(UroToday.com) The 2025 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA between February 13th and 15th 2025, was host to the Poster Session C: Renal Cell Cancer; Adrenal, Penile, Testicular and Urethral Cancers. Dr. Daniela Arduini presented the Abstract 551: Updated results of the Tide-A study evaluating avelumab plus intermittent axitinib in previously untreated patients with metastatic renal cell carcinoma (mRCC).
Dr. Arduini highlighted the role of VEGFR-TKI and anti-PD1/PDL1 immunotherapy (IO) combinations as the standard of care for first-line treatment in metastatic renal cell carcinoma (mRCC). The TIDE-A trial previously demonstrated the feasibility of TKI interruption with IO maintenance in patients achieving tumor response to initial TKI+IO combination therapy, successfully meeting its primary endpoint.1 The investigators have now presented updated results with a longer follow-up for median progression-free survival (PFS) and overall survival (OS) in the overall population and in those who interrupted TKI to further assess the durability and outcomes of this treatment strategy.
Patients with confirmed mRCC, prior surgery for the primary tumor, no symptomatic/bulky disease or liver metastases, ECOG 0/1, and measurable disease were enrolled. Treatment consisted of Avelumab 800 mg IV Q2W plus Axitinib 5 mg PO BID for 36 weeks. At week 36, patients who achieved a partial response (PR) interrupted Axitinib and continued Avelumab until disease progression (PD) or unacceptable toxicity. If PD occurred while on Avelumab, Axitinib was restarted and interrupted again upon achieving a new PR. Patients who did not achieve PR at week 36 continued combination therapy until PD. The study design is shown below.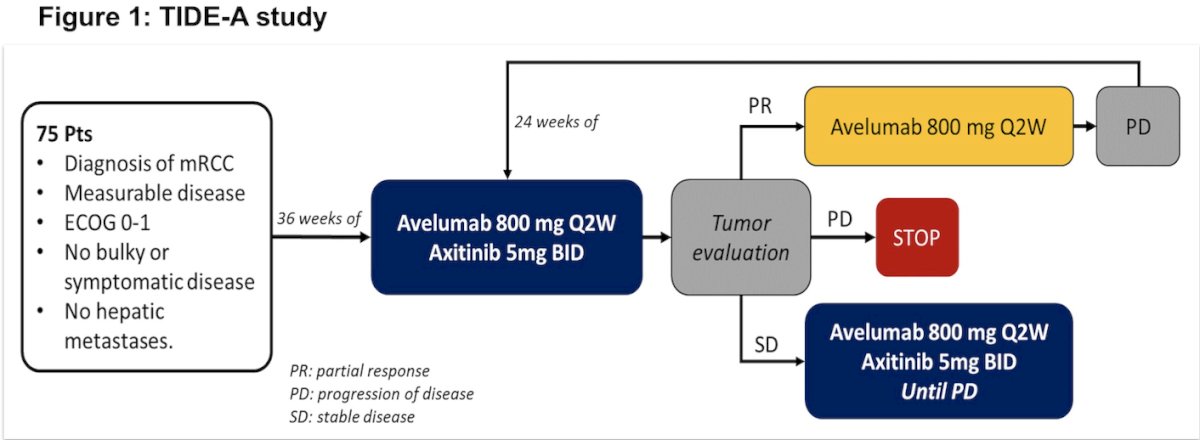
A total of 75 patients were included in the efficacy analysis (40% favorable risk, 60% intermediate/poor risk). As of the April 2024 data cutoff, with a median follow-up of 31.7 months, the median PFS was 27.9 months (95% CI, 23.0–32.8), while the median OS was not reached, with a 24-month OS rate of 85%.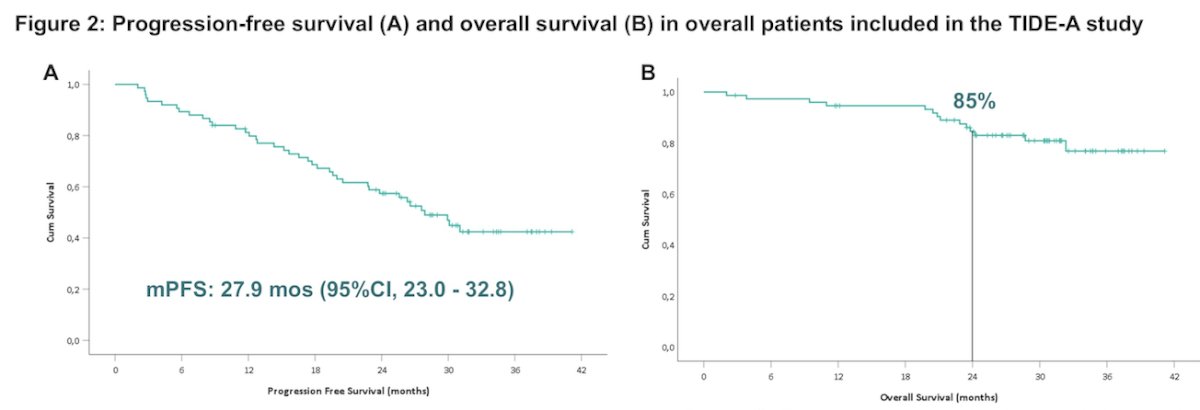
Moreover, among the 29 patients who achieved a response and interrupted axitinib at week 36, the median PFS and the median OS were not reached; while the 24-mos PFS and OS rates were 58% and 82%, respectively.
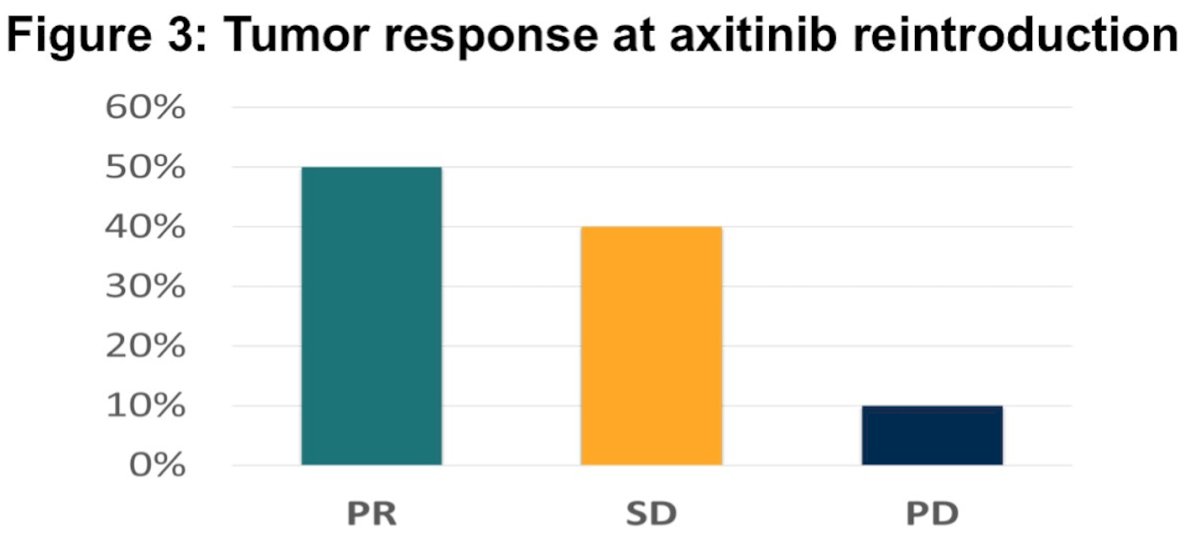
The investigators also evaluated the response to axitinib reintroduction in patients who experienced disease progression while on avelumab maintenance. Among the 21 patients who restarted axitinib, the ORR was 50% (10 partial response, 8 stabel disease, 2 progressive disease), with a median PFS of 17.2 months (95% CI, 11.9–22.5) in this group.
Dr. Arduini concluded with the following key points:
- The TIDE-A trial is the first study demonstrating the feasibility of VEGFR-TKI interruption with immunotherapy maintenance in mRCC patients who achieved a tumor response on combination therapy.
- This updated analysis, with longer follow-up, confirmed the feasibility of VEGFR-TKI interruption and the high response rate upon VEGFR-TKI reintroduction in patients receiving avelumab maintenance.
- This strategy warrants further investigation in a randomized trial.
Presented by: Daniela Arduini, MD, MSc, Medical Oncology at Fondazione Policlinico Universitario Agostino Gemelli IRCCS, Italy.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
Reference: