(UroToday.com) The 2025 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA between February 13th and 15th 2025, was host to the Trials in Progress Poster Session C: Renal Cell Cancer; Adrenal, Penile, Testicular and Urethral Cancers. Dr. Robert Motzer presented the trial in progress poster 610: INTerpath-004: A phase 2, randomized, double-blind study of adjuvant pembrolizumab (pembro) with V940 (mRNA-4157) or placebo for renal cell carcinoma (RCC).
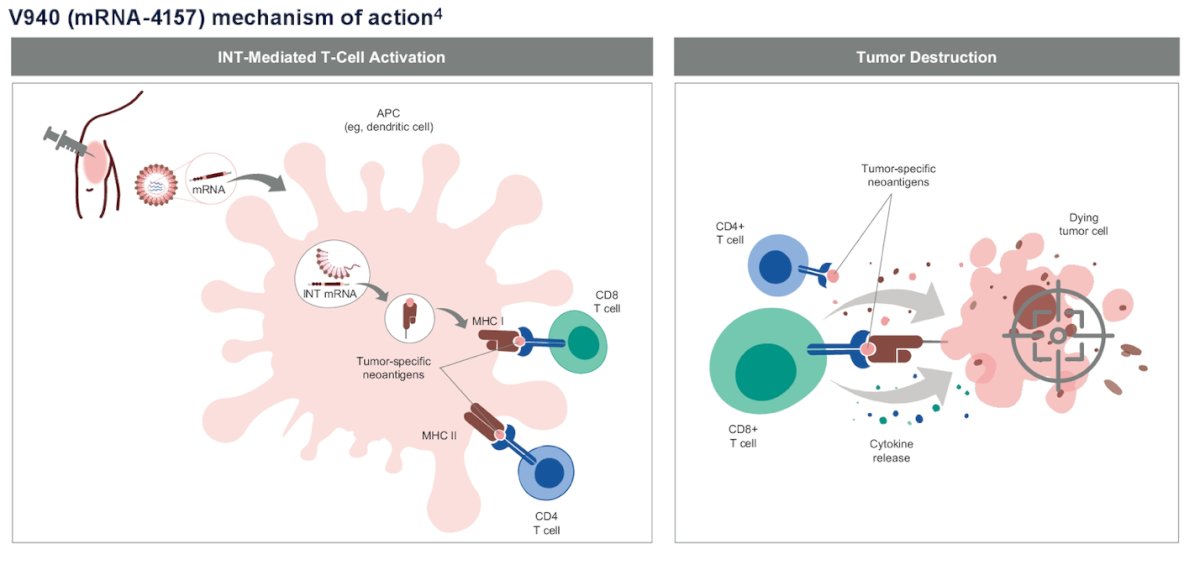
Based on the phase 3 KEYNOTE-564 trial pembrolizumab a PD-1 inhibitor is approved for the adjuvant treatment of patients with renal cell carcinoma (RCC) at increased risk of recurrence following nephrectomy, with or without resection of metastatic lesions. 1 V940 (mRNA-4157) is an individualized neoantigen therapy designed to enhance the antitumor activity of T cells and improve pembrolizumab efficacy. It is developed from the patient’s unique tumor-specific mutational profile. These neoantigens arise from cancer-specific mutations, which are recognized as foreign by the immune system and stimulate robust T cell responses. 2 The mechanism of action is illustrated below:
Targeting neoantigens has shown potential in eliciting antitumor activity across various tumor types, including melanoma. In the phase 2 KEYNOTE-942 study, adjuvant pembrolizumab combined with V940 (mRNA-4157) demonstrated a manageable safety profile and a clinically meaningful improvement in recurrence-free survival after a median follow-up of 34.6 months, compared with adjuvant pembrolizumab monotherapy, in patients with completely resected high-risk melanoma.3
INTerpath-004 (NCT06307431) is a global, multicenter, randomized, double-blind, phase 2 trial designed to evaluate the efficacy and safety or adjuvant V940 plus pembrolizumab or placebo in participants with RCC who have undergone nephrectomy.
Eligible patients are adults with histologically or cytologically confirmed RCC with clear cell or papillary histology (intermediate-high risk [pT2 Gr4, N0, M0 or pT3 Gr3/4, N0, M0], high risk [pT4, N0, M0 or pT any stage, N1, M0], or M1 NED [solid, isolated, soft tissue metastases that can be completely resected at the time of nephrectomy or ≤2 years from nephrectomy]) with or without sarcomatoid features. Patients must have undergone nephrectomy and/or metastasectomy ≤12 weeks prior to randomization and be tumor-free as assessed by investigator. Patients must not have received prior systemic therapy ≤4 weeks or radiotherapy ≤2 weeks prior to randomization. Key inclusion and exclusion criteria are summarized below.

A total of 272 patients will be randomly assigned in a 1:1 ratio to receive pembrolizumab (400 mg IV every 6 weeks for up to 9 cycles) in combination with either V940 (1 mg IM every 3 weeks for up to 9 doses) or placebo. Treatment will continue until unacceptable toxicity, disease recurrence, patient withdrawal, or an investigator’s decision. Randomization will be stratified by histology (clear cell vs. papillary) and disease risk (intermediate-high, high, or M1 NED).
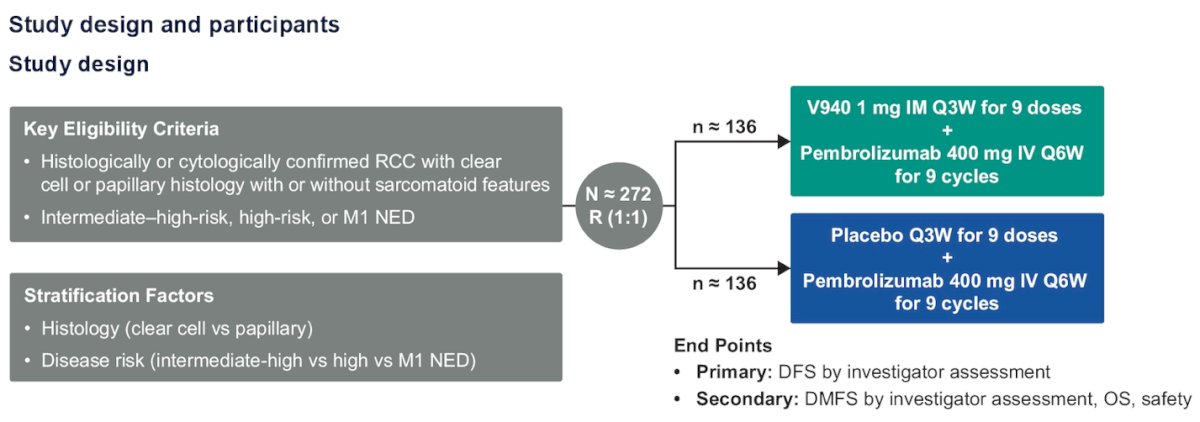
The primary endpoint is disease-free survival by investigator assessment. And key Secondary endpoints include distant metastasis-free survival, overall survival, and safety parameters, including adverse events (AEs), laboratory test results, and vital signs.
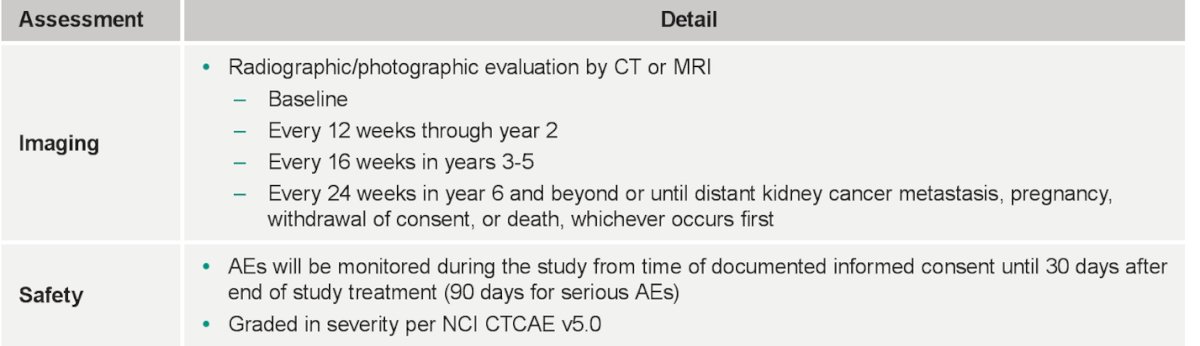
Safety and efficacy analysis are described in detailed below:

Imaging assessments, including CT or MRI, will be conducted every 12 weeks through year 2, every 16 weeks in years 3-5, and every 24 weeks from year 6 onward to monitor disease status. Adverse events (AEs) will be tracked from the time of documented informed consent until 30 days after the end of treatment, with serious AEs monitored for up to 90 days.
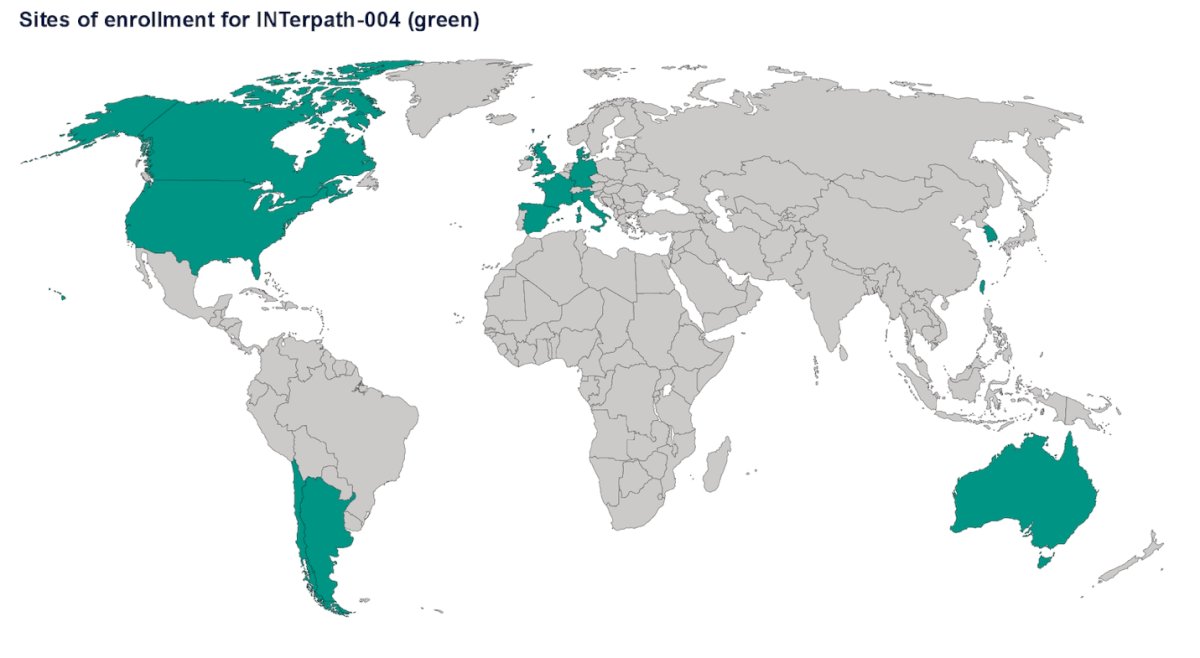
The sites of enrollment are reported below, and the study is currently active.
Presented by: Robert Motzer, MD, Genitourinary Medical Oncologist. Head of Section, Kidney Cancer, Genitourinary Oncology Service, Jack and Dorothy Byrne Chair of Clinical Oncology at Memorial Sloan Kettering Cancer Center (MSKCC). New York, NY, United States.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
References:- Choueiri TK, Tomczak P, Park SH, Venugopal B, Ferguson T, Symeonides SN, Hajek J, Chang YH, Lee JL, Sarwar N, Haas NB, Gurney H, Sawrycki P, Mahave M, Gross-Goupil M, Zhang T, Burke JM, Doshi G, Melichar B, Kopyltsov E, Alva A, Oudard S, Topart D, Hammers H, Kitamura H, McDermott DF, Silva A, Winquist E, Cornell J, Elfiky A, Burgents JE, Perini RF, Powles T; KEYNOTE-564 Investigators. Overall Survival with Adjuvant Pembrolizumab in Renal-Cell Carcinoma. N Engl J Med. 2024 Apr 18;390(15):1359-1371. doi: 10.1056/NEJMoa2312695. PMID: 38631003.
- Wirth TC, Kühnel F. Neoantigen Targeting-Dawn of a New Era in Cancer Immunotherapy? Front Immunol. 2017 Dec 19;8:1848. doi: 10.3389/fimmu.2017.01848. PMID: 29312332; PMCID: PMC5742119.
- Weber JS, Carlino MS, Khattak A, Meniawy T, Ansstas G, Taylor MH, Kim KB, McKean M, Long GV, Sullivan RJ, Faries M, Tran TT, Cowey CL, Pecora A, Shaheen M, Segar J, Medina T, Atkinson V, Gibney GT, Luke JJ, Thomas S, Buchbinder EI, Healy JA, Huang M, Morrissey M, Feldman I, Sehgal V, Robert-Tissot C, Hou P, Zhu L, Brown M, Aanur P, Meehan RS, Zaks T. Individualised neoantigen therapy mRNA-4157 (V940) plus pembrolizumab versus pembrolizumab monotherapy in resected melanoma (KEYNOTE-942): a randomised, phase 2b study. Lancet. 2024 Feb 17;403(10427):632-644. doi: 10.1016/S0140-6736(23)02268-7. Epub 2024 Jan 18. PMID: 38246194.