(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Genitourinary (GU) Annual Symposium held in San Francisco, CA was host to a renal cell cancer oral abstract session. Dr. Laurence Albiges presented the final results of COSMIC-313 of cabozantinib (cabo) in combination with nivolumab (nivo) plus ipilimumab (ipi) in previously untreated advanced renal cell carcinoma (aRCC).
COSMIC-313 evaluated the triplet strategy of cabo + nivo + ipi versus placebo + nivo + ipi in patients with previously untreated aRCC of intermediate or poor risk, per IMDC criteria. At a median follow-up of 14.9 months, the primary analysis demonstrated significantly prolonged PFS with the addition of cabo to nivo + ipi (median PFS: not reached versus 11.3 months; HR: 0.73, 95% CI: 0.57–0.94, p=0.01). Notably, a greater PFS benefit was observed in IMDC intermediate-risk, compared to poor-risk disease patients:
- Intermediate risk: HR=0.63, 95% CI: 0.47–0.85
- Poor risk: HR=1.04, 95% CI: 0.65–1.69
Herein, Dr. Albiges presented the results of the secondary endpoint of OS, updated PFS and safety, and exploratory biomarker analyses.
In this global, double-blind, randomized phase III study, the study investigators enrolled previously untreated patients with clear cell aRCC of IMDC intermediate or poor risk. Patients were randomized to receive cabozantinib 40 mg once daily or matched placebo, stratified by region and IMDC risk. All enrolled patients, regardless of randomized group, received nivolumab (3 mg/kg intravenously every 3 weeks) and ipilimumab (1 mg/kg intravenously every 3 weeks) for 4 cycles followed by nivolumab (480 mg IV every 4 weeks). Nivolumab was continued up to a maximum of 2 years.
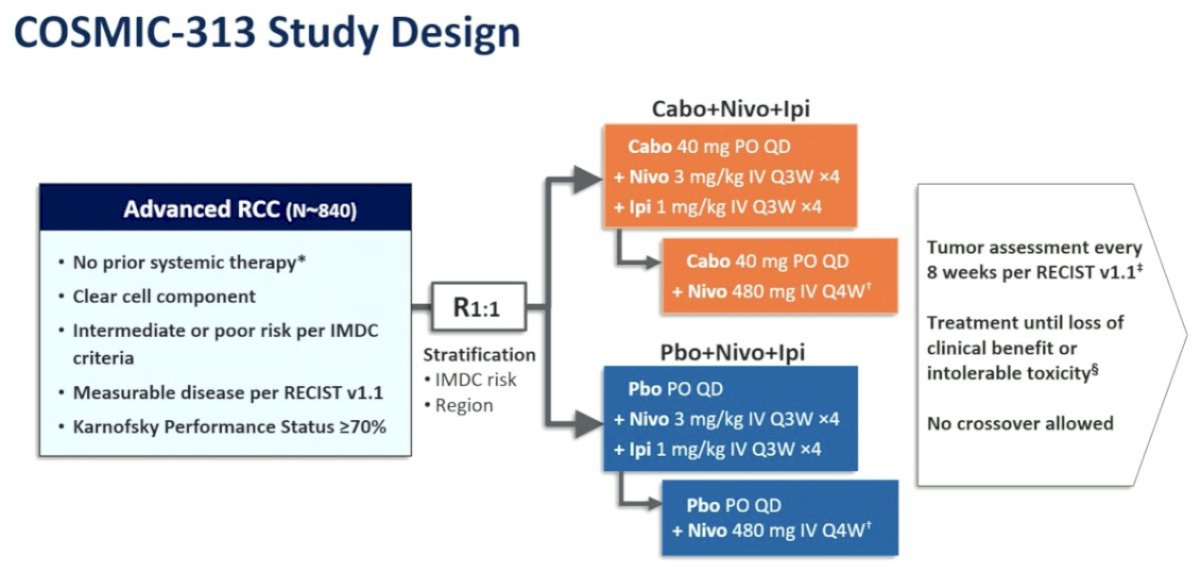
The primary endpoint was progression-free survival (PFS) by blinded independent radiology review per RECIST 1.1 in the first 550 randomized patients (PITT population). The secondary endpoint was overall survival (OS) in all randomized patients (ITT population); objective response rate (ORR) and safety were additional endpoints.
Between June 2019 and March 2021, 855 patients were randomized of whom 428 received cabozantinib, nivolumab, and ipilimumab and 427 received placebo, nivolumab, and ipilimumab. In the overall cohort, IMDC risk was intermediate for 75% and poor for 25%. The median follow-up for this analysis was 45 (range: 37.4–58.5) months.

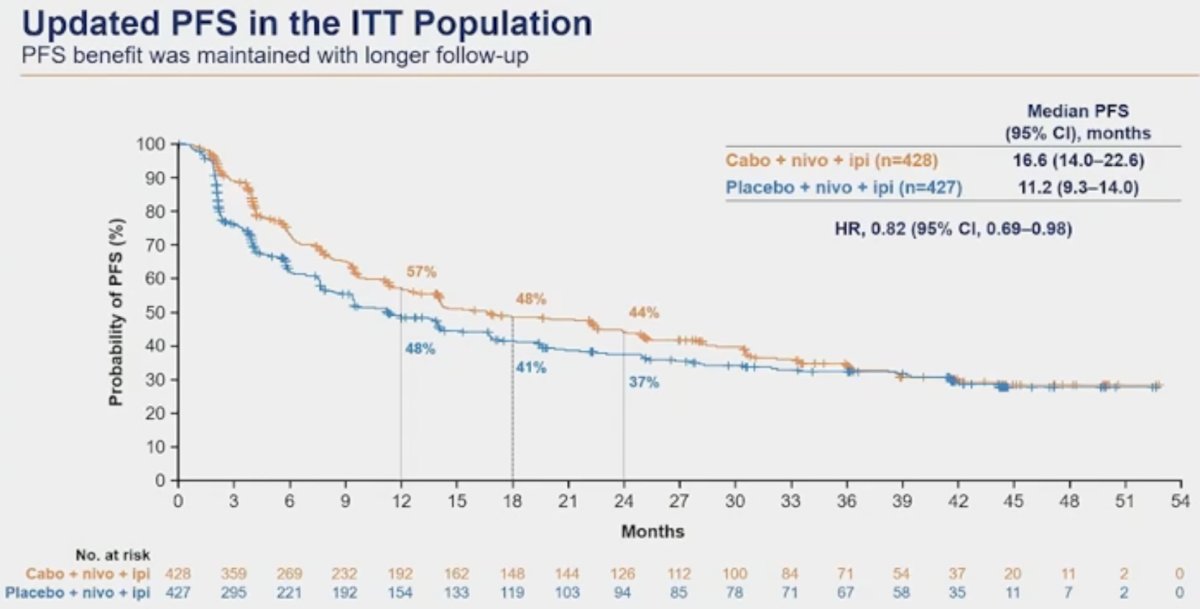
The updated PFS analysis demonstrated a continued significant benefit in favor of the addition of cabo to ipi + nivo (median: 16.6 versus 11.2 months; HR: 0.82, 95% CI: 0.69–0.98):
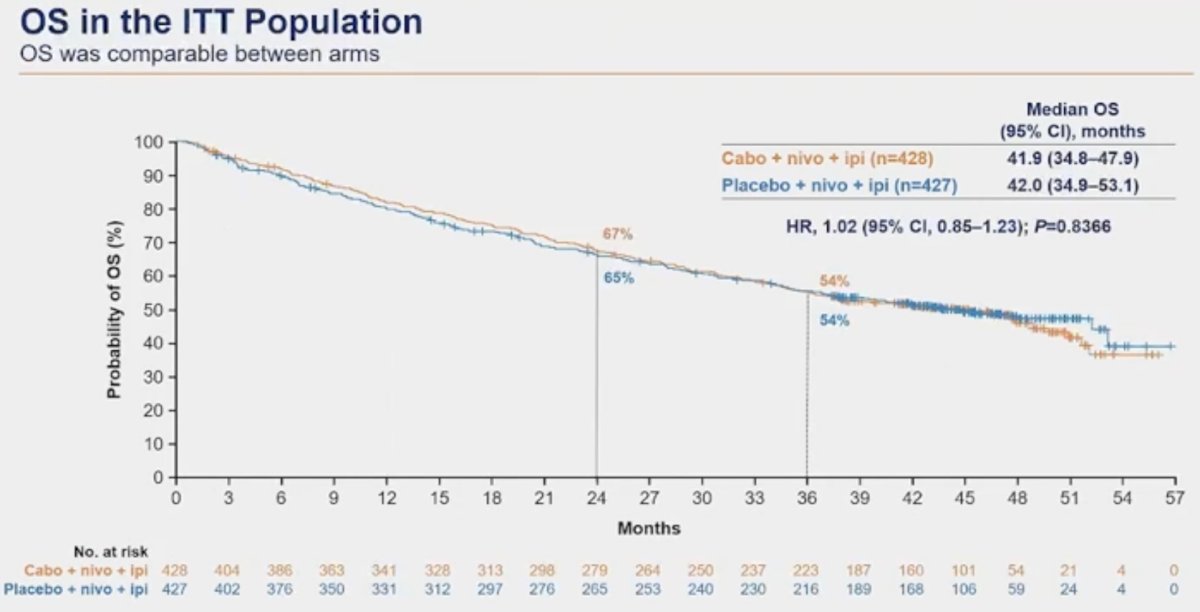
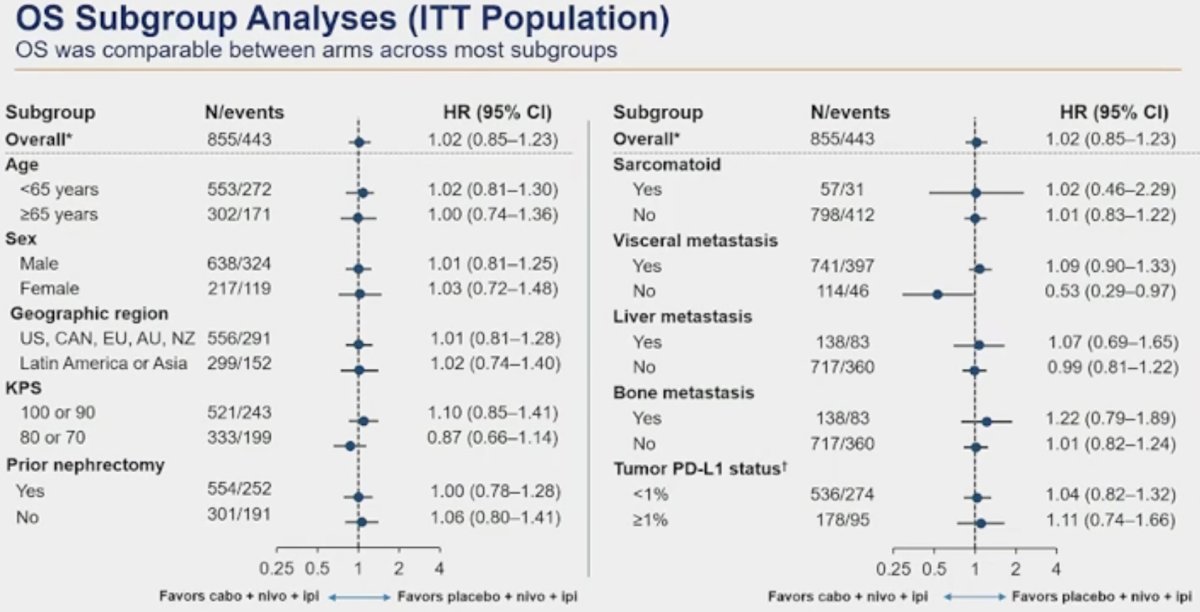
In the overall cohort, there was no overall survival benefit with median survivals of 41.9 and 42 months in the intervention and control arms, respectively (HR: 1.02, 95% CI: 0.85–1.23, p=0.84),
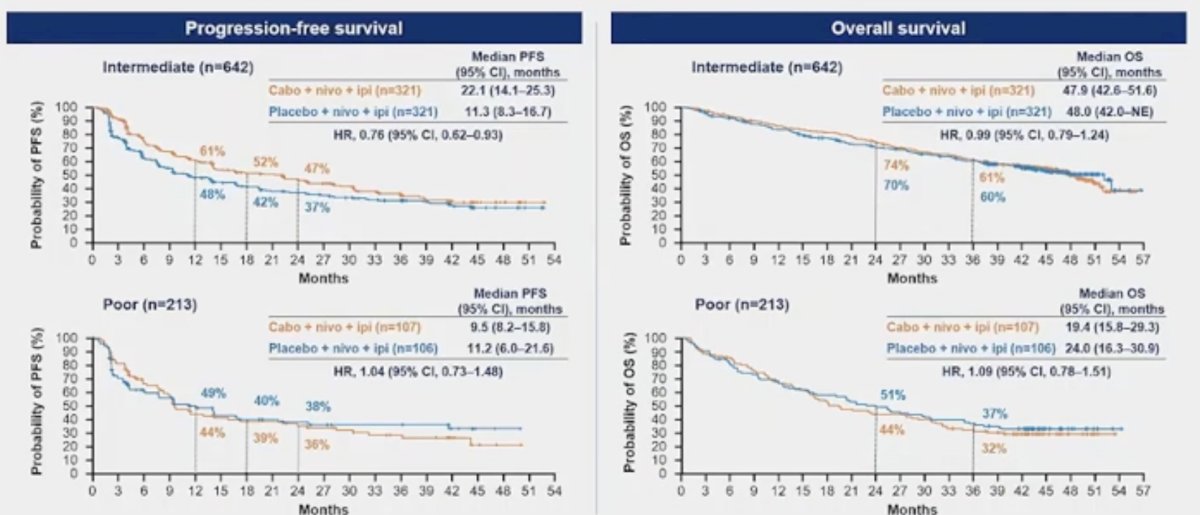
When PFS and OS were stratified by IMDC risk group, Dr. Albiges noted that the PFS benefit was limited to patients with intermediate risk disease only:
- Intermediate risk: 22.1 versus 11.3 months (HR: 0.76, 95% CI: 0.62–0.93)
- Poor risk: 9.5 versus 11.2 months (HR: 1.04, 95% CI: 0.73–1.48)
No OS benefit was observed in either the intermediate or high risk IMDC categories.
Subgroup analyses of OS did not identify any subgroups that may have survival benefits to the addition of cabo to ipi + nivo.
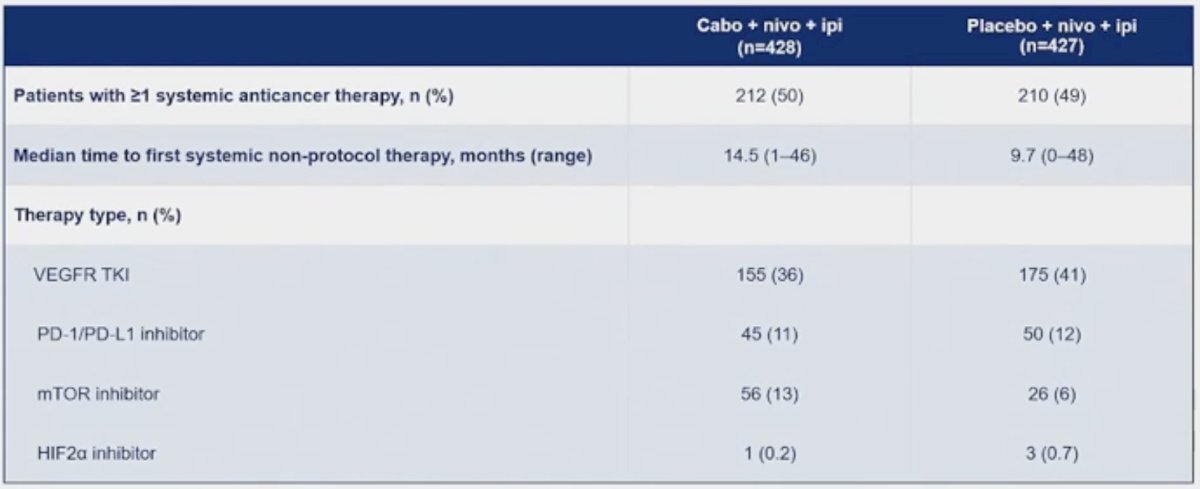
Approximately 50% of patients in both arms proceed to receive ≥1 additional systemic anticancer therapy, at a median of 14.5 and 9.7 months in the cabozantinib and placebo arms, respectively. A VEGFR TKI was the most common next agent in both arms (36–41%), followed by a PD-1/L-1 inhibitor (11–12%).
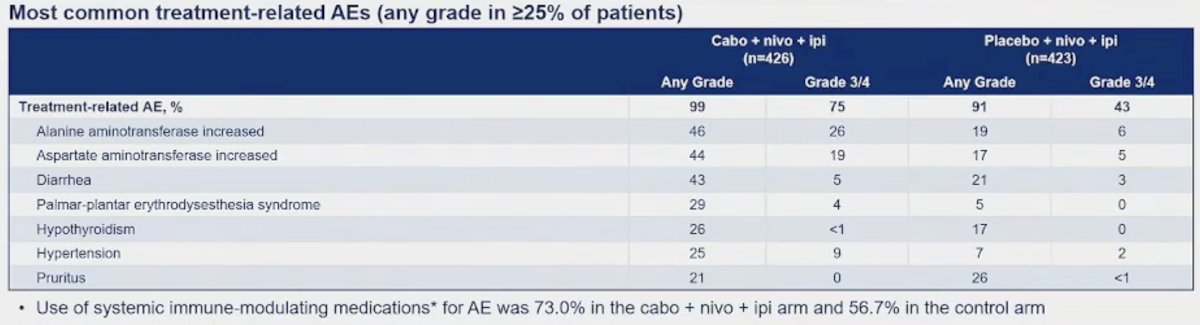
With regard to treatment exposure and adverse events, Dr. Albiges highlighted the following points:
- The median average daily dose of cabozantinib was low (22.4 mg [recommended: 40])
- The recommended 4 cycles of ipilimumab were administered to only 58% of patients
- Treatment-related adverse events leading to discontinuation of ≥1 component occurred in 49% of patients in the cabozantinib arm

AEs related to liver toxicity were the most commonly observed in the cabozantinib group.
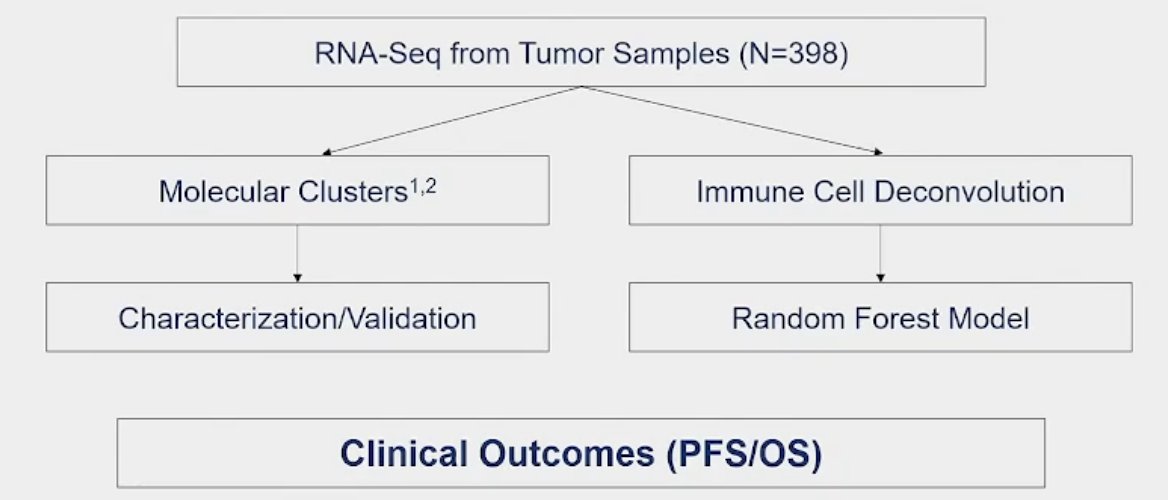
Exploratory biomarker analysis using RNA-seq from tumor samples (n=398) to identify molecular clusters and immune cell deconvolution phenotypes was performed.
Unsupervised transcriptomic analysis revealed seven molecular subsets (illustrated below). The distribution of clusters across IMDC risk groups and transcriptional signatures associated with each cluster were generally consistent with IMmotion 151 and JAVELIN Renal 101.
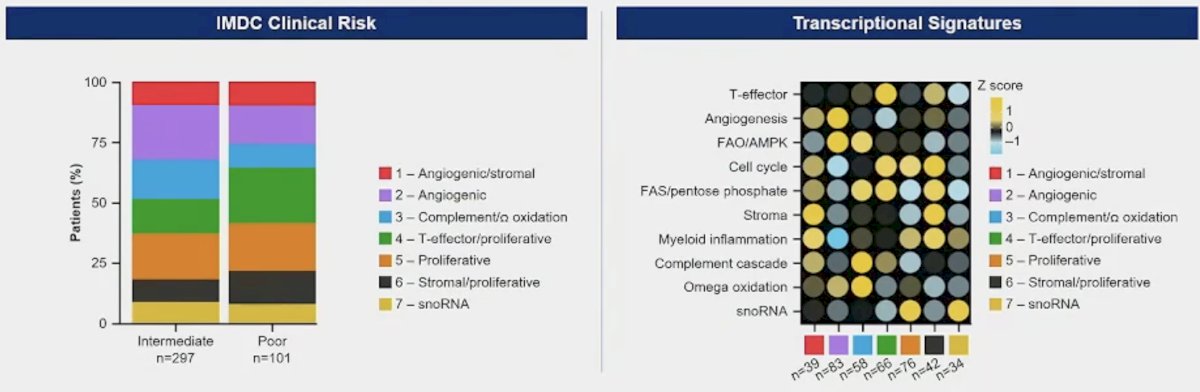
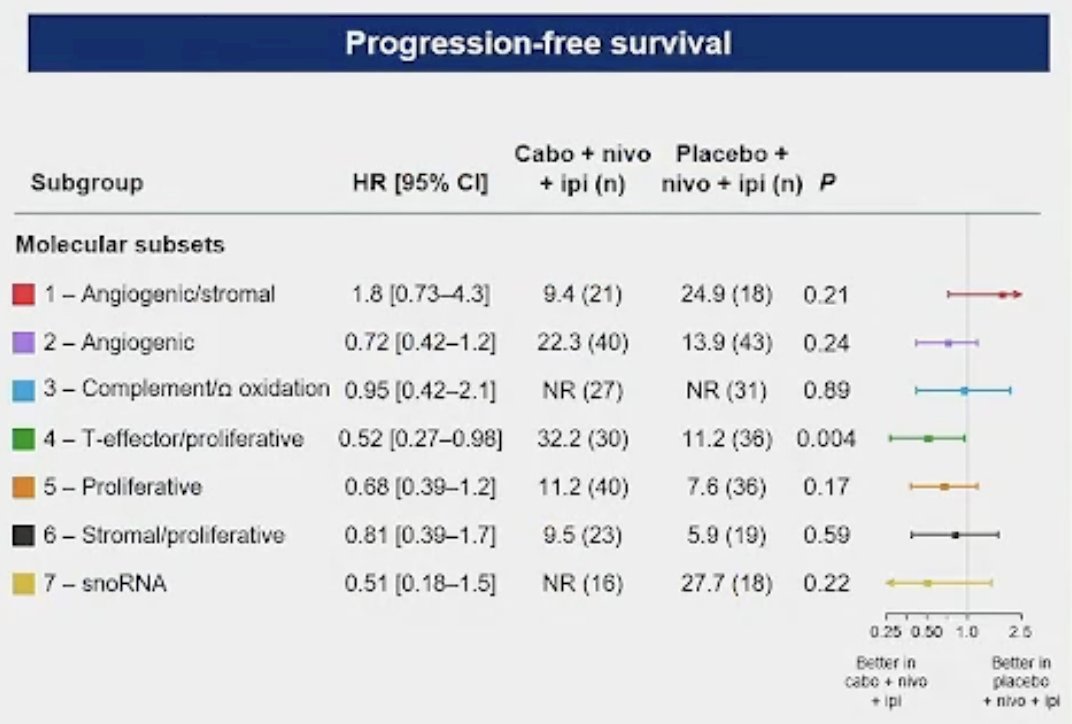
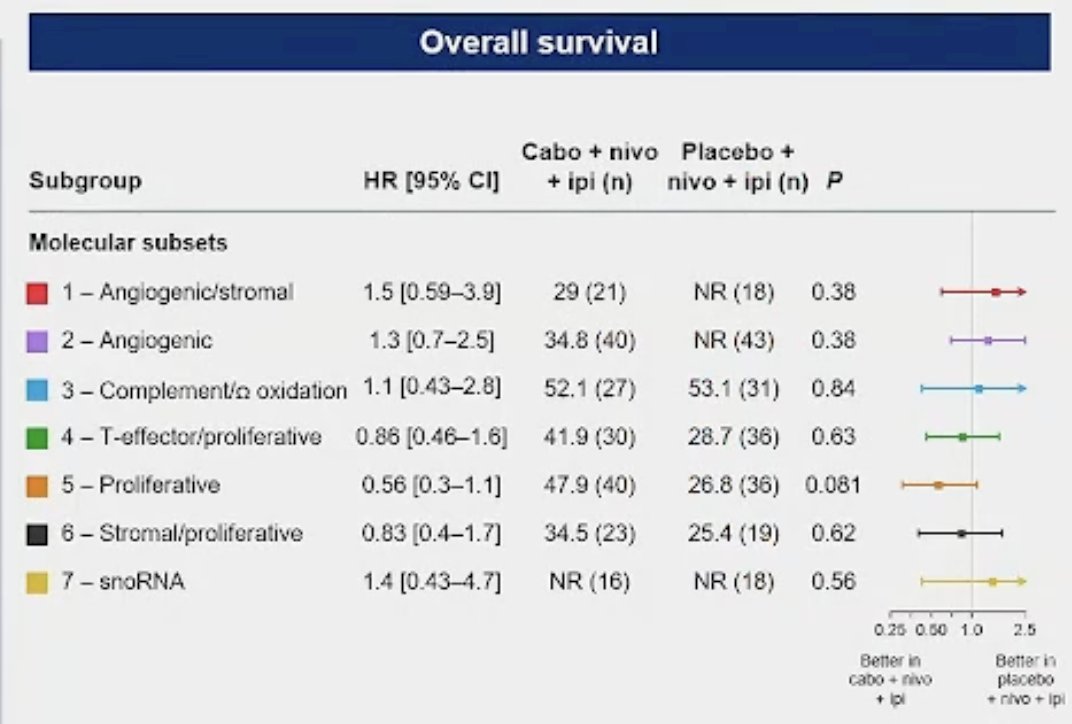
No clear association between molecular clusters and clinical outcomes was observed; however, the sample sizes in each cluster were small.
Deconvolution from RNA-Seq data was used to investigate the effects of cabozantinib on immune cell types. As seen by the green bar in the right panel, the level of M2-like macrophages was the best predictor of overall survival outcomes.
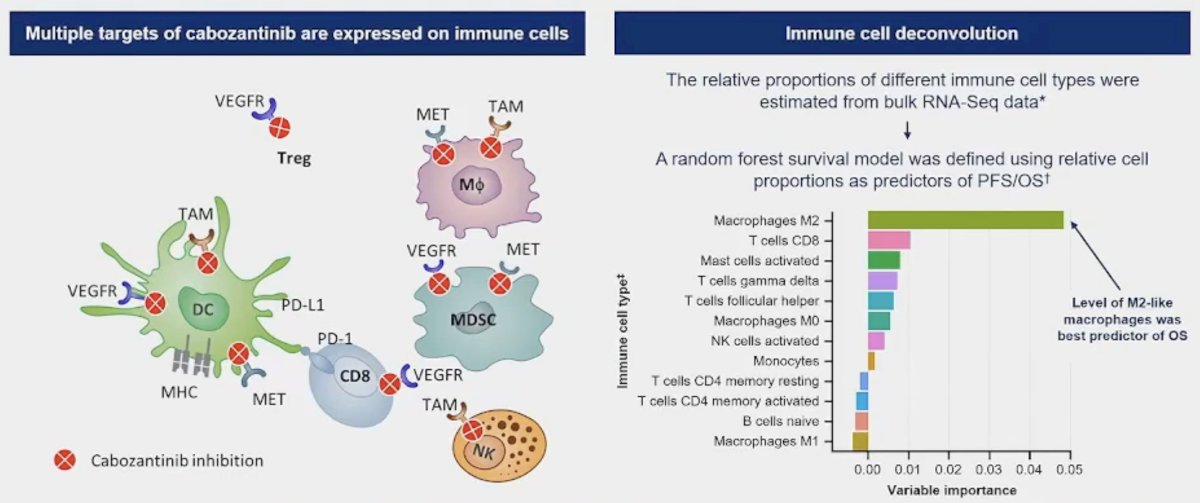
M2-like macrophages contribute to tumor growth, invasion, and metastasis by suppressing the immune response, and have been associated with a poor prognosis in different cancers. Patients with IMDC poor risk disease and those with visceral metastasis exhibited higher levels of
M2-like macrophages
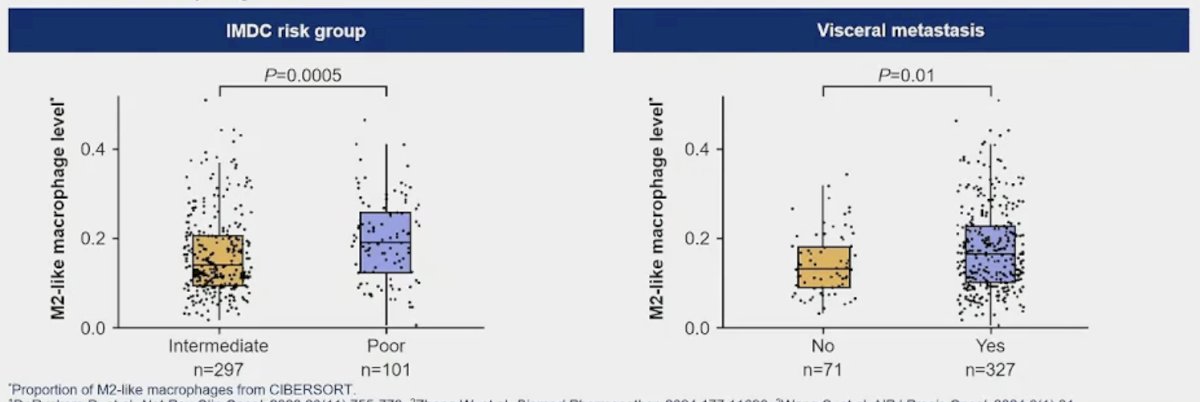
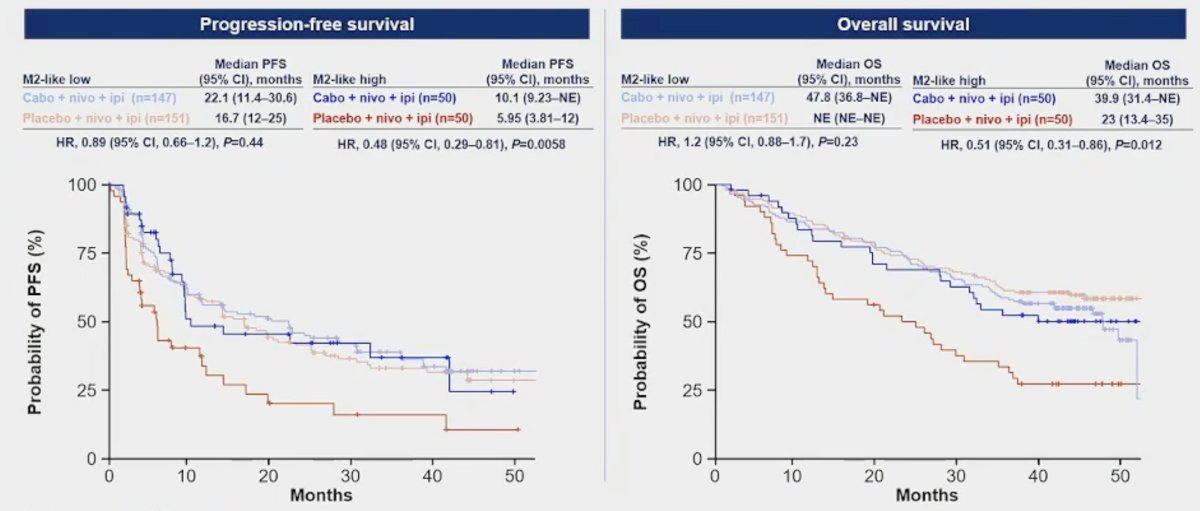
It appears that the addition of cabozantinib to nivo + ipi overcame M2-like macrophage-mediated immune suppression. The red curves below represent patient with M2-like high expression, who received placebo. Both PFS and OS outcomes were worst for this subgroup. Conversely, when cabozantinib was given to these patients (dark blue curves), we see that PFS and OS outcomes were significantly improved – in line with survival outcomes seen in M2-like low subgroups.
Dr. Albiges concluded as follows:
- After 45 months of follow-up, first-line treatment with cabozantinib + nivolumab + ipilimumab continued to demonstrate a PFS benefit over placebo + nivolumab + ipilimumab in patients with aRCC
- There were no significant differences in OS between the two arms in the ITT population or by IMDC risk group
- The safety profile of cabozantinib + nivolumab + ipilimumab was consistent with previously reported results
- There was no clear relationship between previously described molecular clusters and PFS and OS outcomes
- Exploratory immune cell deconvolution and machine learning modeling identified
- The levels of M2-like macrophages are higher in patients with IMDC poor risk disease
- The addition of cabozantinib to nivolumab + ipilimumab may overcome M2-like macrophage-mediated immune suppression
- Preclinical and clinical validation is ongoing
Presented by: Laurence Albiges MD, PhD, Professor, Medical Oncology, Vice-chair of the Department of Cancer Medicine at the Gustave Roussy Institute, Villejuif, France
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
Related content: COSMIC-313 Trial for Advanced Renal Cell Carcinoma - Laurence Albiges
References:
- Choueiri TK, Powles T, Albiges, et al. Cabozantinib plus Nivolumab and Ipilimumab in Renal Cell Carcinoma. N Engl J Med. 2023; 388(19):1767-78.