(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Genitourinary (GU) Annual Symposium held in San Francisco, CA between February 13–15, 2025 was host to a trials-in-progress prostate cancer session. Dr. Wenxin Xu presented a post-hoc analysis of CheckMate 214 evaluating circulating kidney injury marker-1 as a prognostic and predictive biomarker in advanced renal cell carcinoma (RCC).
CheckMate 214 demonstrated that the combination of nivolumab + ipilimumab has superior overall survival and durable responses, compared to sunitinib, with 8 years of follow-up in the first line treatment of advanced RCC.1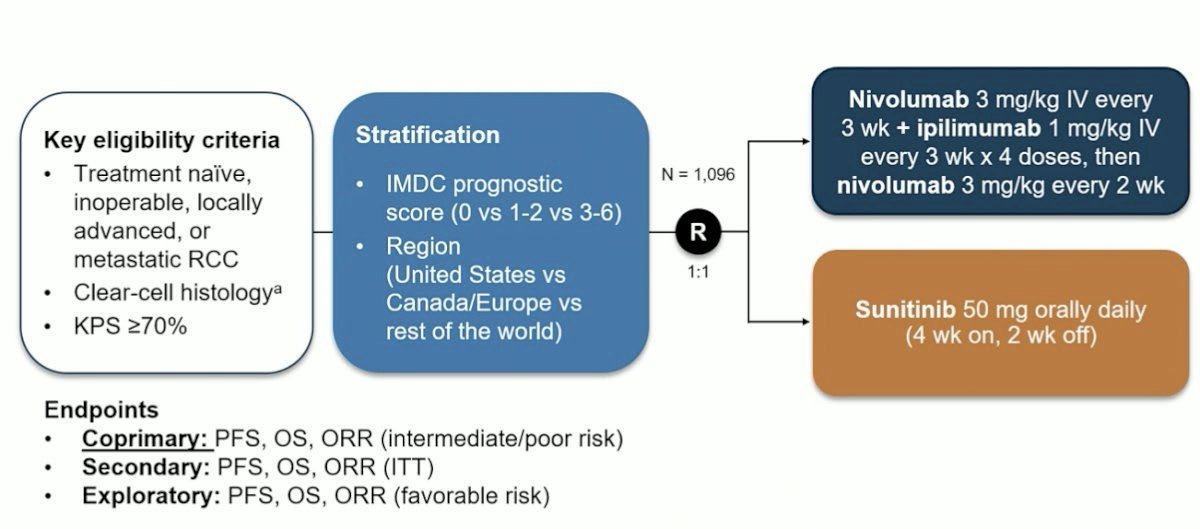
These results continue to support nivolumab + ipilimumab as a 1st line standard of care for intermediate- and poor-risk advanced RCC. However, currently, there are no RCC-specific predictive biomarkers to identify which patients are most likely to respond to this combination therapy.
KIM-1 is a transmembrane protein which is overexpressed in clear cell RCC (ccRCC). The KIM-1 ectodomain is detectable in plasma and serum and is an emerging circulating biomarker for ccRCC. Prior studies have shown that high circulating KIM-1 is a biomarker for:2-5
- Early detection and risk stratification of RCC
- Higher risk of recurrence after nephrectomy (ASSURE, CM 914, IMmotion010)
- Potential benefit from adjuvant immunotherapy (CM 914 Part A, IMmotion010)
In a prior exploratory analysis of a metastatic RCC trial (CheckMate 009):6
- Higher baseline KIM-1 was associated with worse overall survival
- Early decrease in KIM-1 from baseline to 3 weeks was positively associated with improved PFS to Nivolumab
Dr. Xu and colleagues evaluated whether KIM-1 levels at baseline and after 1 cycle of nivolumab + ipilimumab or sunitinib are associated with treatment outcomes in CheckMate 214.
Serum KIM-1 was measured at baseline and 3 weeks after the first dose of nivolumab + ipilimumab (before second dose) using an established enzyme based electrochemiluminescence assay. The investigators were blinded to the identity of clinical samples during laboratory analysis. The association between KIM-1 levels at baseline and clinical outcomes was evaluated using Kaplan-Meier and Cox proportional hazards analyses. Changes in KIM-1 levels were assessed using linear mixed effects models and paired t-tests.
The baseline patient characteristics of the KIM-1 evaluable population are summarized below.
The 821 patients analyzed represent 75% of the CheckMate 214 intent to treat population.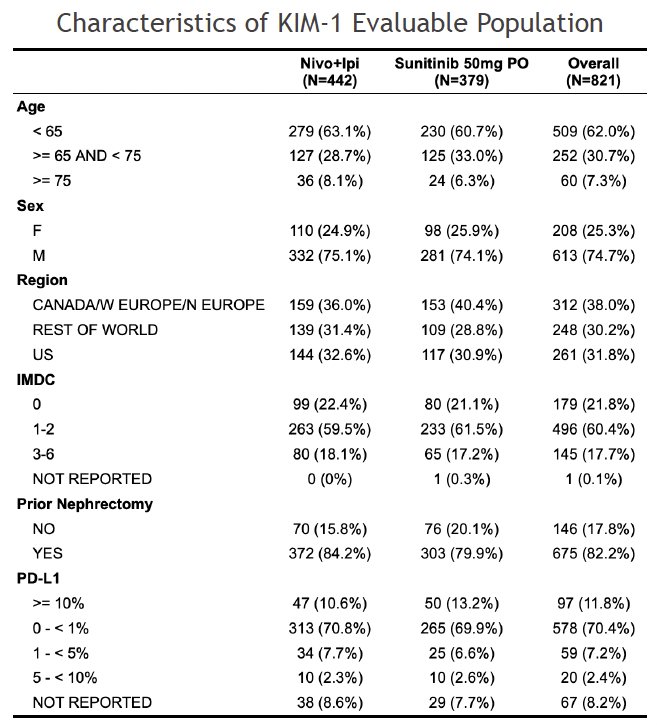
KIM-1 levels at baseline were slightly higher in the sunitinib control arm.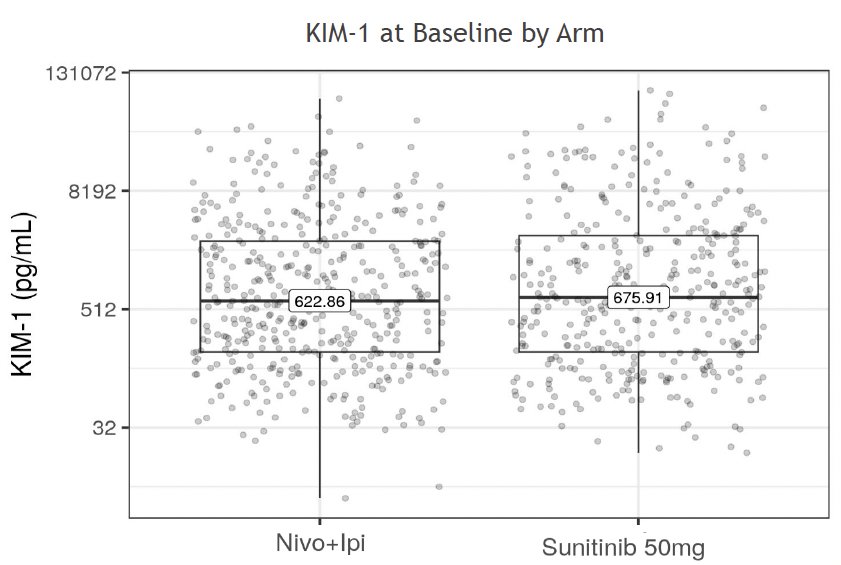
High baseline KIM-1 levels were associated with worse IMDC risk and no prior nephrectomy performed. Baseline KIM-1 was associated with overall tumor burden (measured by sum of target lesion diameters per IRRC).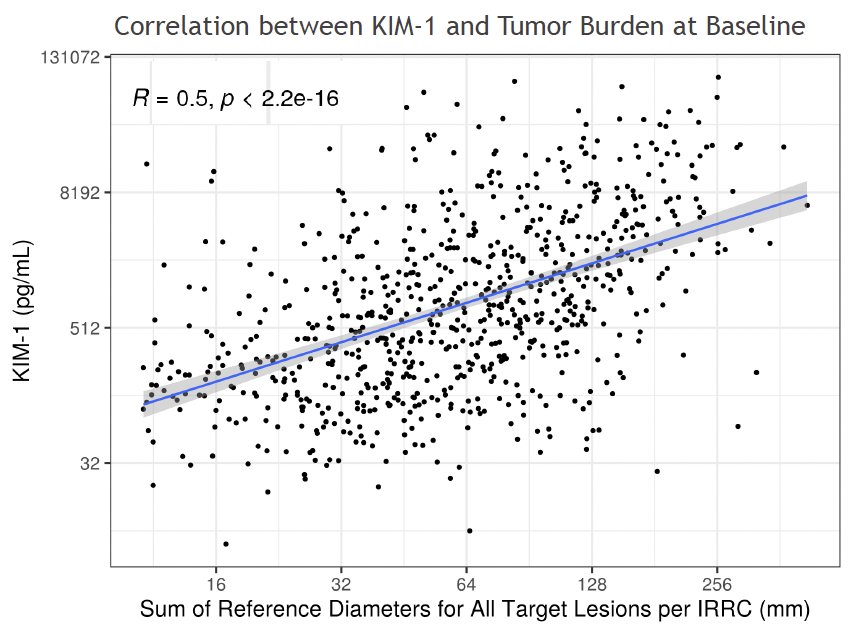
Higher baseline KIM-1 was associated with worse overall and progression free survivals, even after adjustment for IMDC risk and baseline tumor burden in multivariable models. 
In both nivolumab + ipilimumab and sunitinib, circulating KIM-1 levels were overall lower after 3 weeks of treatment compared to baseline.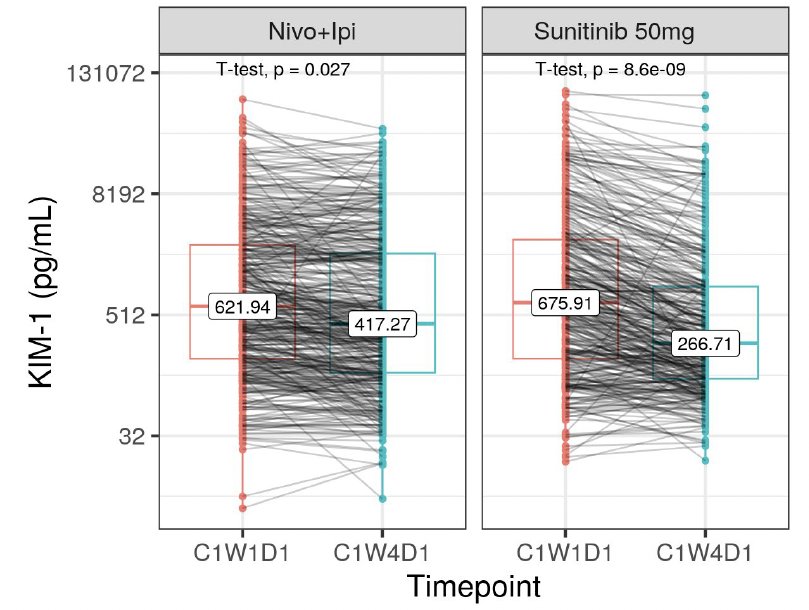
A decrease in KIM-1 levels at 3 weeks post-treatment initiation was strongly associated with a subsequent radiographic response in the nivolumab + ipilimumab, but not sunitinib arm.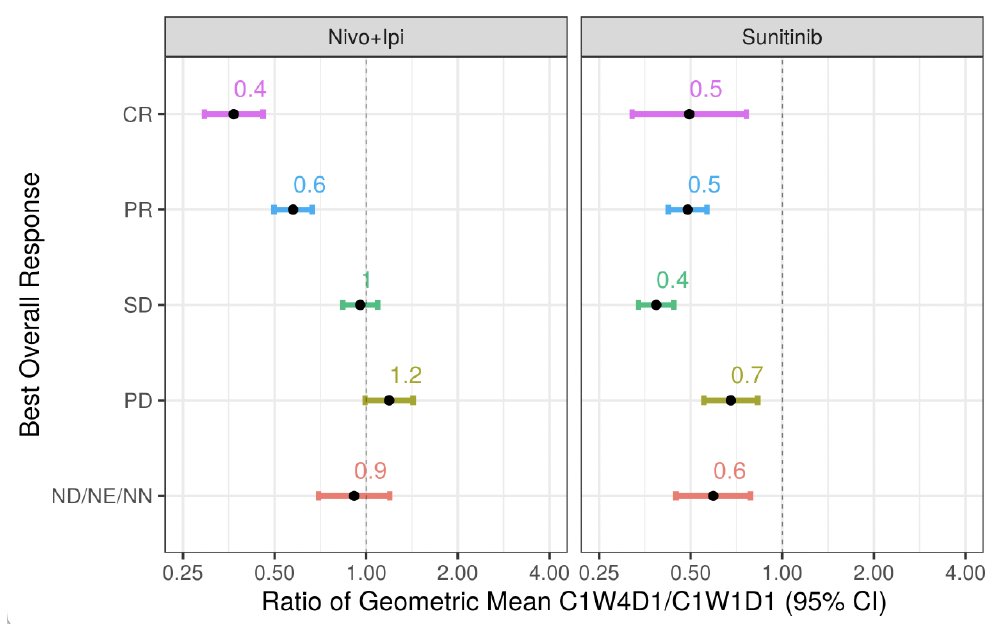
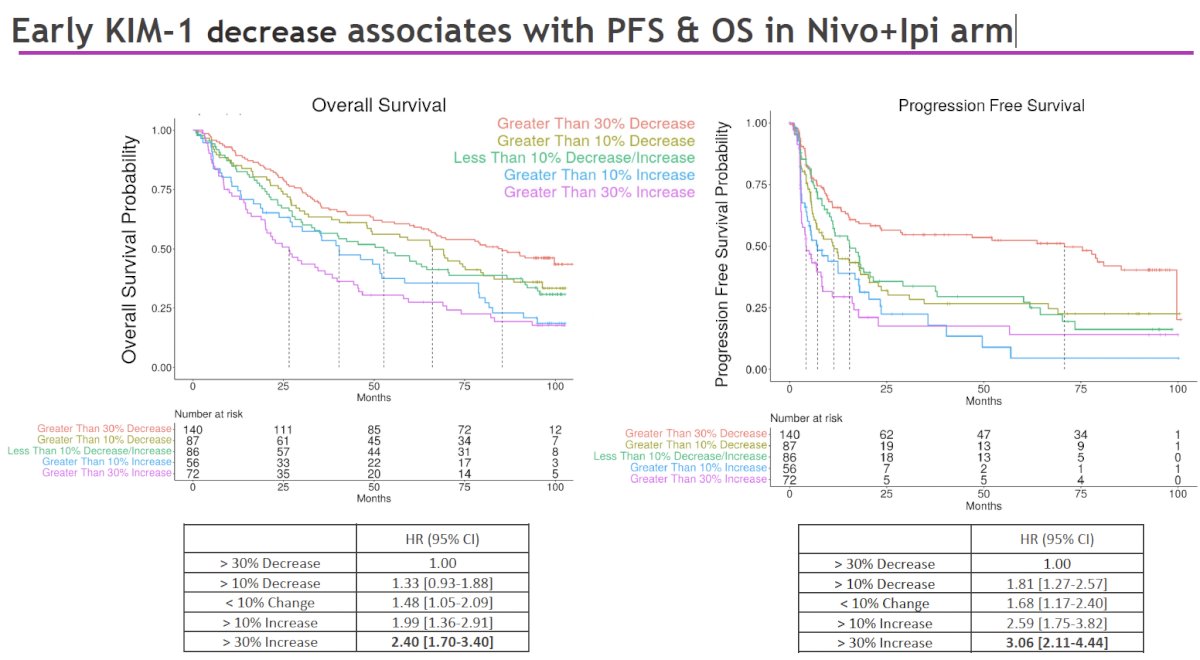
Patients with a 30% decrease in KIM-1 after 3 weeks of treatment had over 3-fold longer median OS and 17-fold longer median PFS compared to those with a 30% increase.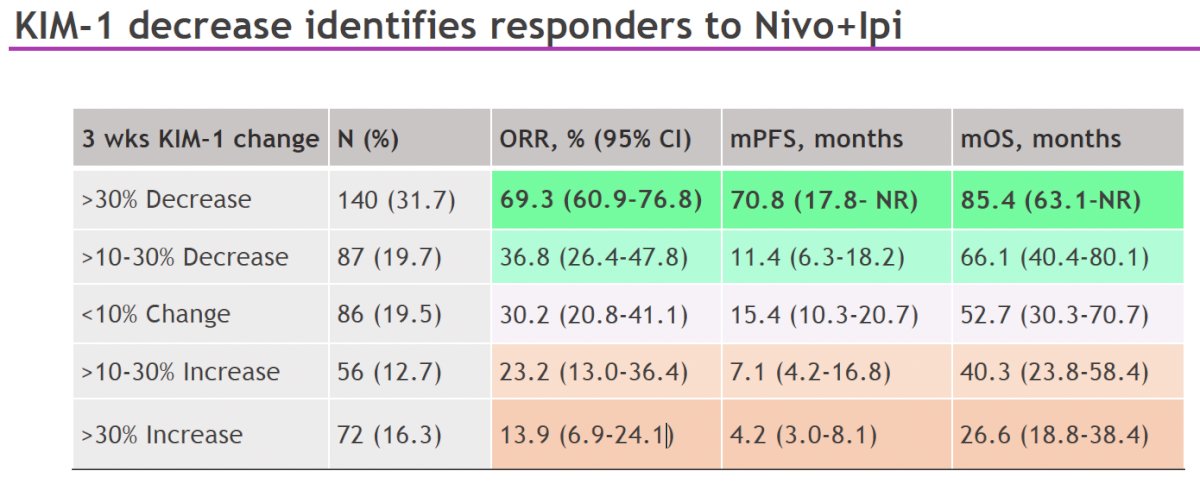
KIM-1 decrease after 3 weeks was not associated with response to sunitinib:
Dr. Xu concluded as follows:
- In CheckMate 214, this post hoc analysis shows that early change in serum KIM-1 just 3 weeks after nivolumab + ipilimumab is associated with long-term efficacy of this IO doublet, but not with sunitinib
- Higher baseline KIM-1 was associated with worse clinical outcomes in both the nivolumab + ipilimumab and sunitinib arms
- These findings are being confirmed in other metastatic RCC trials
- Circulating KIM-1 should be evaluated prospectively as a potential early biomarker for response to RCC immunotherapy
Presented by: Wenxin Xu, MD, Medical Oncologist, Dana-Farber Cancer Institute, Boston, MA
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
References:- Motzer RJ, Tannir NM, McDermott DF, et al. Nivolumab plus Ipilimumab versus Sunitinib in Advanced Renal-Cell Carcinoma. N Engl J Med 2018;378(14):1277-1290.
- Scelo G, Larose TL. Epidemiology and Risk Factors for Kidney Cancer. J Clin Oncol. 2018; 36(36): JCO2018791905.
- Xu W, Gaborieau V, Niman SM, et al. Plasma Kidney Injury Molecule-1 for Preoperative Prediction of Renal Cell Carcinoma Versus Benign Renal Masses, and Association With Clinical Outcomes. J Clin Oncol. 2024; 42:22.
- Xu W, Puligandla M, Halbert B, et al. Plasma KIM-1 Is Associated with Recurrence Risk after Nephrectomy for Localized Renal Cell Carcinoma: A Trial of the ECOG-ACRIN Research Group (E2805). Clin Cancer Res. 2021; 27(12):3397-403.
- Albiges L, Bex A, Suarez C, et al. Circulating kidney injury molecule-1 (KIM-1) biomarker analysis in IMmotion010: A randomized phase 3 study of adjuvant (adj) atezolizumab (atezo) vs placebo (pbo) in patients (pts) with renal cell carcinoma (RCC) at increased risk of recurrence after resection. J Clin Oncol. 2024; 42:Number 16_suppl.
- Xu W, Vemula SV, Niman SM, et al. Circulating KIM-1 is a minimally invasive biomarker correlated with treatment response to nivolumab in patients with metastatic renal cell carcinoma. KCRS 2023 Meeting.