(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Genitourinary (GU) Annual Symposium held in San Francisco, CA between February 13–15, 2025 was host to prostate cancer poster session. Dr. Martin Gleave presented the results of sub-protocol 1 of the Genomic Umbrella Neoadjuvant Study (GUNS) trial assessing genomic alterations and their pathologic responses in high-risk, localized prostate cancer.
GUNS (NCT04812366) is a multicenter, adaptive phase II umbrella trial evaluating androgen receptor pathway inhibitor (ARPI) combination therapies in high-risk, localized prostate cancer to define the effects of biomarker-selected targeted therapies on depth of pathologic response (complete response [pCR] or < 5 mm minimal residual disease [MRD]). Sub-protocols combine ARPI doublets with drugs targeting specific genomic biomarkers (e.g. docetaxel for RB1, PTEN, and/or TP53 loss; niraparib for DNA damage repair [DDR] deficiency; anti-PD-L1 for mismatch repair [MMR] deficiency).
Sub-protocol (SP) 1 enrolls men whose tumors lack genomic alterations associated with aggressive disease that qualify for other sub-protocols. Sub-protocol 1 includes genomic alterations linked to androgen receptor activity (i.e., ETS fusions, SPOP alterations[alt], and/or FOXA1alt). SP-1 patients are randomized to arm 1a (doublet: LHRHa + apalutamide [APA]) or 1b (triplet: LHRHa + APA + abiraterone acetate/prednisone [AAP]).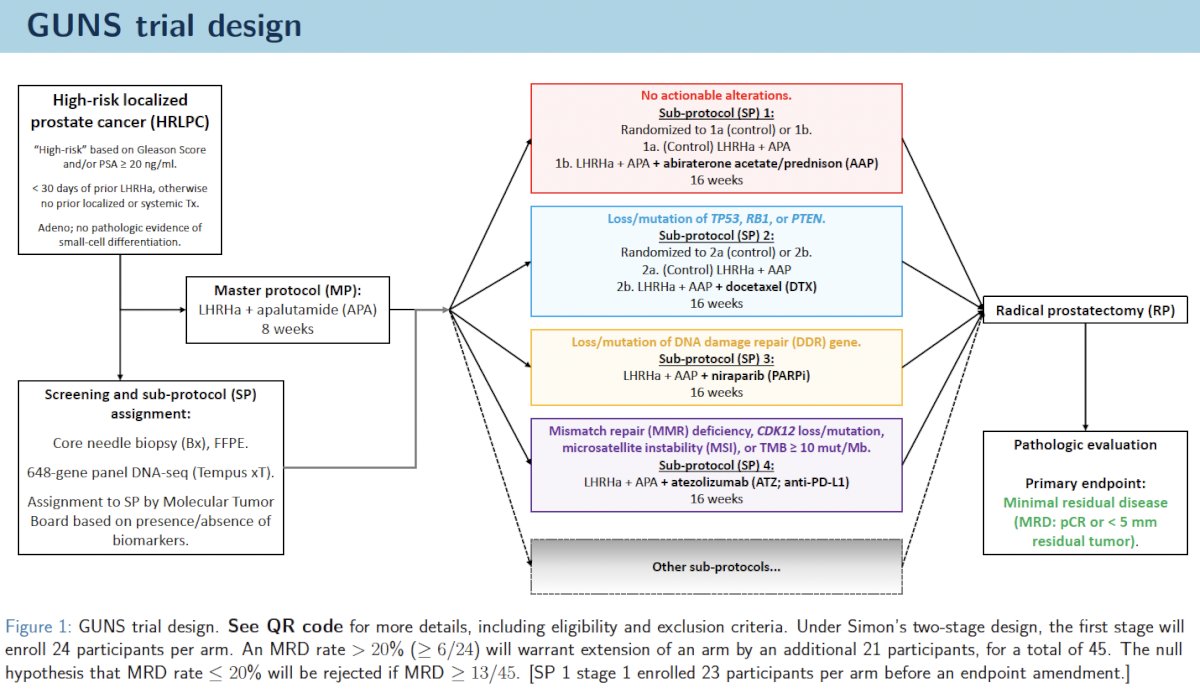
The clinical demographics of GUNS Sub-protocol I participants are summarized below: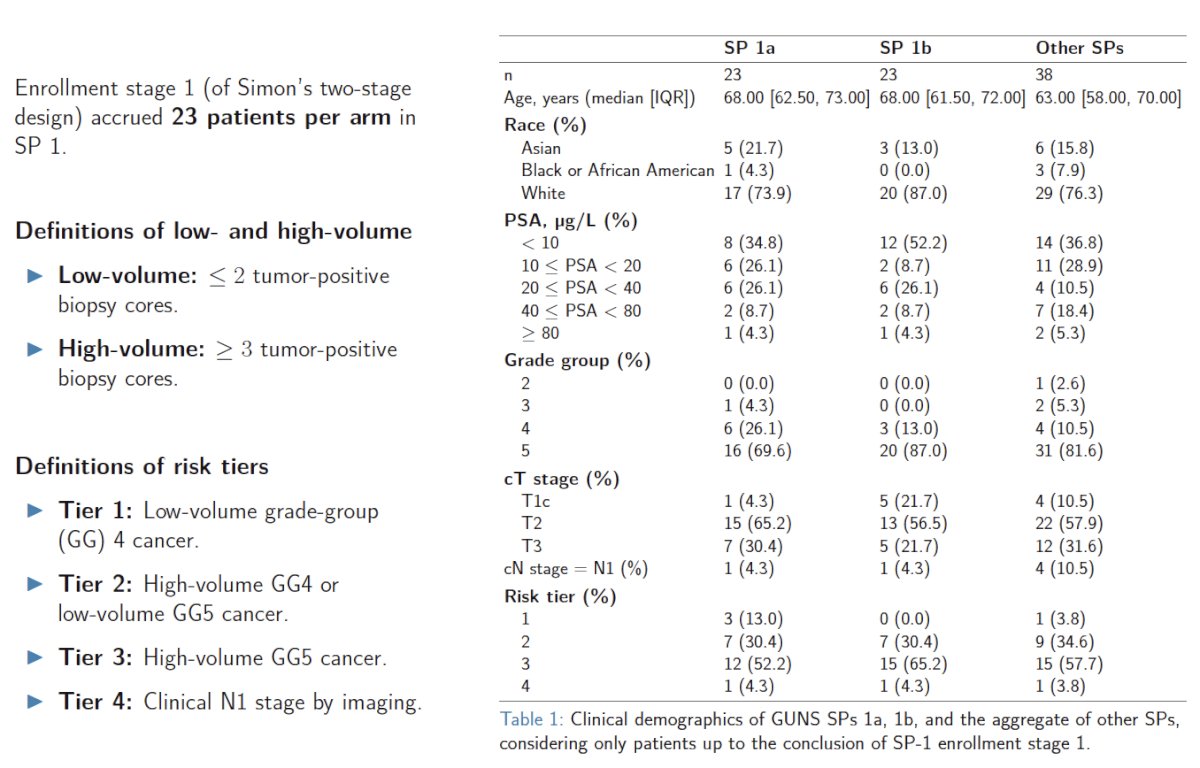
How did the pathologic responses compare between doublet (ADT + APA) and triplet (ADT + APA + AAP) neoadjuvant regimens? No patients achieved a pCR. An MRD was achieved in 48% of triplet therapy versus 13% of doublet therapy patients (p=0.012).
Post-treatment PSA, pT stage, and pN stage were more favorable in the triplet therapy group, although differences did not reach statistical significance. The surgical margin rates were equal in both SP-1 arms.
Cancer degeneration following treatment was scored by pathologists on a scale from 0 to 3. “Degenerative scores” were higher (greater degeneration) with triplet versus doublet therapy.
Genomic alterations linked to AR signaling—ETS gene fusions (35%), FOXA1 mutations and copy gains (23%), and SPOP mutations (15%)—were the most frequently reported genomic alterations in GUNS from September 2021 to October 2024. ETS fusions and FOXA1 alterations occurred at similar rates in sub-protocol 1, as in other sub-protocols. However, SPOP mutations occurred more frequently in sub-protocol 1 patients, compared to patients assigned to other sub-protocols.
There were no statistically significant genomic differences between pre-treatment tumors from MRD than non-MRD cases in sub-protocol 1, although ETS fusions were more commonly present in non-MRD than MRD cases.
Pre-treatment biopsies from GUNS patients enrolled at UBC underwent PTEN immunohistochemistry (IHC). Despite exclusion of genomic PTENalt from sub-protocol 1 (assigned to sub-protocol 2), 7/41(17%) sub-protocol 1 UBC patients had PTEN-IHC-negative tumor biopsies. Negative (≤ 10% cancer cells) PTEN staining by IHC was more common in pre-treatment tumors from non-MRD (6/28; 21%) than MRD (1/13; 8%) patients (p=0.45).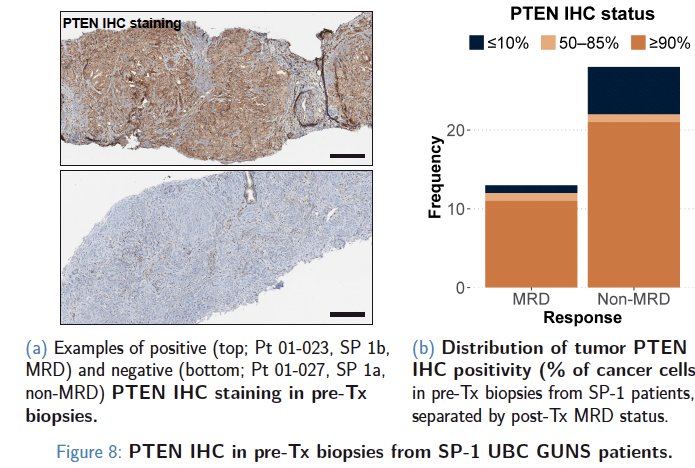
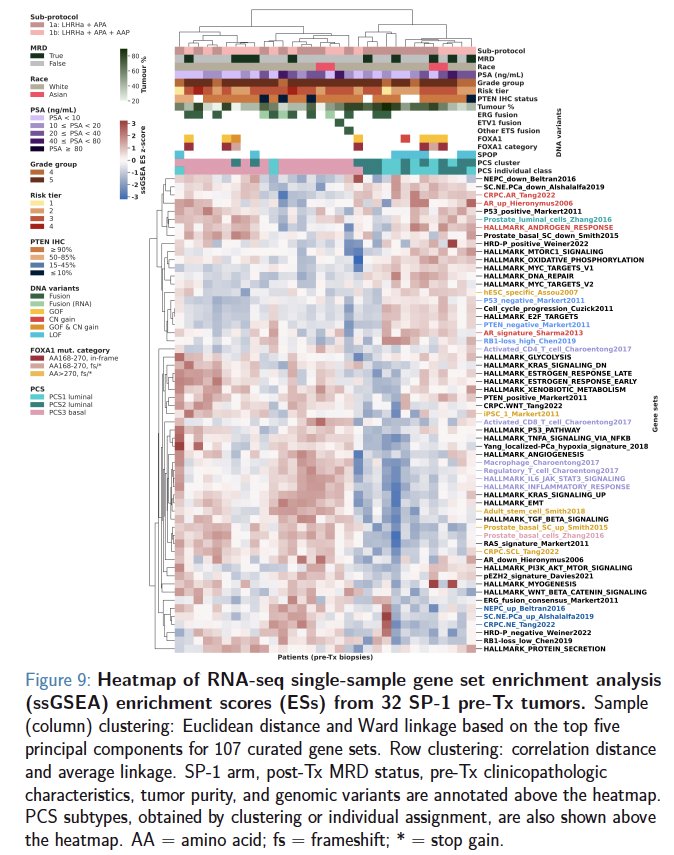
From a transcriptomics standpoint, tumors from MRD and non-MRD cases were not transcriptomically distinct before treatment. Pre-treatment tumors from MRD cases spanned the transcriptomic spectrum of sub-protocol 1 tumors, including luminal and basal phenotypes. Unsupervised hierarchical clustering of RNA-seq data from pre-treatment sub-protocol 1 tumors based on single-sample gene set enrichment scores did not separate MRD cases from non-MRD cases. The clustering predominantly separated tumors with ETS gene fusions (e.g. TMPRSS2–ERG) from tumors with SPOP mutations, and basal (PCS3) tumors from luminal (PCS1/2) tumors.
Providing an overall trial update, Dr. Gleave noted that, overall, 158 patients have been accrued to the GUNS trial, as of January 2025:
- Sub-protocol 1: 65
- Sub-protocol 2: 35
- Sub-protocol 3: 19
- Sub-protocol 4: 6
- Master protocol: 27
New sub-protocols are set to open in 2025:
- SP 5: EZH2 inhibitor (tazemetostat) to target lineage plasticity in genomically aggressive tumors (e.g. TP53alt or RB1alt)
- SP 6: AKT inhibitor (capivasertib) to target PTEN−/AKT-activated tumors
Post- versus pre-treatment analysis of genomics and transcriptomics, including spatial analysis, will be performed to investigate mechanisms and predictors of treatment response/resistance
Dr. Gleave concluded his presentation as follows:
- Genomic alterations associated with AR signaling (ETS gene fusions, FOXA1 alterations, and SPOP mutations) were the most frequent genomic alterations in the GUNS cohort to date.
- Rates of MRD (< 5 mm residual tumor) were higher in sub-protocol 1 patients treated with an ARPI triplet than those treated with a doublet
- Based on these results, sub-protocol 1 has been expanded to its second stage, with a targeted enrollment of 45 participants per arm.
Presented by: Martin Gleave, MD, Distinguished Professor and Head, Department of Urologic Sciences, University of British Columbia, Vancouver, BC
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.