(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Genitourinary (GU) Annual Symposium held in San Francisco, CA between February 13–15, 2025 was host to a renal cell, adrenal, penile, testicular, and urethral cancers poster session. Dr. Toni Choueiri presented updated results from the phase II LITESPARK-003 study of belzutifan plus cabozantinib in patients with advanced clear cell renal cell carcinoma (ccRCC).
The hypoxia-inducible factor-2α (HIF-2α) inhibitor belzutifan is approved in the United States for the second- or subsequent-line treatment of certain patients with advanced renal cell carcinoma (RCC), and the multikinase inhibitor cabozantinib is approved for the first- or subsequent-line treatment of patients with advanced RCC.1,2
Belzutifan combined with cabozantinib showed antitumor activity in participants with advanced ccRCC who were treatment-naïve (cohort 1) or previously treated (cohort 2) in the phase II LITESPARK-003 study (NCT03634540).3,4 In the initial analysis, the primary end point of objective response rate (ORR) was 57% in cohort 1 (n = 35) and 31% in cohort 2 (n = 52) after a median follow-up of 14 months and 24.6 months, respectively. After a median follow-up of 24.3 months in cohort 1 and 39.8 months in cohort 2, belzutifan plus cabozantinib continued to show durable antitumor activity:5,6
- Cohort 1 (n = 50): ORR, 70%; median duration of response (DOR): 28.6 months
- Cohort 2 (n = 52): ORR, 31%; median DOR: 31.5 months
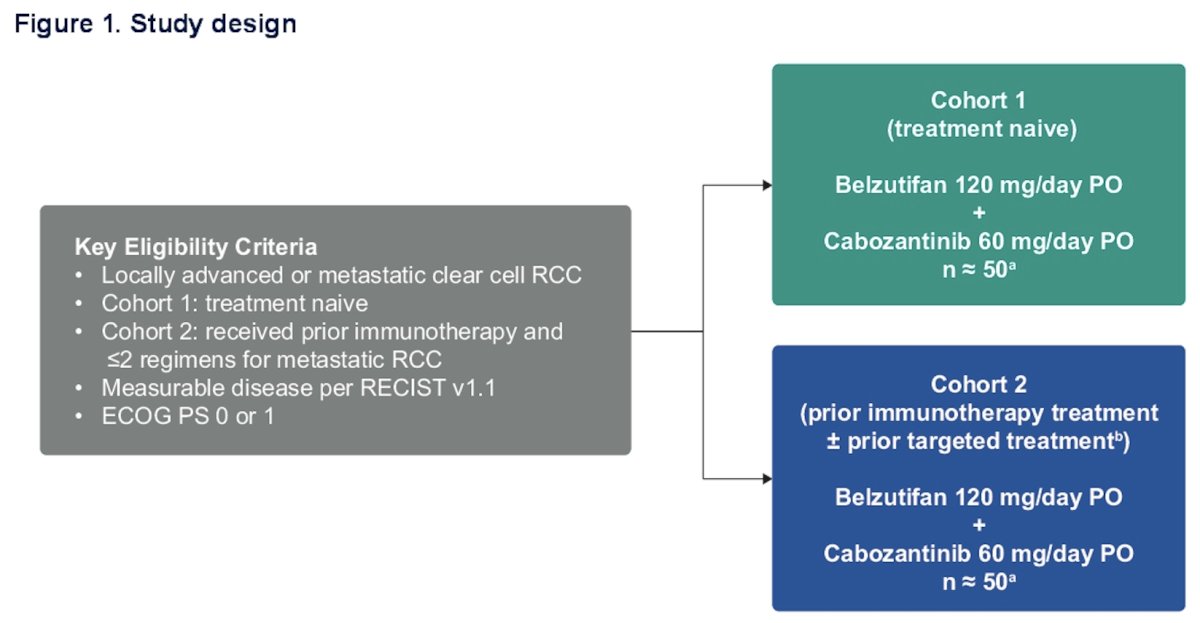
The study design of LITESPARK-003 is illustrated below. In brief, this phase II trial assigned patients with locally advanced or metastatic ccRCC (treatment-naïve or previously treated) to belzutifan 120 mg orally once daily plus cabozantinib 60 mg orally once daily. The primary endpoint was investigator-determined ORR per RECIST v1.1, with secondary outcomes of progression-free survival (PFS), duration of response (DOR), time-to-response (TTR), overall survival (OS), and safety/tolerability.
The OS, PFS, DOR, and associated 95% Cls were estimated using the Kaplan- Meier method. ORR 95% CI was calculated using the Clopper-Pearson method. The severity of adverse events (AEs) was graded per the National Cancer Institute Common Terminology Criteria for Adverse Events. version 5.0. The data cutoff date was March 18, 2024.
The median time from first dose to the data cutoff date was 34.4 months (range: 14.3–58.3) in cohort 1 and 49.9 months (range: 43.2–65.1) in cohort 2.
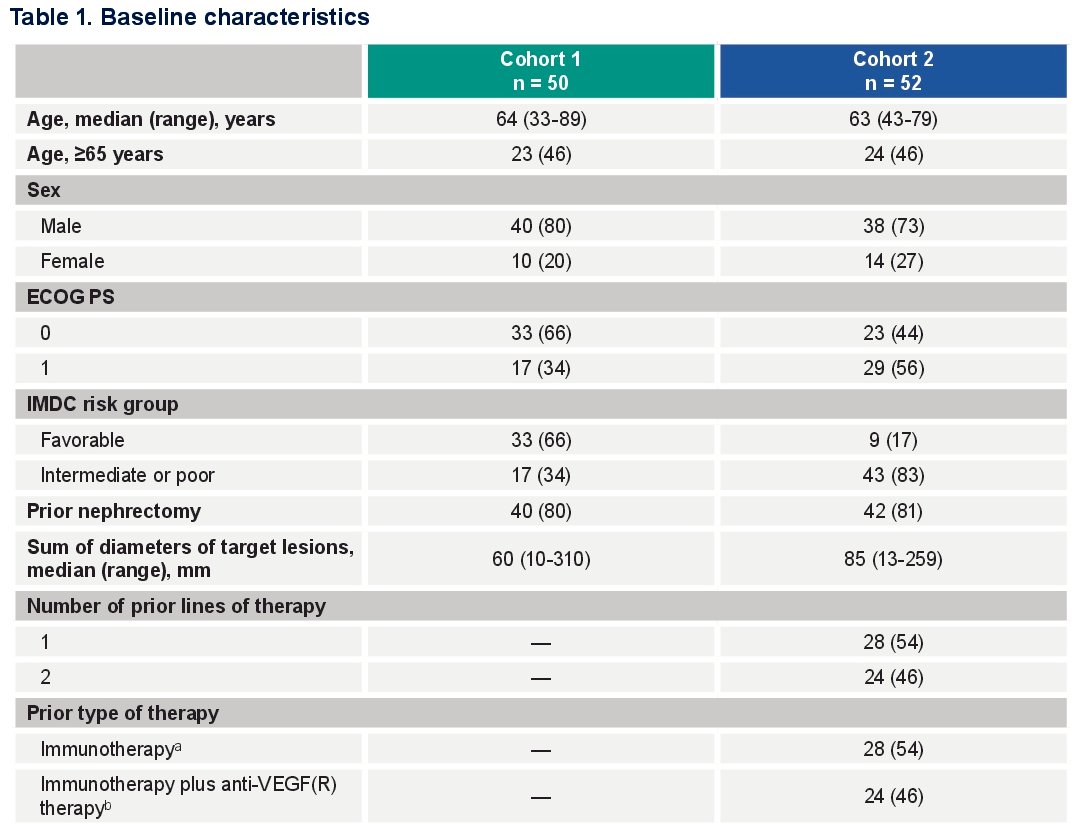
The baseline characteristics are summarized below. The median age was 63–64 years. 83% of patients in Cohort 2 had IMDC intermediate or poor risk disease, versus only 34% in Cohort 1. 80% of patients had a prior nephrectomy. Disease volume was larger in Cohort 2 patients (total sum of target lesions: 85 versus 60 mm). In Cohort 2, 54% had received prior immunotherapy and 46% immunotherapy plus a VEGFR inhibitor.
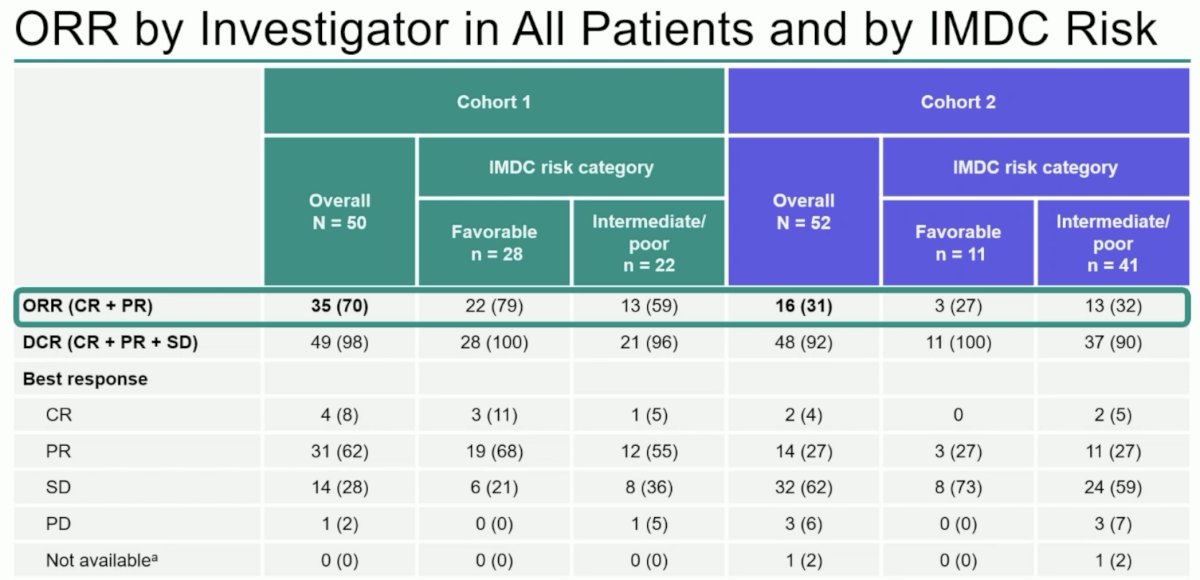
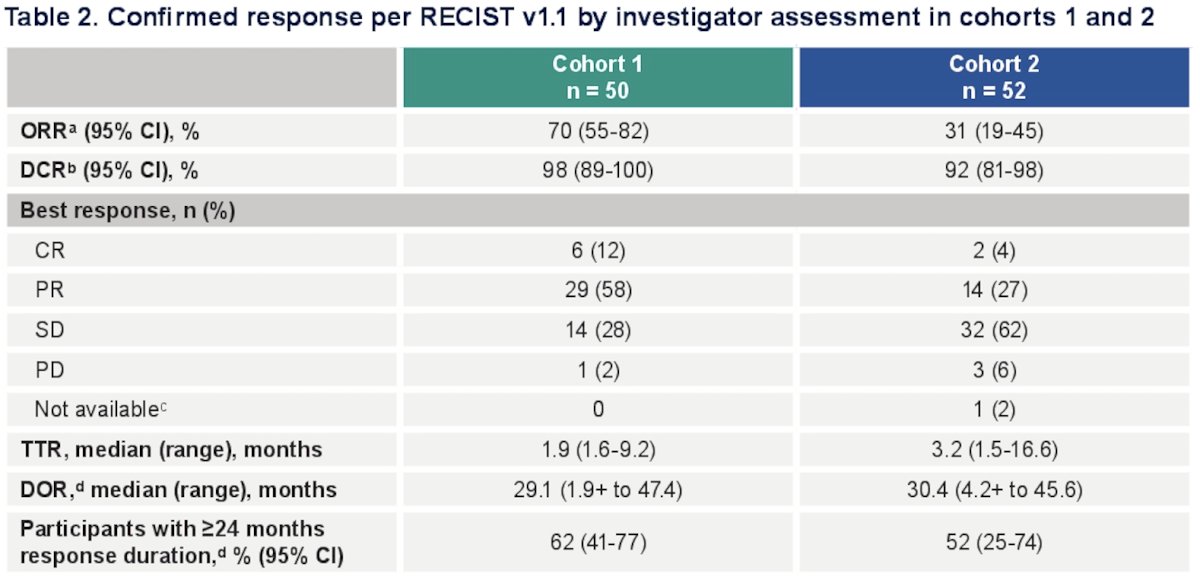
From an efficacy standpoint, the confirmed ORRs in Cohorts 1 and 2 were 70% (CR: 12%, PR: 58%) and 31% (CR: 4%, PR: 27%), respectively. The median time to response was 1.9 and 3.2 months, respectively. The DCR rates were 98% and 92%, respectively. The median durations of response were 29.1 and 30.4 months, respectively.
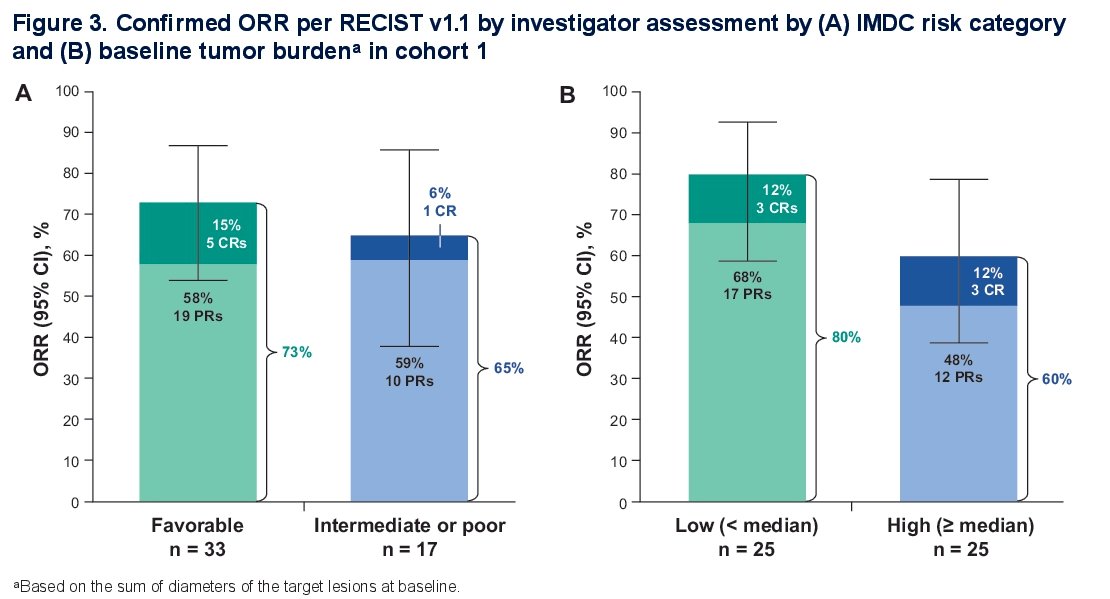
The confirmed ORR by IMDC risk category (left) and baseline tumor burden (right) in Cohort 1 is summarized below. The ORR in favorable risk patients was 73% versus 65% in intermediate or poor risk. In patients with a low tumor burden the ORR was 80% versus 60% in high tumor burden patients.
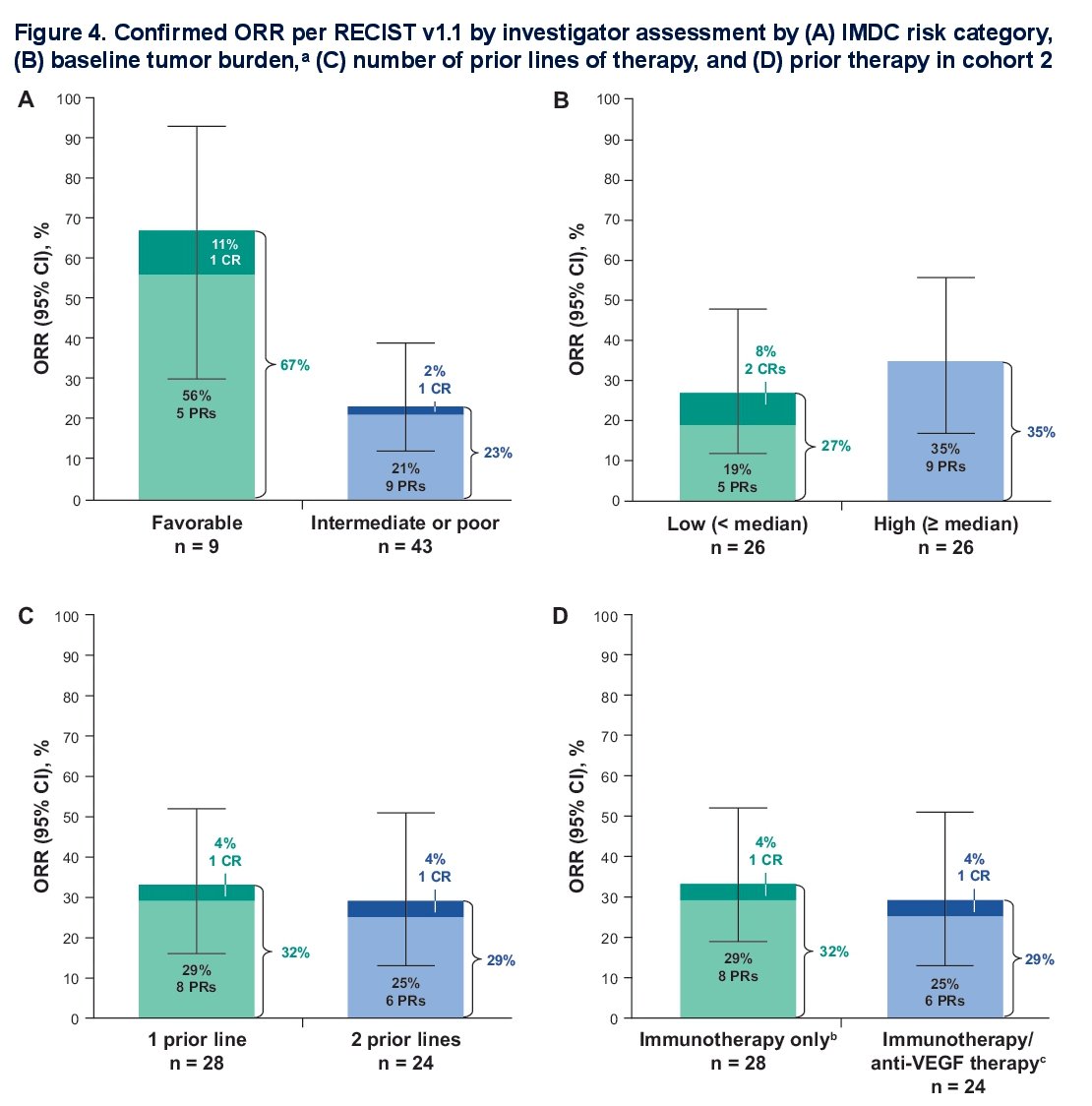
The confirmed ORR by IMDC risk category (upper left), baseline tumor burden (upper right), number of prior lines of therapy (lower left), and prior therapy (lower right) in Cohort 2 is summarized below. The ORR in favorable risk patients was 67% versus 23% in intermediate or poor risk. In patients with a low tumor burden, the ORR was 27% versus 35% in high tumor burden patients. Overall, ORRs were similar irrespective of number of prior lines of therapy (29–32%) or prior therapy received (29–32%).
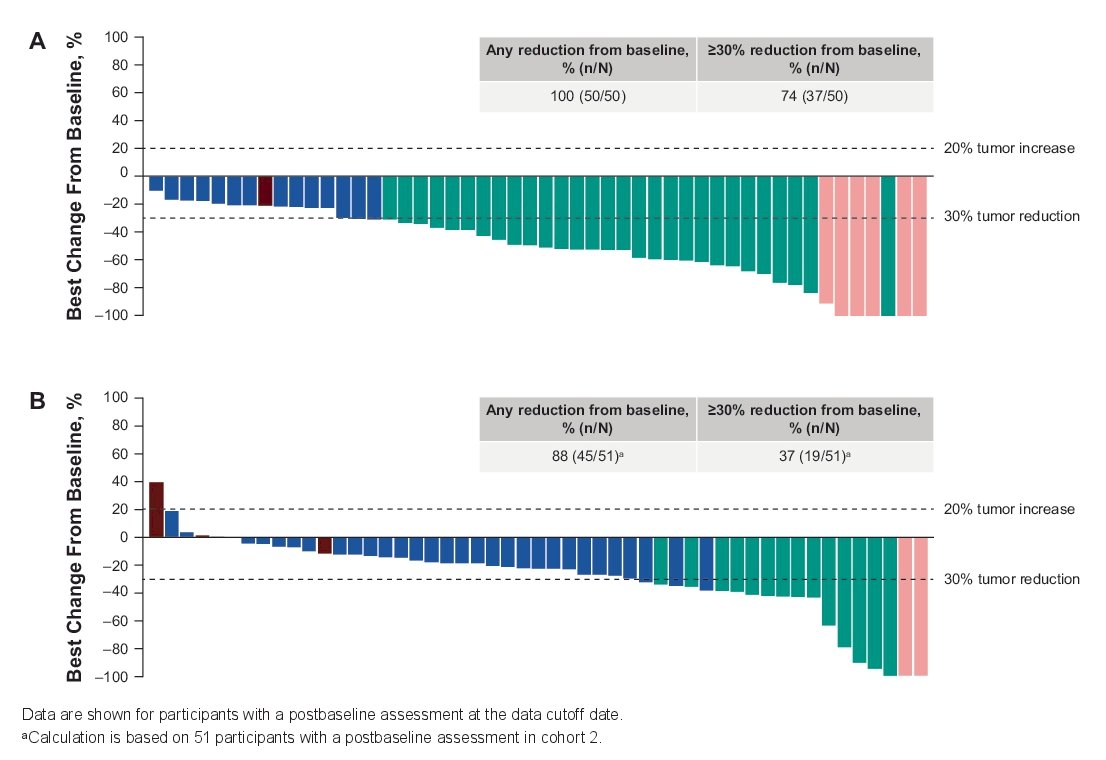
Summarized below is the best percentage change from baseline in target lesion size per RECIST v1.1 by investigator assessment in Cohorts 1 and 2:
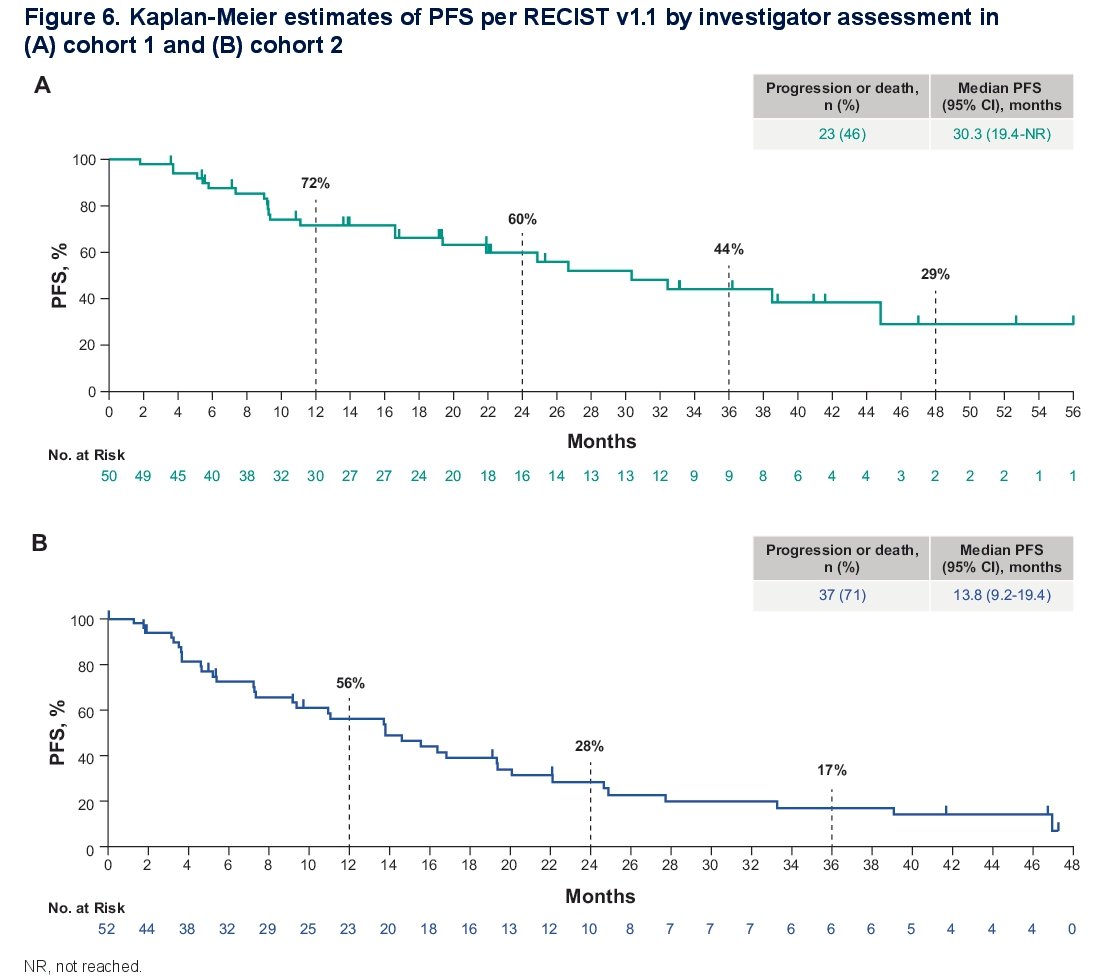
The median PFS in Cohorts 1 and 2 were 30.3 (95% CI: 19.4–NR) and 13.8 (95% CI: 9.2–19.4) months, respectively.
The corresponding overall survival rates were not reached and 26.7 months in Cohorts 1 and 2, respectively.

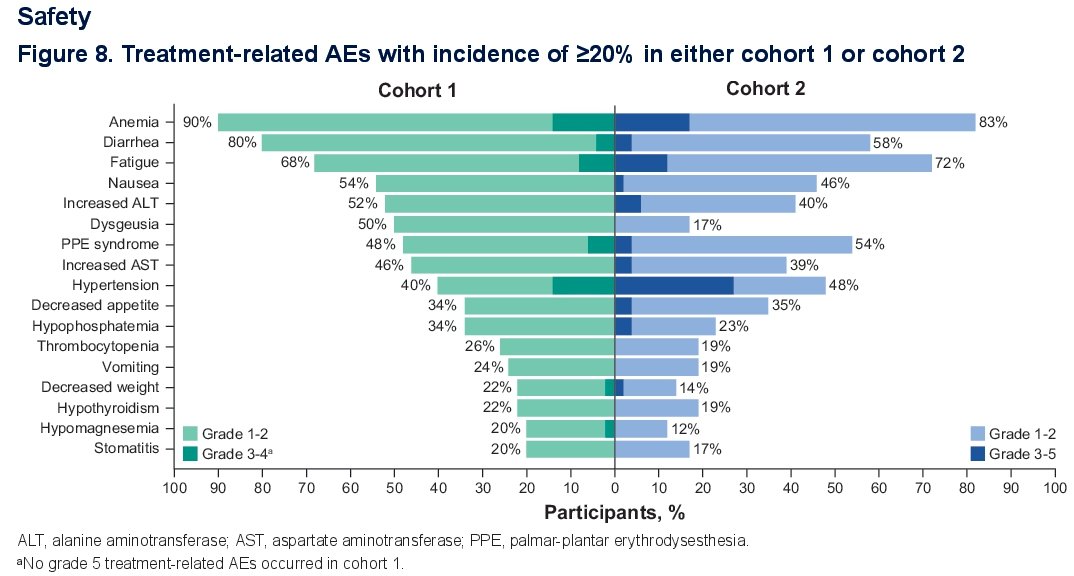
Treatment-related adverse events with incidence ≥20% in either Cohort 1 or 2 are summarized below:
Dr. Choeuiri concluded as follows:
- With updated follow-up, belzutifan plus cabozantinib continued to show durable antitumor activity in both first-line (cohort 1) and subsequent-line (cohort 2) treatment of participants with clear cell RCC
- ORR was consistent across subgroups based on IMDC risk categories, baseline tumor burden, and prior anticancer therapy (cohort 2 only)
- Safety was consistent with prior observations and with the individual profiles of each agent
- These results support further investigation of a HIF-2α inhibitor in combination with a VEG(R) tyrosine kinase inhibitor for advanced clear cell RCC in both first-line and subsequent-line settings
Presented by: Toni K. Choueiri, MD, Jerome and Nancy Kohlberg Professor of Medicine, Dana-Farber Cancer Institute and Harvard Medical School, Boston, MA
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
References:- Welireq™ (belzutifan) tablets, for oral use [package insert]. Rahway, NJ: Merck Sharp & Dohme, LLC; 2023.
- CABOMETYX® (cabozantinib) tablets, for oral use [package insert]. South San Francisco, CA: Exelixis, Inc.; 2023.
- Choueiri TK, Powles T, Burotto M, et al. Lenvatinib plus pembrolizumab for advanced renal cell carcinoma. Ann Oncol 2022;33(12):1204.
- Choueiri TK, Motzer RJ, Powles T, et al. Lenvatinib plus pembrolizumab versus sunitinib for advanced renal cell carcinoma: extended follow-up from the CLEAR study. Lancet Oncol 2023;24(5):553-562.
- Choueiri TK, et al. Belzutifan plus cabozantinib as first-line treatment for patients with advanced clear-cell renal cell carcinoma (LITESPARK-003): an open-label, single-arm, phase 2 study. Lancet Oncol 2025;26(1):64-73.
- Choueiri TK, et al. Phase II LITESPARK-003 study of belzutifan in combination with cabozantinib for advanced clear cell renal cell carcinoma (ccRCC). Ann Oncol 2023;34(Suppl 1):S1328-S1329.