(UroToday.com) The 2025 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA was host to the Rapid Oral Abstract Session C: Renal Cell Cancer. Dr. Wen Kong presented Abstract 443: Lenvatinib plus tislelizumab as first-line therapy for advanced fumarate hydratase-deficient renal cell carcinoma: A single-center, single-arm, phase II study.
Dr. Kong began his presentation by highlighting that this was a prospective investigator-initiated trial conducted in China. He noted that fumarate hydratase-deficient renal cell carcinoma (FH-RCC) is a rare and aggressive subtype of RCC with a poor prognosis.
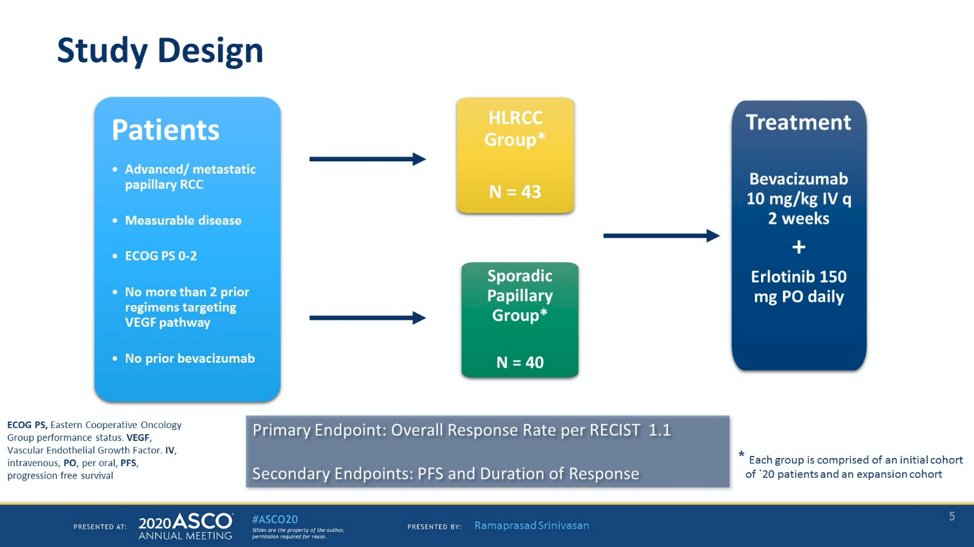
Bevacizumab plus erlotinib has demonstrated significant anti-tumor activity and is a recommended treatment option in the NCCN Kidney Cancer guidelines for these patients. This recommendation is based on results from a Phase II study evaluating bevacizumab and erlotinib in patients with advanced hereditary leiomyomatosis and renal cell carcinoma (HLRCC) or sporadic papillary RCC.1
The primary endpoint of the study was the objective response rate (ORR), which was 54% across all patients. In the HLRCC cohort, the ORR was 72%, while in the sporadic papillary RCC group, it was 35%. The median progression-free survival (PFS) was 21.1 months for patients with HLRCC and 8.8 months for those with sporadic papillary RCC. These findings confirm that the combination of bevacizumab and erlotinib is highly active in patients with papillary RCC, particularly those with FH deficiency. Notably, this trial was designed over 10 years ago, and treatment for RCC has changed drastically in the last decade. Below is the study design of this study:
However, a Retrospective study showed comparable response rates for patients with FH-deficient RCC between first-line ICI/TKI and Bevacizumab/Erlotinib, but the ICI/TKI group had better survival (2) as shown below:

Tislelizumab is a monoclonal antibody that targets the PD-1 protein on T cells and has the potential to enhance treatment outcomes for FH-deficient RCC when combined with a TKI. To evaluate the efficacy of the Tislelizumab + Lenvatinib combination in this setting, researchers proposed this trial.
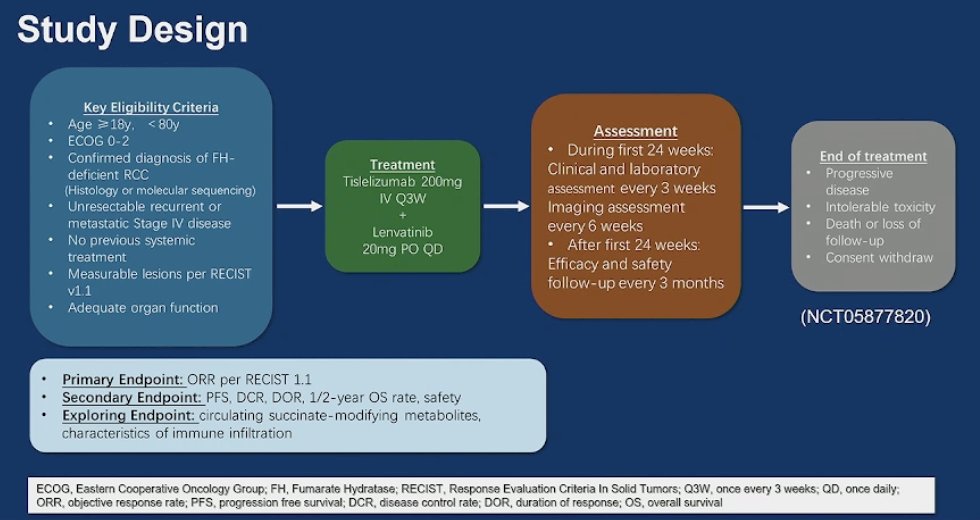
Eligible patients were 18 to 80 years old with pathologically confirmed, unresectable, advanced, or metastatic FH-RCC. They had measurable disease per RECIST 1.1 and no prior systemic therapy. FH-RCC diagnosis was confirmed through DNA sequencing, identifying germline or somatic FH mutations. Patients received lenvatinib 20 mg orally once daily and tislelizumab 200 mg intravenously every three weeks until disease progression, intolerable toxicity, or withdrawal of consent. The primary endpoint was objective response rate (ORR), while secondary endpoints included disease control rate (DCR), progression-free survival (PFS), duration of response (DOR), 1-year and 2-year overall survival (OS) rates, and safety. The study design is shown below:
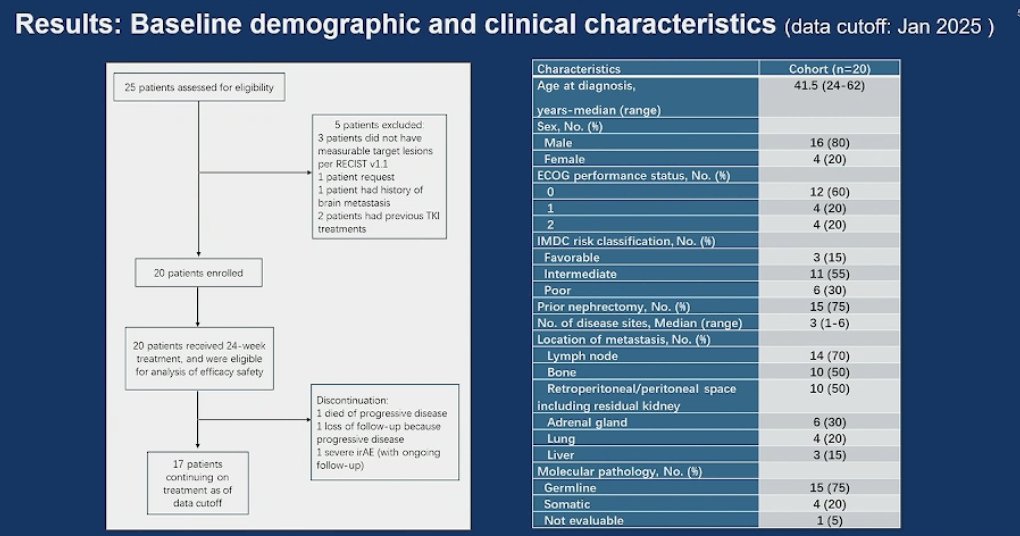
Dr. Kong noted that 20 patients were enrolled between September 2023 and January 2025. Notably, three-quarters had a history of nephrectomy. The most common sites of recurrence were the lymph nodes, followed by bone metastases, retroperitoneal space, and renal fossa recurrence. Germline mutations were identified in 75% of patients. Baseline characteristics are summarized below.
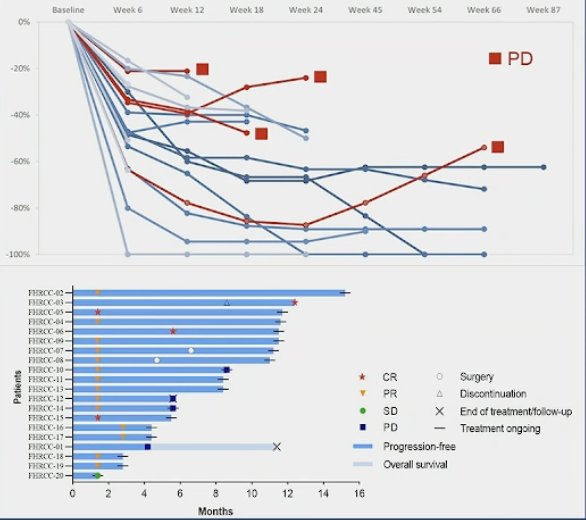
The median follow-up was 9.7 months (range: 1.4–15.2). The objective response rate (ORR) was 90% (18/20), and the disease control rate (DCR) was 100%. Both hereditary and sporadic FH-RCC benefited from the treatment.

The median time to response was 6 weeks. No primary progression was observed, as all patients achieved at least stable disease (SD) at 12 weeks, with some degree of tumor shrinkage. At the latest assessment, four patients experienced progressive disease (PD): one patient died, one suffered a pathological fracture, and one progressed while on tislelizumab. In total, four progression-free survival (PFS) events and one overall survival (OS) event occurred. Median PFS and OS were not reached, but the 6-month PFS and OS rates were 85% and 100%, respectively. Three patients underwent definitive surgery with or without radiotherapy. At the last follow-up, 17 out of 20 patients remained on treatment as shown in the Swimmer’s plot below:
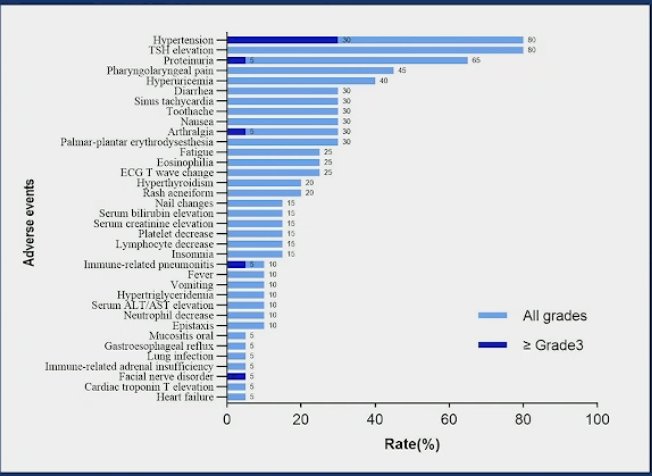
In terms of safety, all patients (100%) experienced treatment-related adverse events (AEs). Grade ≥3 AEs were reported in 45% (9/20) of patients. Lenvatinib dose reduction was required in 45% (9/20) of cases, while tislelizumab was discontinued in 15% (3/20) of patients.
Dr. Kong concluded his presentation with the following key messages:
- Lenvatinib plus tislelizumab demonstrated promising anti-tumor efficacy with an acceptable toxicity profile.
- ORR was 90%, including a 20% complete response rate.
- No primary progression was observed; all patients achieved disease control.
- The adverse event profile was consistent with previous reports.
- ICI/TKI combination may be a promising first-line treatment option for advanced FH-RCC.
- Limitations of the study include short follow-up, immature data, and a small sample size.
- The study was single-center and single-arm; expanded validation is needed.
- Data on exploratory endpoints have not yet been reported.
Presented by: Wen Kong, MD, Department of Urology, Renji Hospital, School of Medicine, Shanghai Jiao Tong University School of Medicine. Shanghai, China.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
Related content: Combination Lenvatinib-Tislelizumab for Fumarate Hydratase-Deficient Renal Cell Carcinoma - Wen Kong
- Ramaprasad Srinivasan et al., Results from a phase II study of bevacizumab and erlotinib in subjects with advanced hereditary leiomyomatosis and renal cell cancer (HLRCC) or sporadic papillary renal cell cancer.. JCO 38, 5004-5004(2020) DOI:10.1200/JCO.2020.38.15_suppl.5004
- Xu Y, Kong W, Cao M, Wang J, Wang Z, Zheng L, Wu X, Cheng R, He W, Yang B, Dong B, Pan J, Chen Y, Huang J, Jiang C, Zhai W, Li F, Chen R, Zhou X, Wu G, Geng X, Chen J, An H, Yuan Y, Xu T, Chen D, Lin D, Xu L, Huang K, Peng L, Yu Y, Tai S, Qi H, Luo K, Kang X, Wang H, Huang Y, Zhang J, Xue W. Genomic Profiling and Response to Immune Checkpoint Inhibition plus Tyrosine Kinase Inhibition in FH-Deficient Renal Cell Carcinoma. Eur Urol. 2023 Feb;83(2):163-172. doi: 10.1016/j.eururo.2022.05.029. Epub 2022 Jun 15. PMID: 35715365.