(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Genitourinary (GU) Annual Symposium held in San Francisco, CA between February 13–15, 2025 was host to a renal cell cancer oral abstract session. Dr. Robert Motzer presented the final follow-up results from the CheckMate 9ER trial of nivolumab (NIVO) plus cabozantinib (CABO) versus sunitinib (SUN) for previously untreated advanced renal cell carcinoma (aRCC).
The combination of NIVO+CABO showed significant efficacy benefits, compared to SUN, for patients with previously untreated aRCC in the primary analysis (median follow-up, 18.1 months) of the phase III CheckMate 9ER trial:1
- PFS per BICR: Median 16.6 vs 8.3 months; HR: 0.51, p< 0.001
- OS: Medians not reached; HR: 0.60, p=0.001
- ORR per BICR: 55.7% vs 27.1%, p< 0.001
Herein, Dr. Motzer presented the final efficacy and safety results of the CheckMate 9ER trial with a long-term median follow-up of 67.6 months.
In this phase III trial, patients with aRCC and a clear cell component, irrespective of IMDC risk group, were randomized to nivolumab 240 mg every 2 weeks + cabozantinib 40 mg once daily vs sunitinib 50 mg once daily (4 weeks on/2 weeks off) until disease progression or unacceptable toxicity, with up to 2 years of nivolumab. The primary endpoint was progression-free survival per RECIST v1.1 by blinded independent central review (BICR). Secondary endpoints included overall survival, objective response rate per RECIST v1.1 by BICR, and safety.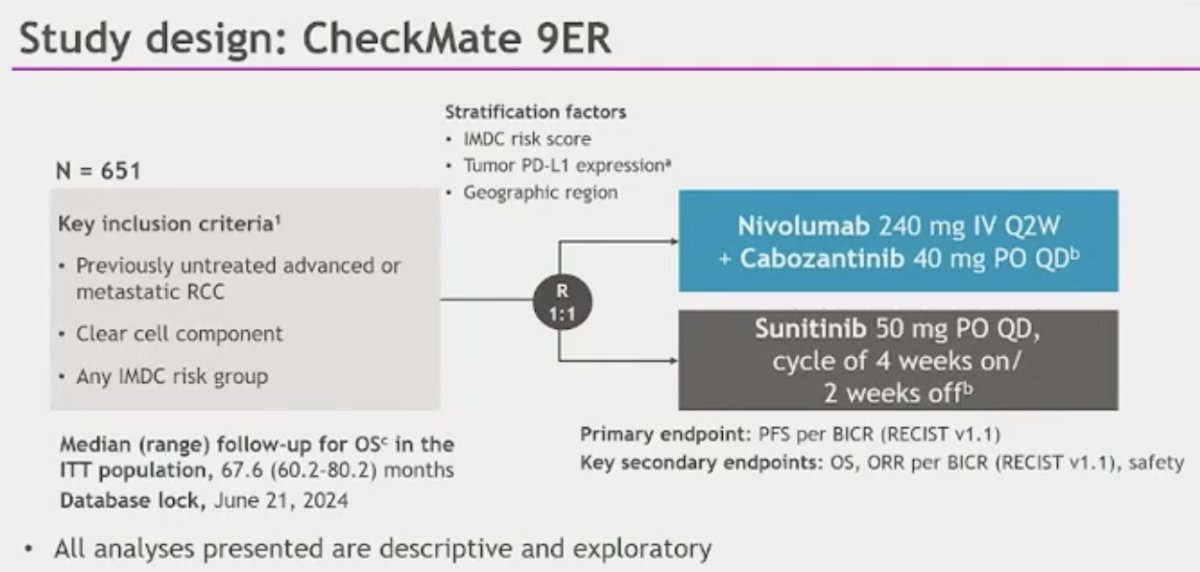
Overall, 323 patients were randomized to nivolumab + cabozantinib and 328 to sunitinib, with treatment arms well-balanced for baseline characteristics.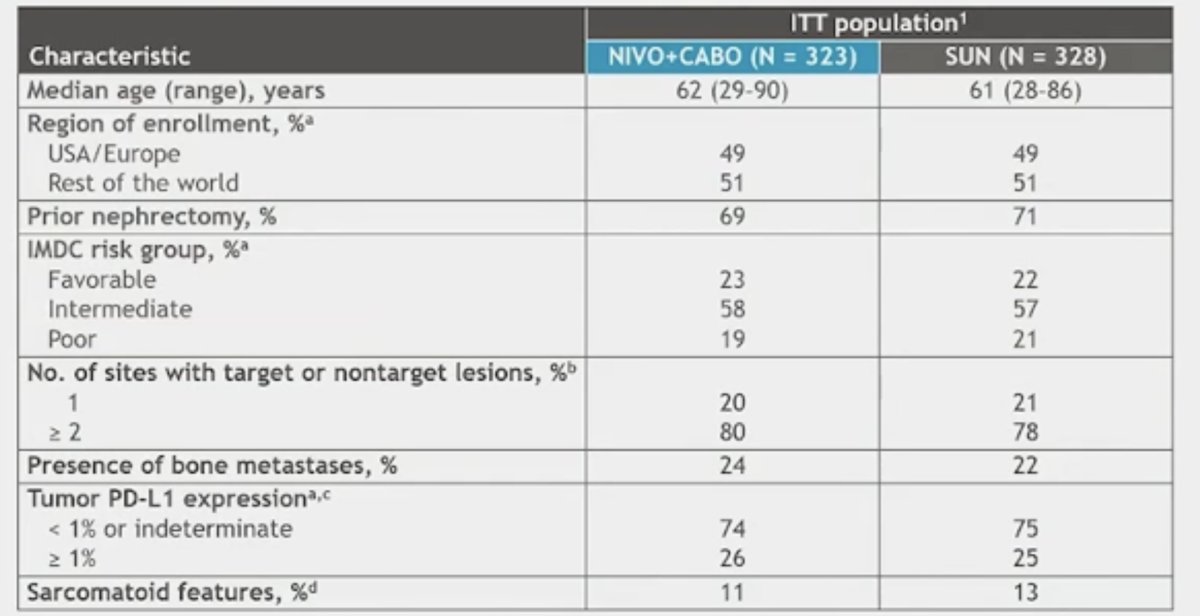
At this updated follow-up, the median PFS remained higher in the NIVO + CABO arm (median: 16.4 versus 8.3 months; HR: 0.58, 95% CI: 0.49–0.70).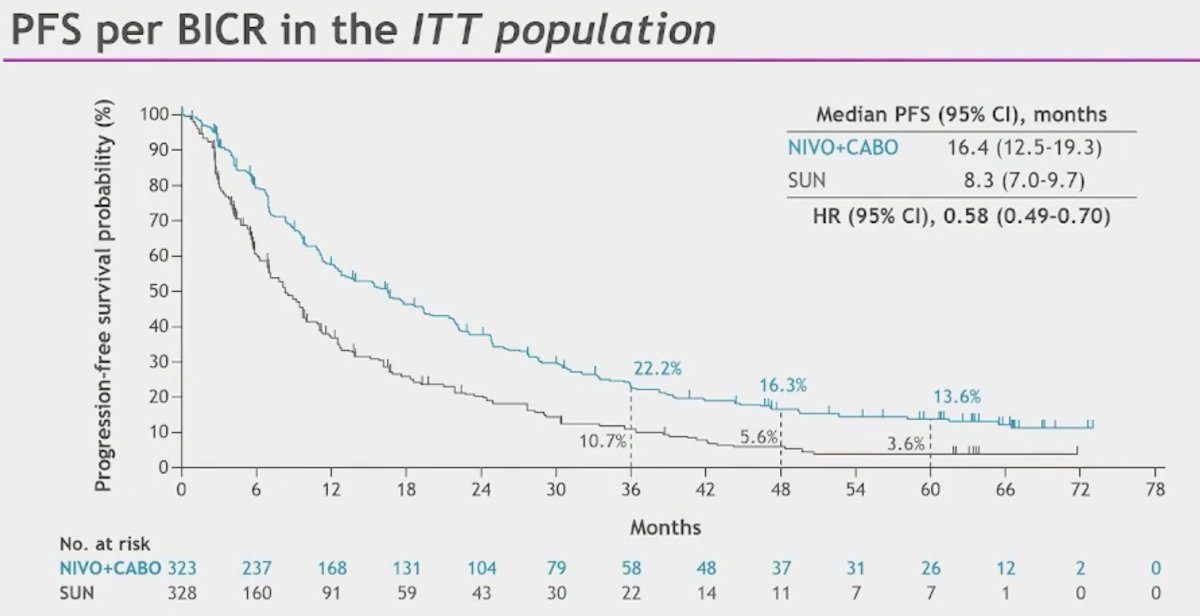
Overall survival continued to favor the NIVO + CABO arm (median: 46.5 versus 35.5 months; HR: 0.79, 95% CI: 0.65–0.96):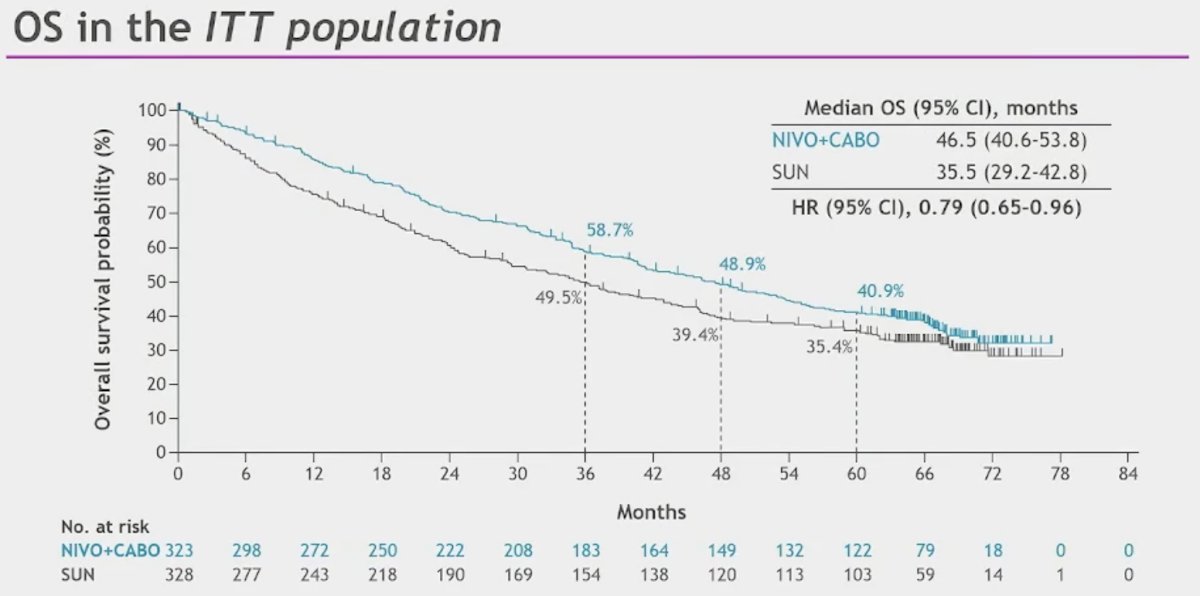
The ORR was two-fold higher in the NIVO + CABO arm (55.7% versus 27.4%). A complete response was observed in 14% of NIVO + CABO patients, and a partial response was observed in 42%. Only 6.5% of patients had progressive disease as their best objective response.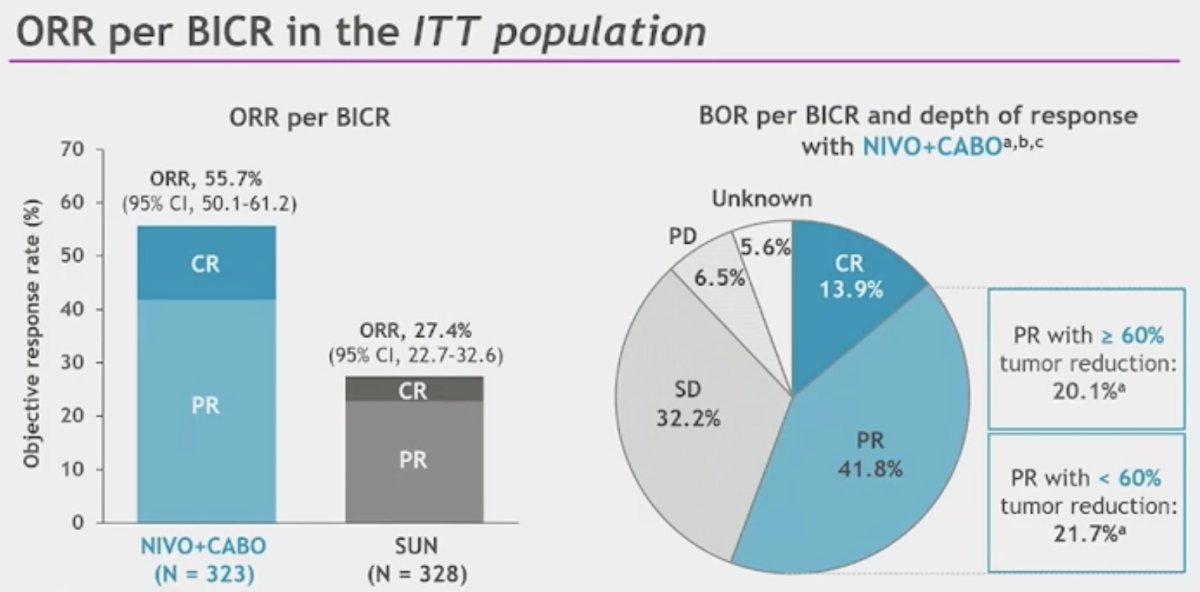
Responses were durable with a median duration of response of 22 months in the NIVO + CABO arm.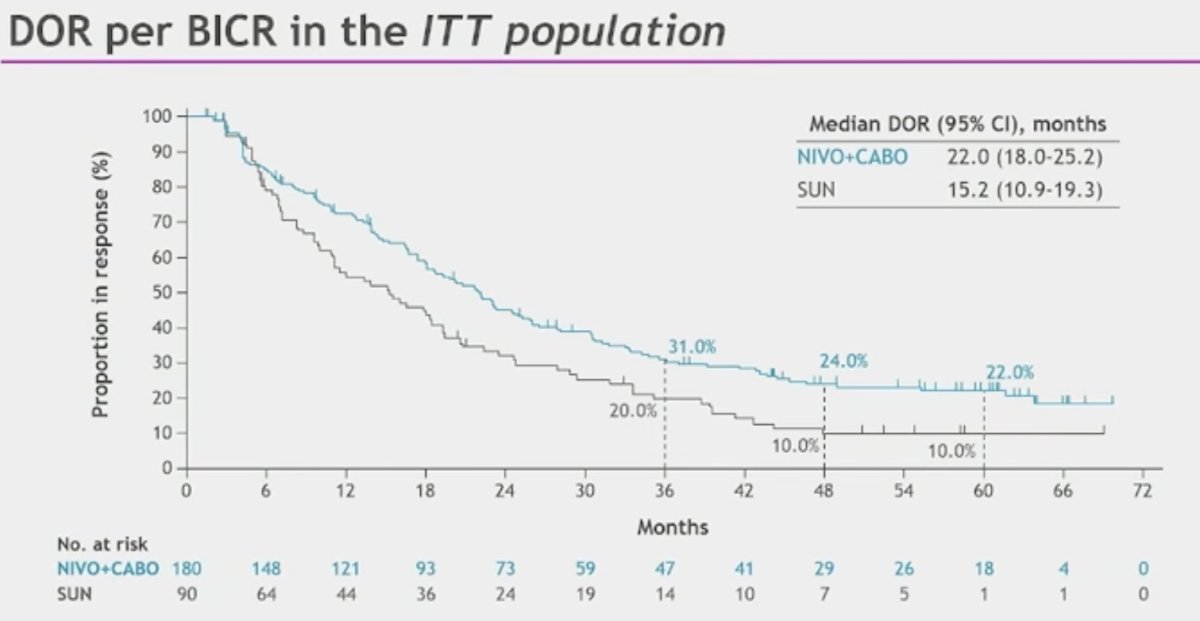
PFS, OS, and ORR in the IMDC favorable risk group are illustrated below. Notably, there was no significant OS benefit for NIVO + CABO versus sunitinib (median: 53.7 versus 58.9 months; HR: 1.08, 95% CI: 0.70–1.66):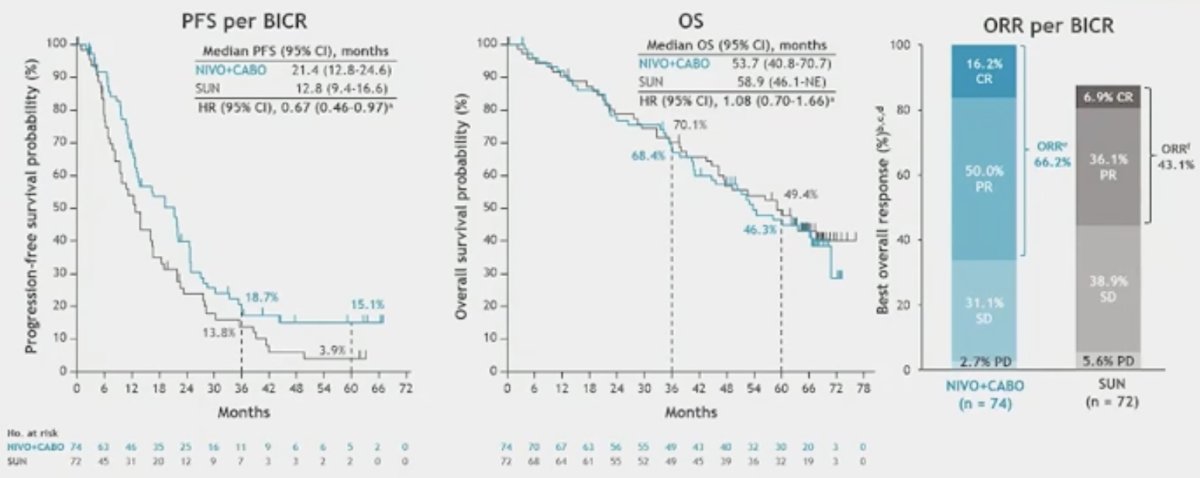
In the IMDC intermediate/poor risk group, significant PFS (15.4 versus 7.1 months) and OS (43.9 versus 29.2) benefits were observed with NIVO + CABO: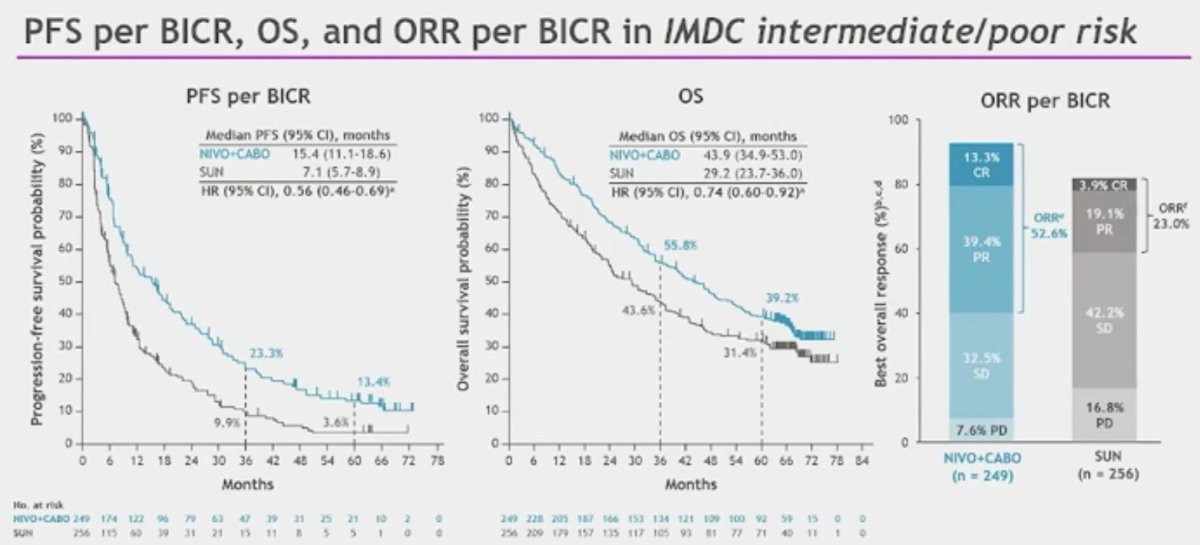
Efficacy outcomes by baseline organ sites of metastases all favored NIVO + CABO (HRs 0.43–0.75):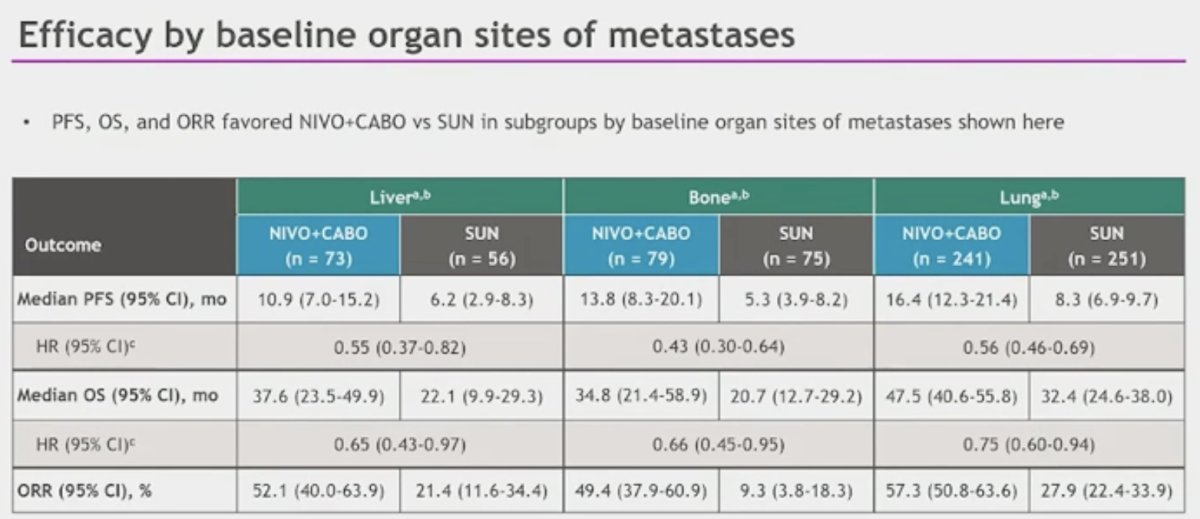
Almost all patients had discontinued study treatment at the time of analysis. 43% of NIVO + CABO patients received subsequent systemic therapy versus 55% of SUN patients. More patients in the SUN arm subsequently received any PD-(L)1 inhibitor (81% versus 36%), whereas NIVO + CABO patients were more likely to receive any VEGF(R) inhibitor (79% versus 51%) as next-line therapy.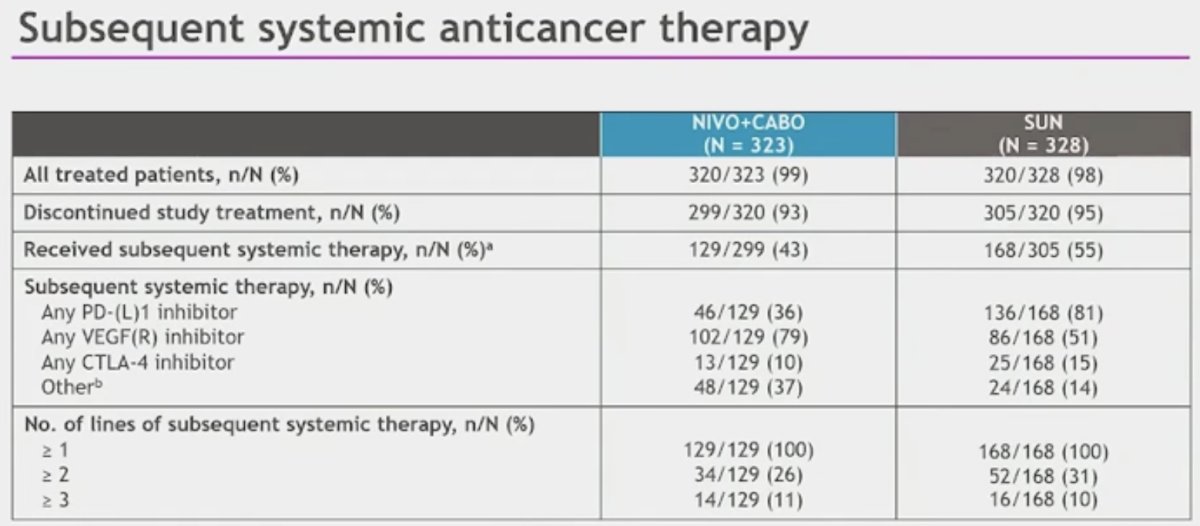
The median duration of therapy was 21.8 and 8.9 months in the NIVO + CABO and SUN arms, respectively.
Treatment-related AEs are summarized below. Grade 3–4 adverse events were observed in 68% and 55% of patients in the NIVO + CABO and SUN arms, respectively. There were no new safety signals with this extended follow-up.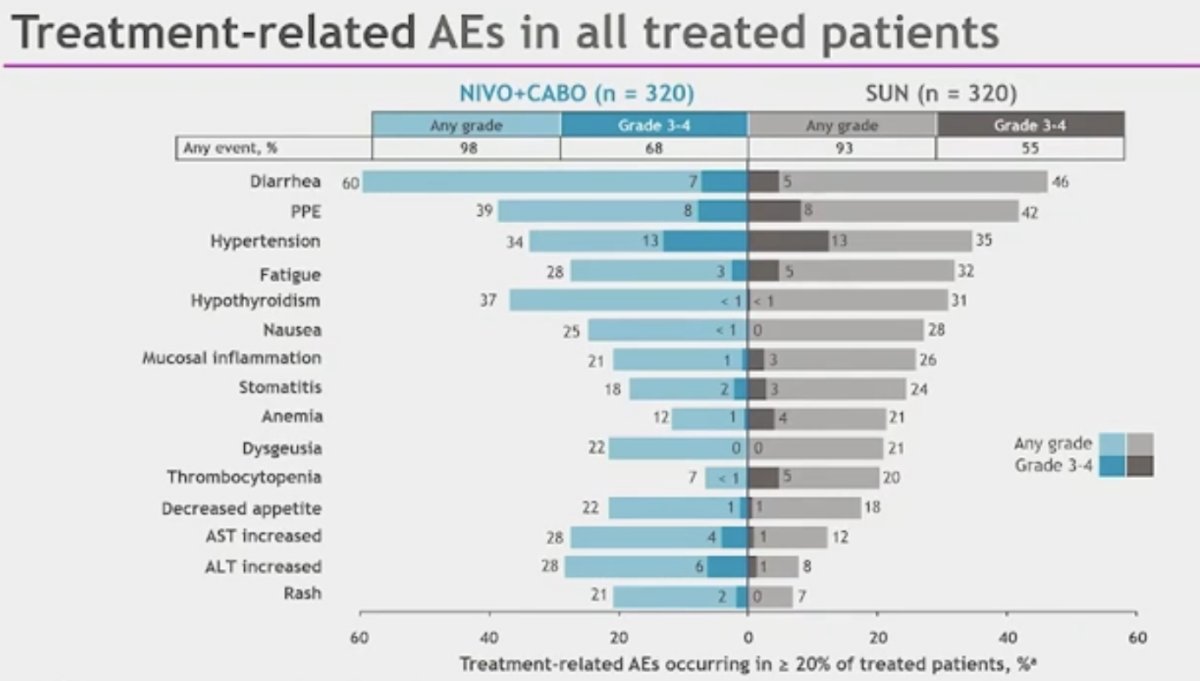
14% of patients developed immune-related Grade 3–4 adverse events, with thyroid abnormalities the most common adverse event. 13% and 5% of patients received corticosteroids at a dose of ≥40 mg for ≥2 weeks and ≥30 days, respectively.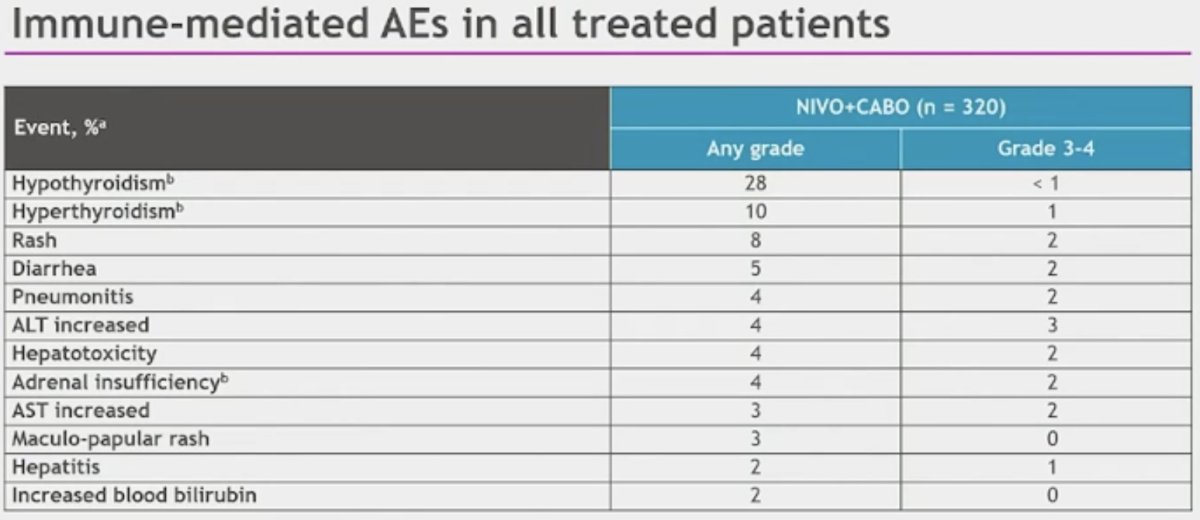
Dr. Motzer concluded as follows:
- A long-term efficacy benefit was observed with NIVO + CABO over SUN in these final results from the CheckMate 9ER trial, with a median follow up of 67.6 months
- Safety and tolerability with long-term follow-up were manageable and consistent with previous follow-up
- The results continue to support NIVO + CABO as a standard of care for previously untreated aRCC
- As subcutaneous NIVO has been shown to provide clinical equipoise to standard IV dosing, it could be considered as an alternative for patients with aRCC.
Presented by: Robert Motzer, MD, Attending Physician, Medical Oncologist, Memorial Sloan Kettering Cancer Center, New York, NY
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
Reference: