(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Genitourinary (GU) Annual Symposium held in San Francisco, CA between February 13–15, 2025 was host to a renal cell and testicular cancers oral abstract session. Dr. Axel Heidenreich presented the final results of the COTRIMS (Cologne trial of retroperitoneal lymphadenectomy in metastatic seminoma) trial.
Clinical stage (CS) IIA/B seminoma accounts for only 10–15% of seminomas.
For such patients, current guidelines recommend either:
- Radiotherapy with 30 Gy (IIA) or 36 Gy (IIB)
- Bleomycin + etoposide + cisplatin (BEP) x 3 cycles or etoposide + cisplatin (EP x 4 cycles)
The 5-year survival of seminoma patients, irrespective of stage of disease, remains excellent overall. This is particularly true for stage I patients, who have a 5-year overall survival rate of 99%, despite ~15% experiencing disease relapse without adjuvant therapy, of which 95% recur in the retroperitoneum. Dr. Heidenreich noted that, overall, ~20% of patients with CS I-II seminoma have disease confined to the retroperitoneum. This provides a rationale for performing a retroperitoneal lymph node dissection (RPLND) in such patients.
Another rationale for performing an RPLND in such patients is that current guideline-recommended treatment options are associated with significant long-term toxicity, which becomes especially relevant with long-term (>15 years) follow-up.1,2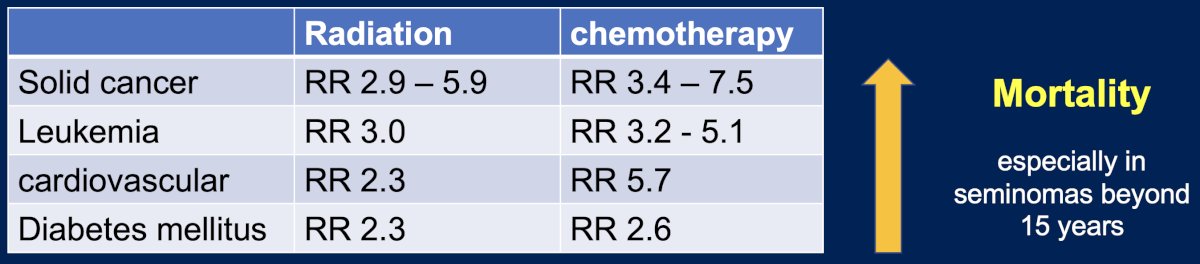
The prospective single arm, single center COTRIMS trial evaluated the efficacy and safety of unilateral, modified template, nerve sparing RPLND in CS IIA/B seminomas.3 Patients were not recommended for adjuvant systemic therapy following their RPLND and underwent guideline-recommended follow-up in accordance with the EAU guidelines. If disease relapse occurred, they were recommended for 3–4 cycles of BEP, based on the underlying IGCCCG classification.
Eligibility criteria were as follows:
- Pure testicular seminomas
- Negative AFP and beta-HCG levels, with lactate dehydrogenase levels <1.5-fold the upper limit of normal.
- CS II A/B disease at presentation or progression during active surveillance
- No prior adjuvant carboplatin permitted
In equivocal cases, a repeat CT scan was performed 6–8 weeks later. Circulating miR371 testing was performed to predict retroperitoneal specimen histology.
The study outcomes were as follows:
- Feasibility
- Oncologic outcomes
- Progression-free survival (primary outcome)
- Overall survival
- Functional outcomes: presence/absence of antegrade ejaculation
- Complications
- Using Clavien-Dindo classification
The primary outcome was 2-year progression-free survival rates with an H0 of ≤20%. The statistical plan is summarized below: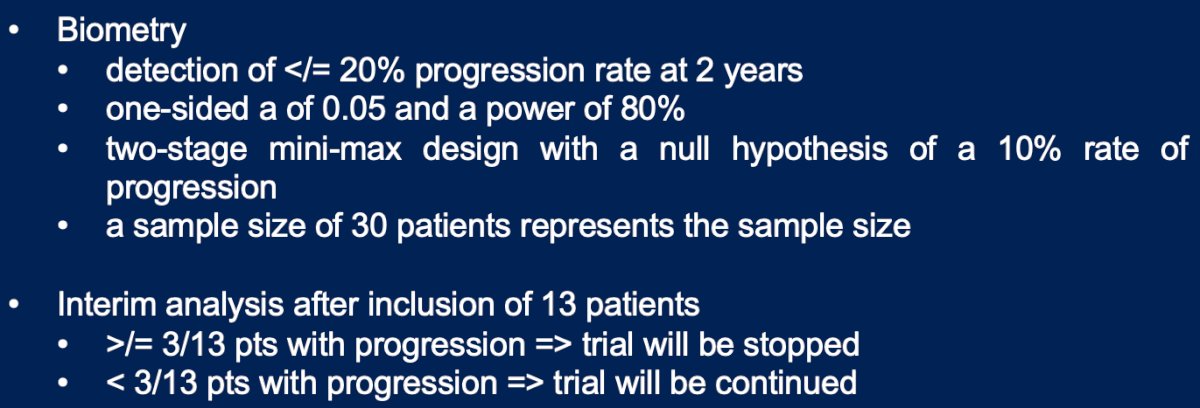
The baseline cohort characteristics are summarized below (n=34). Almost half of patients (47%) had CS I disease at presentation (i.e., progressed during surveillance). At the time of RPLND, 65% had CS IIA disease, with the remaining 35% having CS IIB disease. The median number of lymph nodes detected on pre-operative CT axial imaging was 1.6, with a median nodal size of 2.2 cm.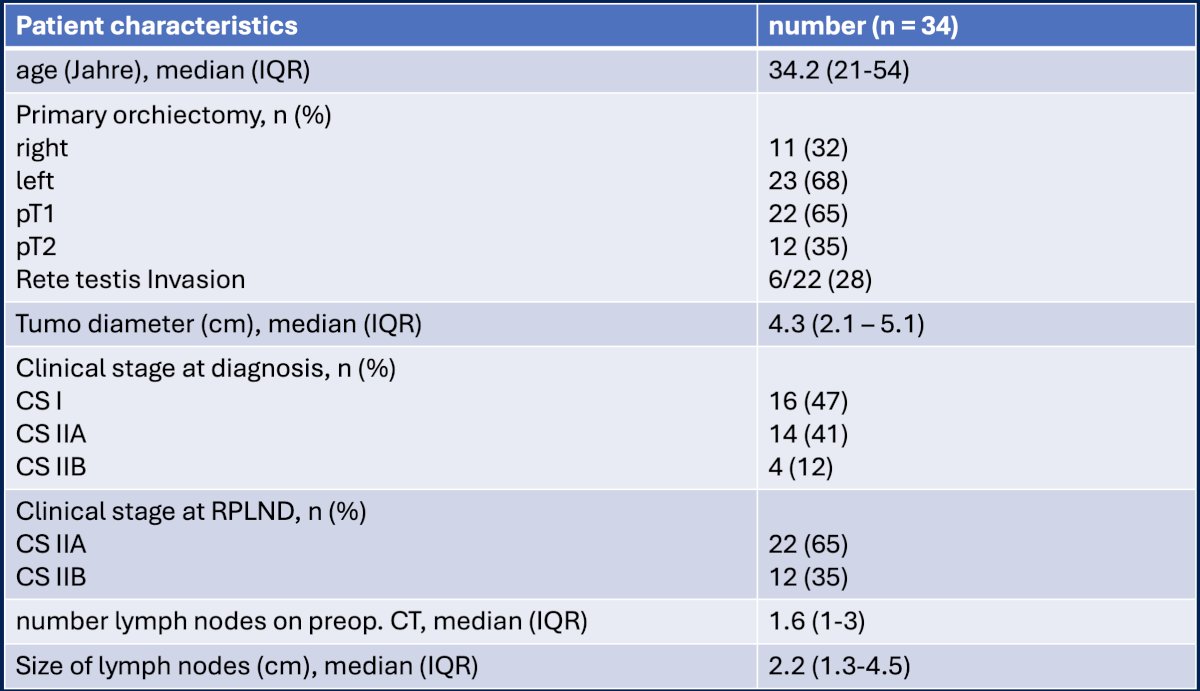
Of the 34 patients, 31 (91%) underwent an open approach, with 3 (9%) undergoing a robotic RPLND. Antegrade ejaculation was preserved in 88% of patients. Grade 3–4 complications were observed in 4 (12%) patients (lymphocele, chylous ascites, paralytic ileus).
The pre-operative distribution of retroperitoneal lymph nodes is as follows:
The median lymph node yield was 19 (range: 7–57). The median number of positive lymph nodes was 1.4, and the median diameter of the positive nodes was 2.3 cm. The pathologic features of the resected nodes were as follows:
- Seminoma: 29 (85%)
- Extracapsular extension: 8 (28%)
- No malignant tissue: 3 (9%)
- Embryonal carcinoma: 2 (6%)
Histology revealed metastatic testicular germ cell tumors in 22/24 patients (92%), with positive miR371a findings for 20 of these 22 patients with metastases (91%). Histology revealed no malignancy in one patient and lymphoma in another, both of whom had negative miR371a findings. One additional patient with pure teratoma and another with a microscopic seminomatous lymph node metastases had false-negative miR371a findings. The miR371 assay had sensitivity of 91% and specificity of 50%. The positive predictive value was 100% and the negative predictive value was 75%.3.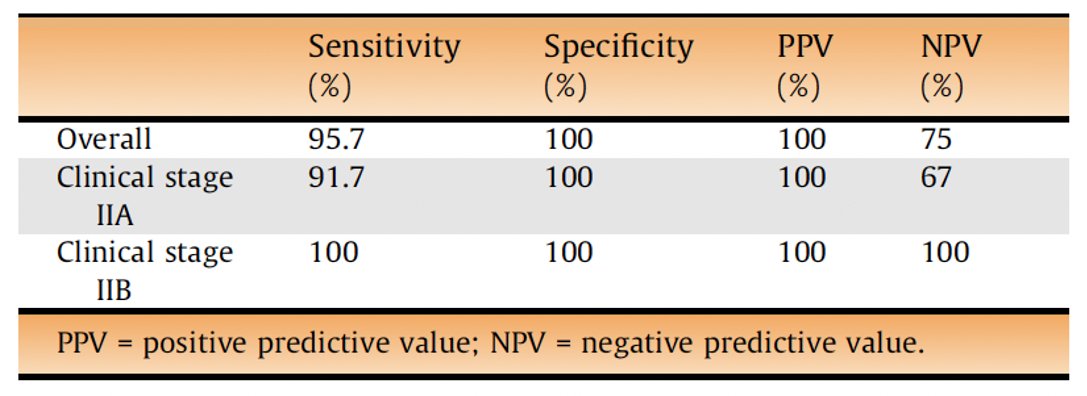
At a median follow-up of 43.2 months, the overall survival was 100%. The treatment-free survival rate was 99.3%, with 4 relapses observed. Of these 4 patients, 3 received BEP and remained free of disease recurrence. One underwent a repeat RPLND and remained disease-free at the last available follow-up.
The locations of the observed relapses were:
- Pulmonary
- Mediastinal
- Pelvic (contralateral)
- Para-aortic (contralateral)
Dr. Heidenreich noted that in comparison to other trials/series of primary RPLND in CS II seminoma patients, the recurrence-free survival rates compared favorably.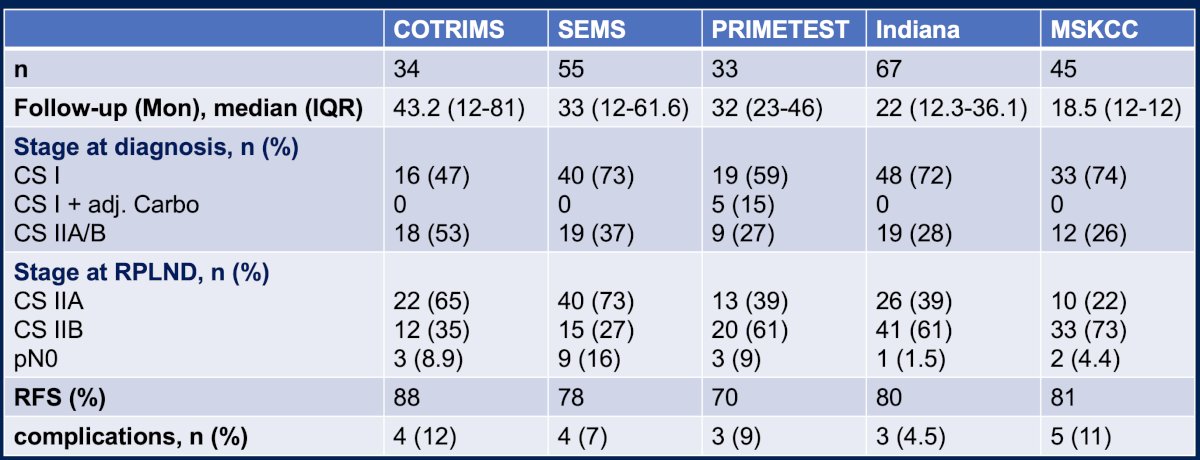
Why were the relapse rates lower in COTRIMS, compared to these other trials/series? Dr. Heidenreich noted that possible reasons may include:
- Favorable patient cohort selection
- 80% had CS IIA disease or low-volume CS IIB
- Template performed
- Retrocaval and retro-aortic nodes dissected
- Common iliac artery node packets down to the iliac bifurcation were purposely harvested
- Template extended lateral to the ureters
- The ipsilateral testicular vein and vasa deferentia were resected
Dr. Heidenreich concluded as follows:
- Nerve-sparing primary RPLND for patients with marker-negative, CS IIA/B seminomas is:
- Feasible, with a low frequency of operative morbidity
- Associated with excellent oncologic outcomes
- Avoids unnecessary chemotherapy/radiation therapy in 10–15% of cases
- Avoids overtreatment in 80% of patients
- Due to the relative rarity of CS IIA/B seminomas These surgeries should be centralized to experienced, high-volume, centers of excellence
- This approach is now recommended by the AUA and SWENOTECA guidelines
- miR371 has high predictive accuracy in this setting
Presented by: Axel Heidenreich, MD, PhD, Professor of Urology, University Hospital Cologne, Cologne, Germany
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
References:- Fung C, Dinh PC, Fossa SD, Travis LB. Testicular Cancer Survivorship. J Natl Compr Canc Netw. 2019; 17(12): 1557-68.
- Kvammen O, Myklebust TA, Solberg A, et al. Long-term Relative Survival after Diagnosis of Testicular Germ Cell Tumor. Cancer Epidemiol Biomarkers Prev. 2016; 25(5): 773-9.
- Heidenreich A, Paffenholz P, Hartmann F, Seelemeyer F, Pfister D. Retroperitoneal Lymph Node Dissection in Clinical Stage IIA/B Metastatic Seminoma: Results of the COlogne Trial of Retroperitoneal Lymphadenectomy In Metastatic Seminoma (COTRIMS). Eur Urol Oncol. 2024; 7(1): 122-7.
- Seelemeyer F, Pfister D, Pappesch R, et al. Evaluation of a miRNA-371a-3p Assay for Predicting Final Histopathology in Patients Undergoing Primary Nerve-sparing Retroperitoneal Lymphadenectomy for Stage IIA/B Seminoma or Nonseminoma. Eur Urol Oncol. 2024; 7(3): 319-22.