(UroToday.com) The 2025 GU ASCO annual meeting featured a kidney cancer session and a presentation by Dr. Fady Ghali discussing a simulation study of modeling survival outcomes of KEYNOTE-564 with standard of care control arm treatment. Many trials use non standard of care control arms, inflating survival benefit estimates. The KEYNOTE-564 study,1-2 reporting improved overall survival with use of adjuvant checkpoint inhibitor, pembrolizumab, following surgery for renal cell carcinoma (RCC) suffers from a common challenge: a large portion of the control arm received non-standard of care subsequent therapy upon progression (in this case, dual checkpoint inhibitor or checkpoint inhibitor + tyrosine kinase inhibitor), thus underestimating survival in this group.
Gated Counterfactual Simulation estimates survival under counterfactual standard of care conditions by applying reference trial data. As such, Dr. Ghali and colleagues sought to model the survival of KEYNOTE-564 control group patients had they received checkpoint inhibitor/tyrosine kinase inhibitor therapy per current standard of care to more accurately assess this intervention.
Data were extracted from the Kaplan-Meier plots as published in KEYNOTE-4263 and KEYNOTE-564. Patient-level survival data were simulated using an iterative process to adjust the censored and event rates to ensure consistency with published reference survival curves derived from KEYNOTE-426. Thus, these measures estimate a counterfactual survival parameter for the KEYNOTE-564 control group based on results from the KEYNOTE-426 study to approximate the expected increase in survival probability if the percent of control patients which received non-standard of care therapy had received standard of care:
A total of 52% (n = 109) of patients in the control arm of KEYNOTE-564 that progressed did not receive checkpoint inhibitor in the first-line setting. Based on KEYNOTE-426, the investigators estimated a one-year mortality risk of 9.5% for those receiving axitinib-pembrolizumab versus 19.8% for those receiving tyrosine kinase inhibitor alone, equating to a 10.3% attributable risk between these arms. When analysis was performed on extracted data where that proportion of patients in the control arm were simulated to have avoided death on an annual basis distributed randomly across five years, the results from the re-simulation of KEYNOTE-564 outcomes with a standard of care control demonstrate a simulated overall survival HR of 0.80 (95% CI 0.56 – 1.14) for adjuvant pembrolizumab: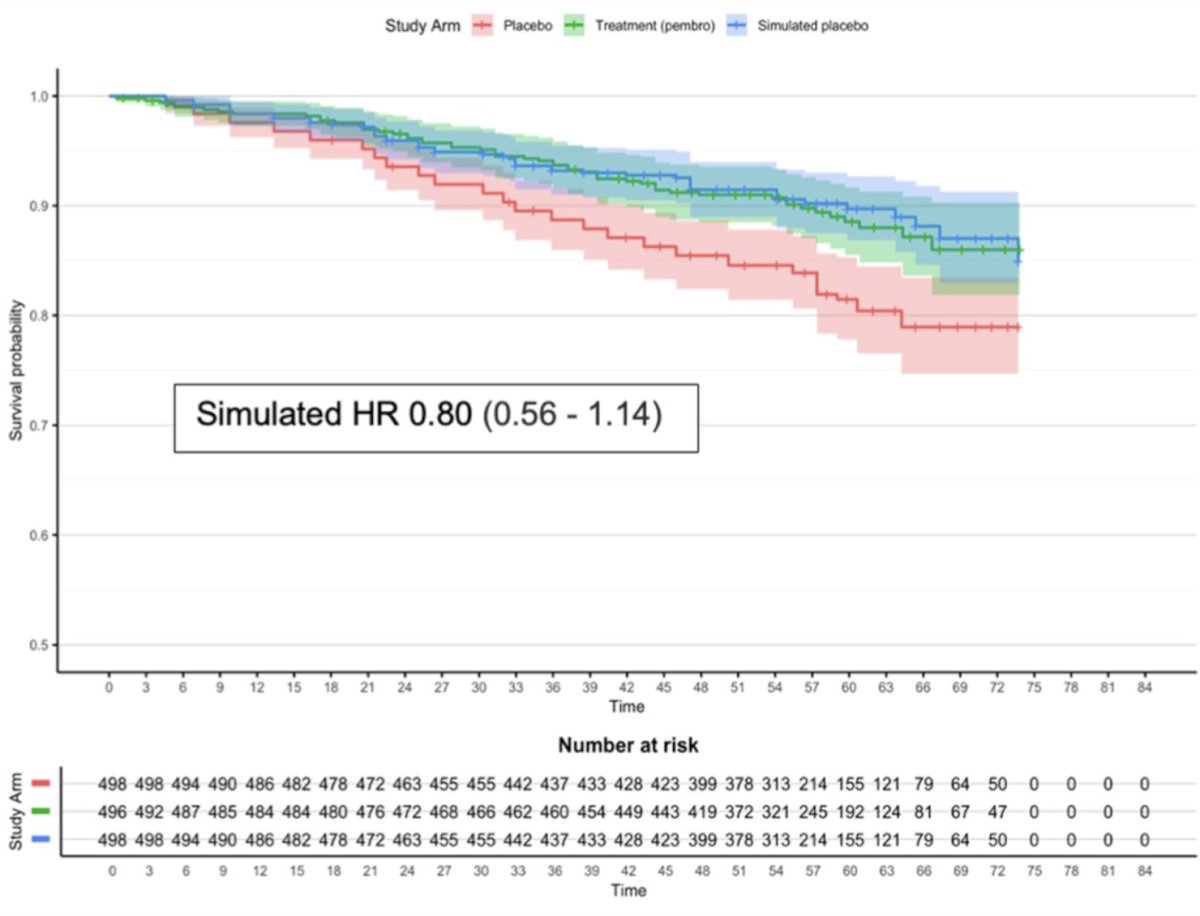
As a sensitivity analysis, the investigators also conducted this model demonstrating hazard ratios for a standard of care control arm simulation with varying effect sizes: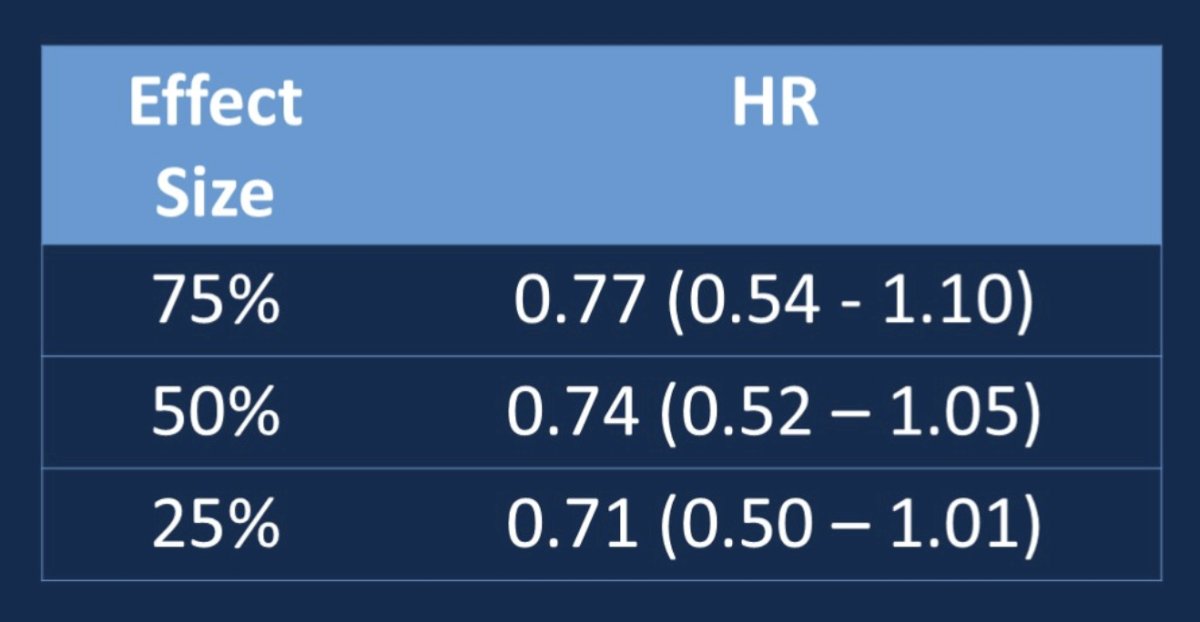
Dr. Ghali concluded his presentation discussing a simulation study of modeling survival outcomes of KEYNOTE-564 with standard of care control arm treatment with the following statements:
- Gated Counterfactual Simulation adjusted survival suggests pembrolizumab’s survival benefit in the adjuvant setting may be overestimated
- A non standard of care control arm can bias regulatory decisions on drug approvals
- Gated Counterfactual Simulation provides a scalable tool for survival re-analysis in clinical trials
- Future applications may improve trial design and regulatory evaluation
Presented by: Fady Ghali, MD, Yale School of Medicine, New Haven, CT
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
References:
- Choueiri TK, Tomczak P, Park SH, et al. Adjuvant Pembrolizumab after Nephrectomy in Renal-Cell Carcinoma. N Engl J Med. 2021 Aug 19;385(8):683-694.
- Choueiri TK, Tomczak P, Park SH, et al. Overall Survival with Adjuvant Pembrolizumab in Renal-Cell Carcinoma. N Engl J Med. 2024 Apr 18;390(15):1359-1371.
- Rini BI, Plimack ER, Stus V, et al. Pembrolizumab plus Axitinib versus Sunitinib for Advanced Renal-Cell Carcinoma. N Engl J Med 2019;380(12):1116-1127.