling and management before selecting a salvage treatment. The most important factors include grade group 4-5, pathologic stage pT3b-4, short PSA doubling times, and short intervals from primary therapy to PSA recurrence.
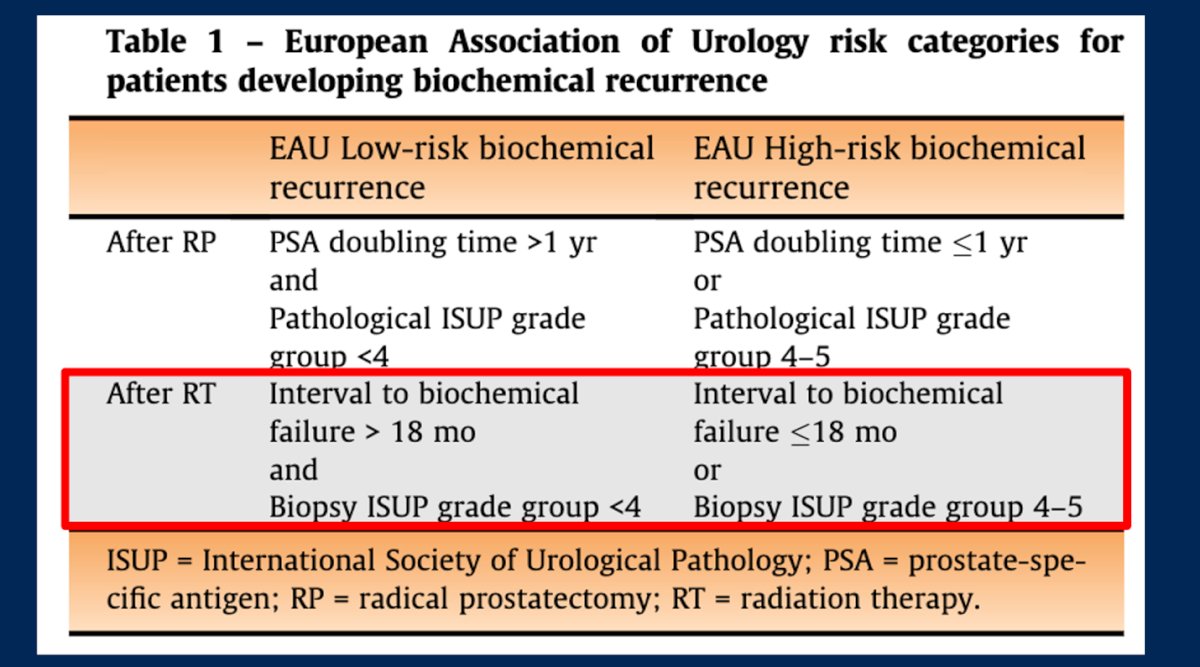
Moreover, the EAU-EANM-ESUR-ISUP-SIOG guidelines on prostate cancer endorse their own EAU risk categories for patients developing biochemical recurrence. After radiation therapy, an interval to biochemical failure greater than 18 months and a biopsy showing ISUP grade group <4 are prognostic factors that help classify patients into low and high-risk biochemical recurrence groups.4
After re-staging patients, ideally with PSMA-PET, and performing a biopsy to confirm the recurrence and stratify them into risk categories, it is time to discuss local salvage treatment. Options include:
Ablative Therapy (Focal or Whole Gland)
- Cryotherapy
- HIFU
- TULSA
- Irreversible Electroporation (IRE)
- +/- ADT
Until recently, biochemical recurrence was one of the last disease states without compelling data supporting the use of androgen deprivation therapy (ADT) in combination with androgen receptor pathway inhibitors (ARPIs). However, two recent trials have demonstrated a benefit of combining ADT with AR targeted therapy:
- EMBARK trial (ADT vs ADT + Enzalutamide vs Enzalutamide alone)
- PRESTO trial (ADT vs ADT with Apalutamide vs ADT/Apalutamide + Abiraterone/Prednisone)
Dr. Cookson moved on to discuss the Patient #1 Case:
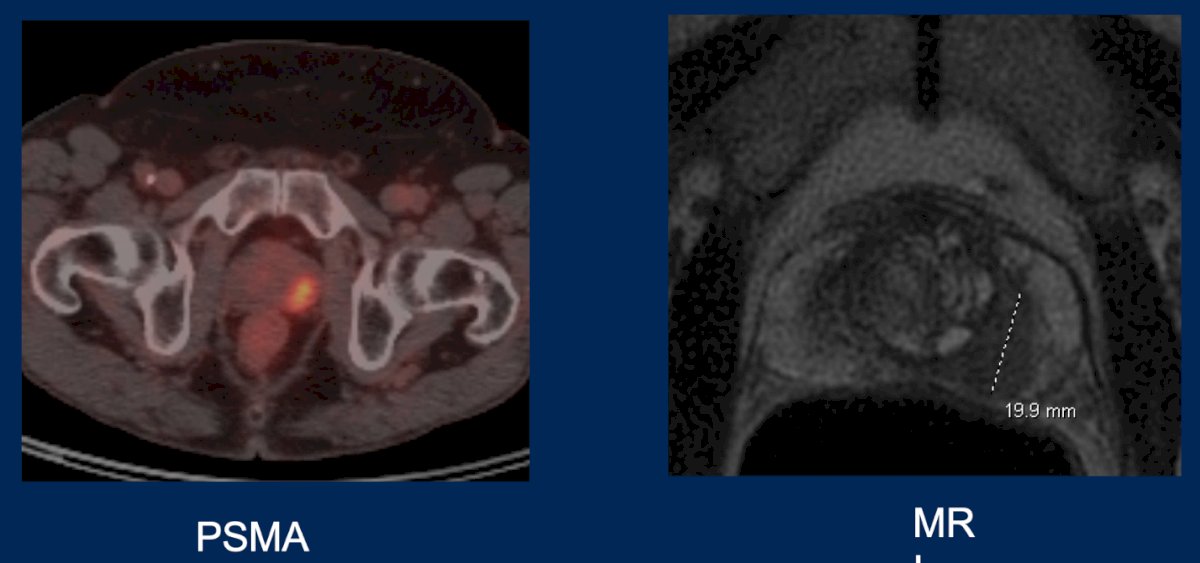
This is a 62-year-old male with a history of GG2 (3/12 cores) cT1cNxM0 prostate cancer treated 5 years ago with IMRT (79.2 Gy:1.8 per fraction, Prostate and Seminal Vesicles). The PSA nadir was 0.5 ng/mL, and he was lost to follow-up until now. His PSA is 5.9 ng/mL. The Prostate MRI revealed a 48cc gland with a suspicious lesion in the Left Peripheral Zone, as shown below.
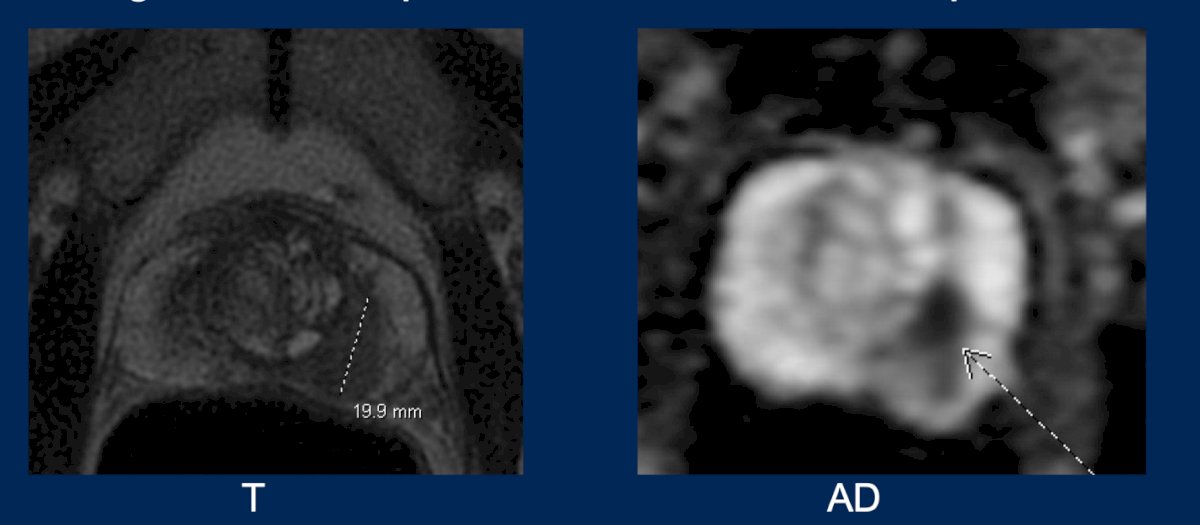
The prostate biopsy revealed a target lesion in the left peripheral zone with Gleason score 3+4, Grade Group 2, along with three additional cores from the left side, also showing Gleason 3+4, Grade Group 2. All other systematic cores, including those from the right side, were negative. The patient reported mild lower urinary tract symptoms, with nocturia occurring once per night, and has normal erectile function.
A PSMA PET scan was performed, showing uptake in the left peripheral zone, consistent with the lesion observed on MRI. There was no evidence of metastatic disease.
To summarize the case, this is a 62-year-old gentleman with a local radio recurrent grade group 2 prostate cancer, PSA 5.9ng/ml, PZ lesion on MRI, no evidence of metastatic disease and who desires salvage treatment. Treatment options for him include:
- Radical Prostatectomy
- Focal Ablative Therapy
- Repeat Radiation Therapy
The salvage treatment options were discussed by Drs. Ashley Ross, Thomas Polascik, and Juanita Crook, respectively.
Presented by: Michael Cookson, MD, MMHC, FACS, University of Oklahoma College of Medicine, Oklahoma, United States.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
References:- Morgan TM, Boorjian SA, Buyyounouski MK, et al. Salvage therapy for prostate cancer: AUA/ASTRO/SUO guideline part I: introduction and treatment decision-making at the time of suspected biochemical recurrence after radical prostatectomy. J Urol. 2024;211(4):509-517. https://www.auajournals.org/doi/10.1097/JU.0000000000003892
- Morris MJ, Rowe SP, Gorin MA, Saperstein L, Pouliot F, Josephson D, Wong JYC, Pantel AR, Cho SY, Gage KL, Piert M, Iagaru A, Pollard JH, Wong V, Jensen J, Lin T, Stambler N, Carroll PR, Siegel BA; CONDOR Study Group. Diagnostic Performance of 18F-DCFPyL-PET/CT in Men with Biochemically Recurrent Prostate Cancer: Results from the CONDOR Phase III, Multicenter Study. Clin Cancer Res. 2021 Jul 1;27(13):3674-3682. doi: 10.1158/1078-0432.CCR-20-4573. Epub 2021 Feb 23. PMID: 33622706; PMCID: PMC8382991.
- Hope TA, Eiber M, Armstrong WR, Juarez R, Murthy V, Lawhn-Heath C, Behr SC, Zhang L, Barbato F, Ceci F, Farolfi A, Schwarzenböck SM, Unterrainer M, Zacho HD, Nguyen HG, Cooperberg MR, Carroll PR, Reiter RE, Holden S, Herrmann K, Zhu S, Fendler WP, Czernin J, Calais J. Diagnostic Accuracy of 68Ga-PSMA-11 PET for Pelvic Nodal Metastasis Detection Prior to Radical Prostatectomy and Pelvic Lymph Node Dissection: A Multicenter Prospective Phase 3 Imaging Trial. JAMA Oncol. 2021 Nov 1;7(11):1635-1642. doi: 10.1001/jamaoncol.2021.3771. PMID: 34529005; PMCID: PMC8446902.
- Tilki D, van den Bergh RCN, Briers E, Van den Broeck T, Brunckhorst O, Darraugh J, Eberli D, De Meerleer G, De Santis M, Farolfi A, Gandaglia G, Gillessen S, Grivas N, Henry AM, Lardas M, J L H van Leenders G, Liew M, Linares Espinos E, Oldenburg J, van Oort IM, Oprea-Lager DE, Ploussard G, Roberts MJ, Rouvière O, Schoots IG, Schouten N, Smith EJ, Stranne J, Wiegel T, Willemse PM, Cornford P. EAU-EANM-ESTRO-ESUR-ISUP-SIOG Guidelines on Prostate Cancer. Part II-2024 Update: Treatment of Relapsing and Metastatic Prostate Cancer. Eur Urol. 2024 Aug;86(2):164-182. doi: 10.1016/j.eururo.2024.04.010. Epub 2024 Apr 29. PMID: 38688773.