(UroToday.com) The 2025 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA was host to the Panning for Gold: The Role of ctDNA as a Biomarker for Bladder Cancer Session. Dr. Nimira Alimohamed discussed the Potential Impact of ctDNA on Perioperative Management of Muscle-Invasive Bladder Cancer.
Dr. Alimohamed began by discussing the standard of care for eligible patients with muscle invasive bladder cancer (MIBC), which includes cisplatin-based neoadjuvant chemotherapy followed by radical cystectomy, with adjuvant nivolumab offered to high-risk patients. She highlighted that perioperative chemo-immunotherapy with durvalumab has demonstrated improvements in DFS and OS in the NIAGARA trial, though regulatory approvals are still pending.1 Bladder preservation strategies are being increasingly utilized. The detection of ctDNA after curative-intent treatment signifies molecular residual disease (MRD) and may predict recurrence before imaging. Various ultra-sensitive ctDNA assays, including tumor-agnostic and tumor-informed approaches, have been evaluated to date.
There are many unmet needs in MIBC such as:
Breakthrough therapies and new combinations are expected to improve survival and we eagerly anticipate these data. We should recognize the potential of ctDNA to address some of these unmet needs.
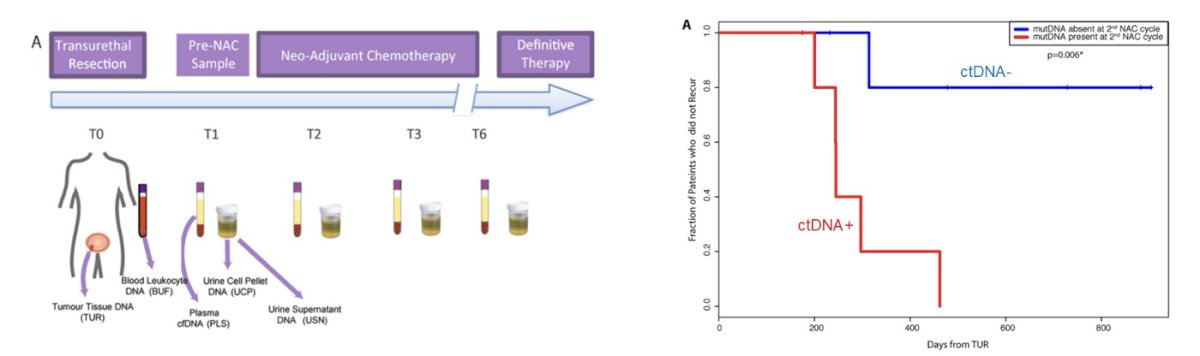
ctDNa in patients treated with neoadjuvant chemotherapy (NAC)ctDNA is prognostic in MIBC treated with NAC. In a study of patients undergoing TURBT followed by NAC, pre-NAC plasma and urine cell pellet samples were collected for cfDNA and UCP analysis (T1), with serial collections (T2-T4) during and after treatment. Among 17 patients receiving cisplatin-based NAC, ctDNA was evaluated using a patient-specific panel of eight genes. Detection of ctDNA before cycle 2 of NAC was significantly associated with early disease recurrence (p = 0.0006), demonstrating a sensitivity of 83% and a specificity of 100%.2
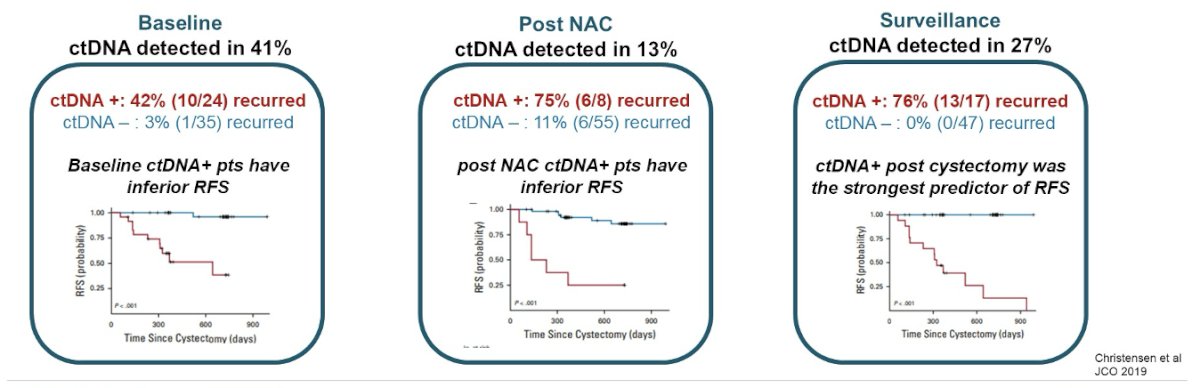
Notably, ctDNA is prognostic at different time points. In a prospective study of 68 patients with MIBC treated with NAC, ctDNA was evaluated at baseline, post-NAC, and during surveillance using a personalized, tumor-informed ctDNA assay (Signatera™). At baseline, ctDNA was detected in 41% of patients. Among those who were ctDNA-positive, 42% experienced recurrence. Post-NAC, ctDNA remained detectable in 13 patients, with 75% of them recurring. During surveillance, ctDNA was detected in 27% of patients, with 76% of these cases associated with recurrence.3
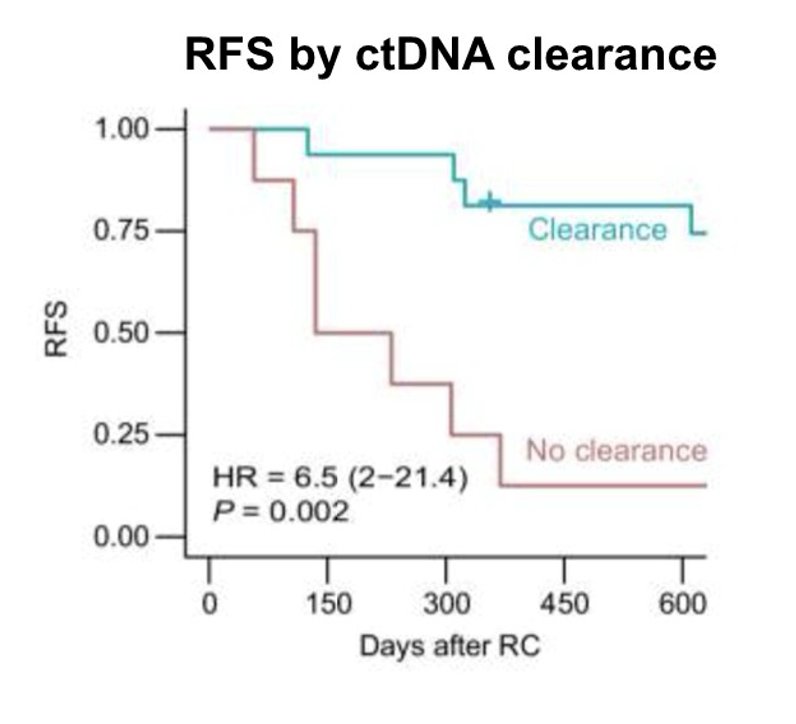
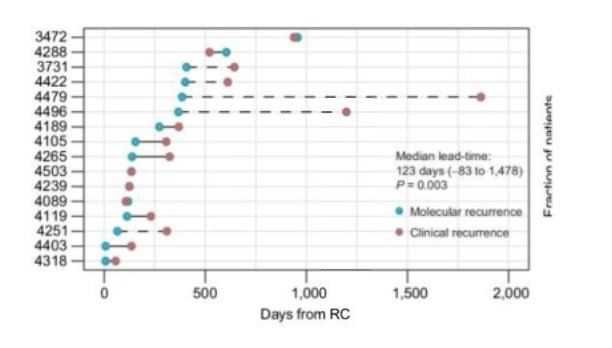
Moreover, ctDNA may serve as an early marker of disease response, with ctDNA dynamics correlating with patient outcomes. An updated analysis of this dataset with a median follow-up of 68 months demonstrated that ctDNA dynamics were associated with clinical outcome (RFS), and ctDNA clearance with NAC correlated with pathologic downstaging.
Notably, in this study, ctDNa detection precedes radiographic disease by 4 months, the median lead time from cDNA detection to radiographic evidence of disease was 123 days.
A retrospective analysis of 167 patients with MIBC assessed ctDNA at three time points—pre-radical cystectomy (RC), post-RC (MRD window), and during surveillance. This multi-institutional study included patients who received diverse treatments and utilized a personalized, tumor-informed ctDNA assay (Signatera™).4
Notably, ctDNA detection at all time points was significantly associated with shorter DFS:
- Pre-RC (p=0.045)
- MRD window (p=0.002)
- Surveillance (p<0.001)
The study schema is illustrated in the figure below.

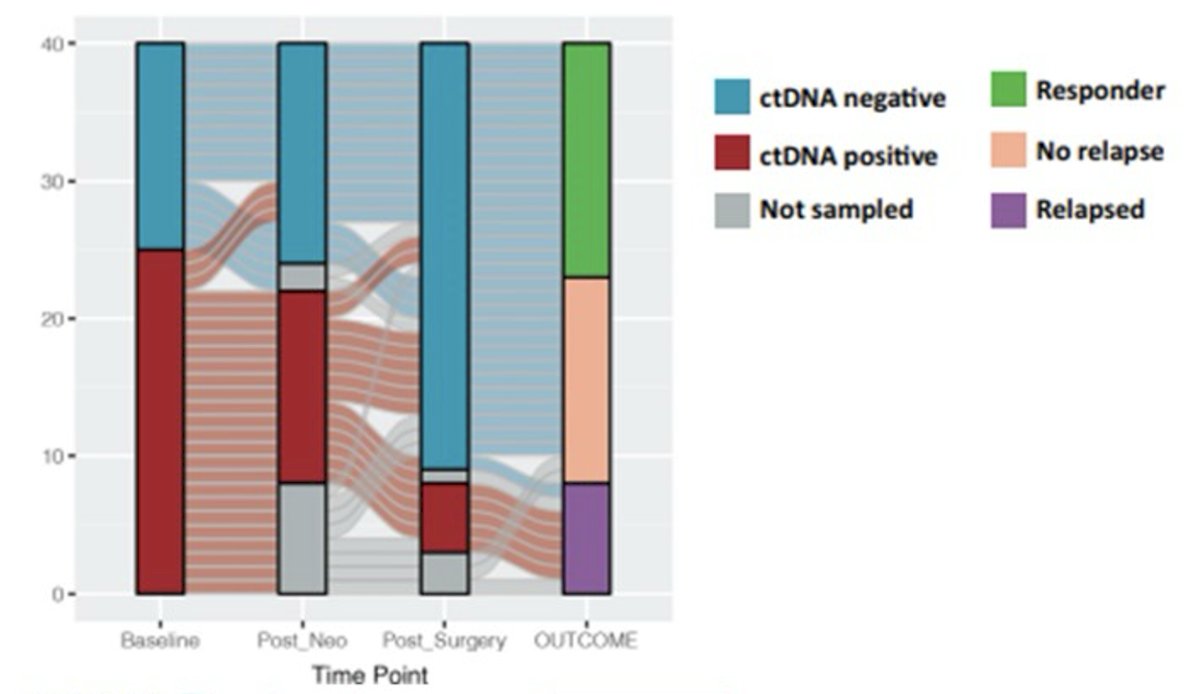
The ABACUS trial evaluated neoadjuvant atezolizumab in MIBC, enrolling cisplatin-ineligible or refusing patients (n=95) who received two cycles of atezolizumab followed by radical cystectomy. The trial met its primary endpoint, demonstrating a pCR rate of 39% and a 2-year DFS of 68%.
Notably, an exploratory analysis (n=40) assessed sequential ctDNA dynamics, revealing that ctDNA positivity was highly prognostic at all time points. Three patients who achieved ctDNA clearance with atezolizumab also achieved pCR, and no relapses were observed in ctDNA-negative patients. The figure below illustrates the decrease in ctDNA positivity following neoadjuvant treatment and surgery, with red bars indicating patients with detectable ctDNA at different time points.5
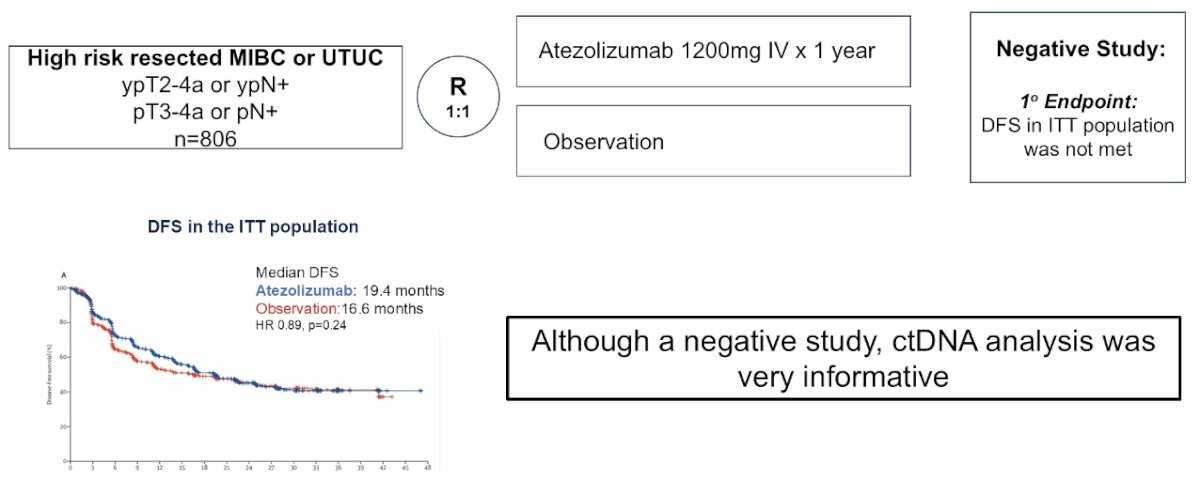
Similarly, the IMvigor010 trial, which evaluated adjuvant atezolizumab in MIBC, did not demonstrate a DFS benefit in the ITT population (19 months with atezolizumab vs. 16 months with observation). However, the ctDNA analysis provided valuable insights into treatment response and prognostic stratification.6
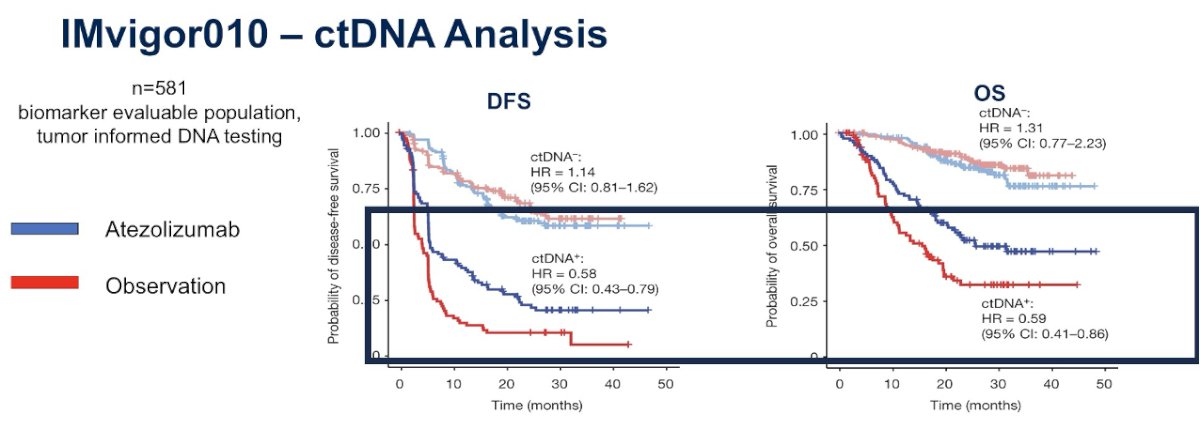
In IMvigor010, ctDNA analysis revealed that ctDNA was detected in 37% of patients after surgery, and these patients had significantly inferior DFS and OS. Notably, among ctDNA+ patients, adjuvant atezolizumab provided a clear benefit in both DFS and OS, highlighting the potential of ctDNA as a biomarker for selecting patients who may derive the most benefit from adjuvant immunotherapy.
In an exploratory analysis of ctDNA dynamics from IMvigor010, the biomarker-evaluable population (n=581) with plasma samples collected at C1D1 and C3D1 demonstrated that ctDNA clearance with atezolizumab was associated with improved overall survival. With a median follow-up of 46.8 months, these findings further emphasize that a decrease in ctDNA levels with immunotherapy may serve as an early marker of treatment effect, reinforcing the role of ctDNA monitoring in guiding therapy decisions.7
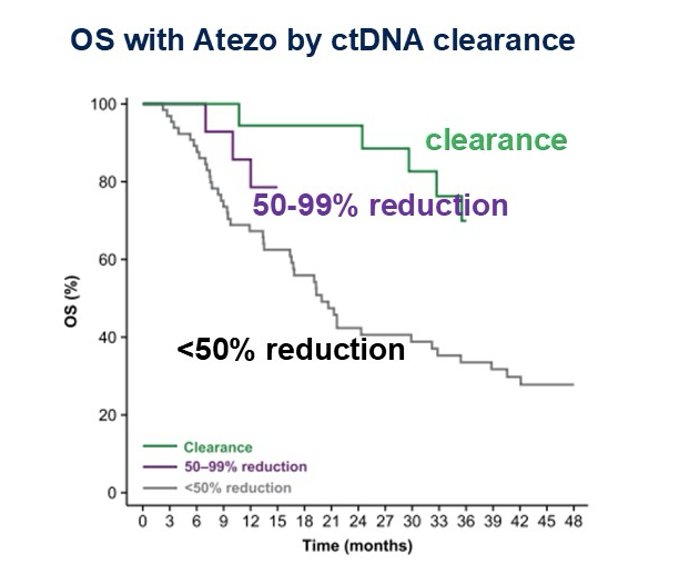
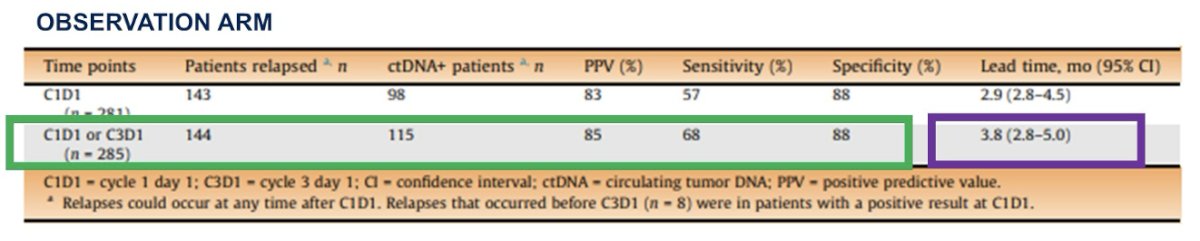
When comparing landmark versus serial ctDNA testing, evaluating ctDNA at both C1D1 and C3D1 increased sensitivity for predicting relapse compared to C1D1 alone. ctDNA detection at either time point provided a lead time of 3.8 months before clinical recurrence. However, despite the improved prognostication with serial ctDNA evaluation after surgery, ctDNA is not a perfect predictor—32% of patients in the ctDNA-negative group still experienced relapse, highlighting the need for further refinement in its clinical application.
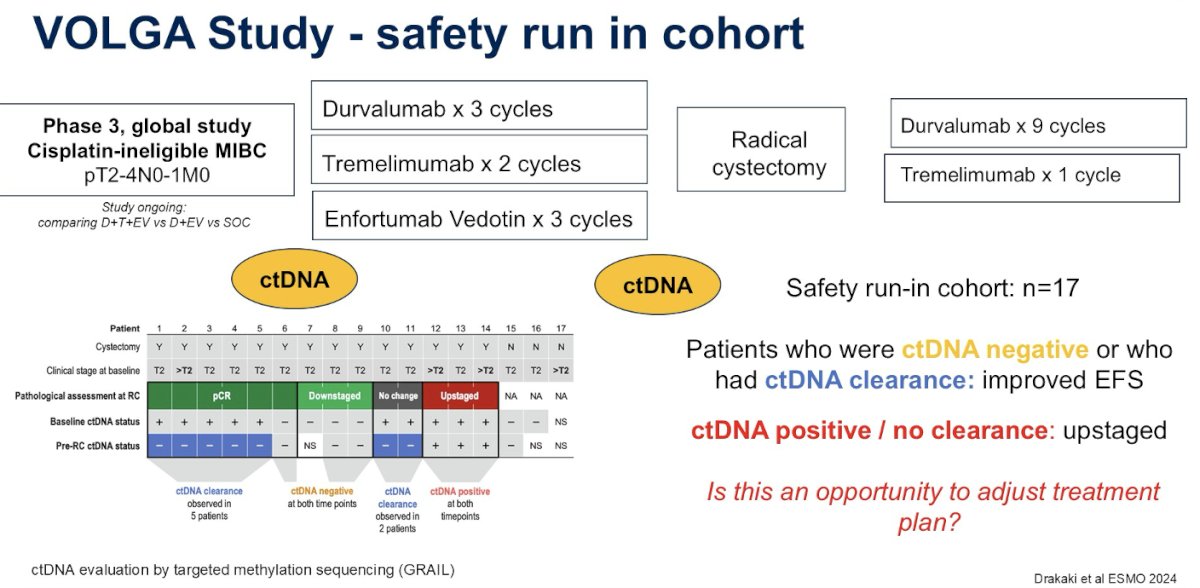
The VOLGA study, a global Phase 3 trial, is evaluating a novel approach for cisplatin-ineligible MIBC (pT2-4N0-1M0) patients with preoperative durvalumab + tremelimumab + enfortumab vedotin, followed by radical cystectomy and adjuvant durvalumab + tremelimumab. ctDNA was assessed both before and after neoadjuvant treatment (prior to radical cystectomy).
In the safety run-in cohort, patients who were ctDNA-negative or achieved ctDNA clearance had improved EFS, whereas those who remained ctDNA-positive or did not clear ctDNA were more likely to be upstaged at surgery. Dr. Alimohamed raised the critical question of whether this data could allow for treatment modifications—potentially identifying patients unlikely to respond to current regimens and adjusting their management accordingly.8
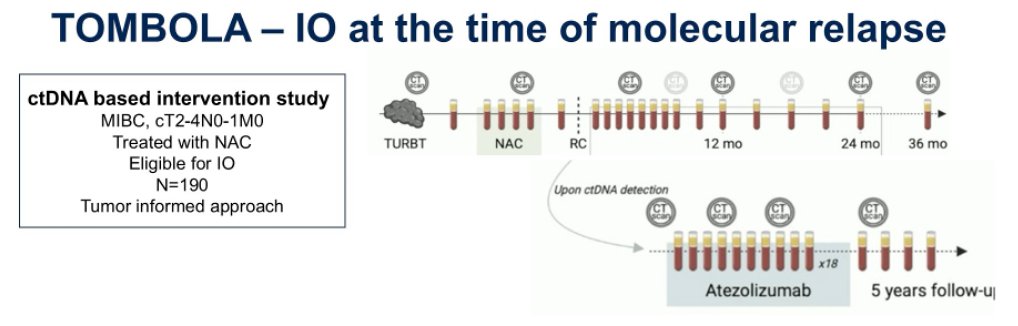
The TOMBOLA study is a ctDNA-based intervention trial evaluating the use of immunotherapy at the time of molecular relapse. It is enrolling patients with MIBC (cT2-4N0-1M0) who have been treated with neoadjuvant chemotherapy (NAC) and are eligible for adjuvant immunotherapy (IO). The study aims to determine whether initiating immunotherapy at the time of molecular relapse improves outcomes, with a primary endpoint of complete response (ctDNA/imaging) after treatment.
A preliminary analysis revealed that among ctDNA- patients, only 2 out of 66 relapsed. Notably, 56% of patients were ctDNA+ post-cystectomy and were subsequently treated with atezolizumab, leading to 55% converting to ctDNA- status with no evidence of disease on imaging.
The IMvigor011 trial is a randomized study that stratifies patients based on ctDNA status, administering adjuvant atezolizumab specifically to ctDNA-positive patients. This trial aims to determine whether serial ctDNA testing can more effectively identify patients who will benefit from adjuvant immunotherapy while sparing ctDNA-negative patients from unnecessary treatment and toxicity. The study design is shown below.
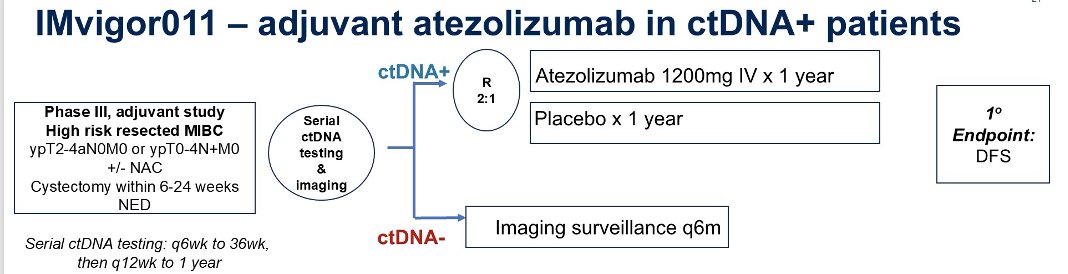
An exploratory analysis of the IMvigor011 trial focused on the surveillance cohort, where patients with high-risk MIBC who remained persistently ctDNA-negative (n=171, median follow-up 16.3 months) demonstrated favorable outcomes. At 12 and 18 months, DFS rates were 92% and 88%, respectively, while OS was 100% and 98%. These findings support the growing confidence in a surveillance approach for patients with persistently undetectable ctDNA, potentially avoiding unnecessary adjuvant therapy.
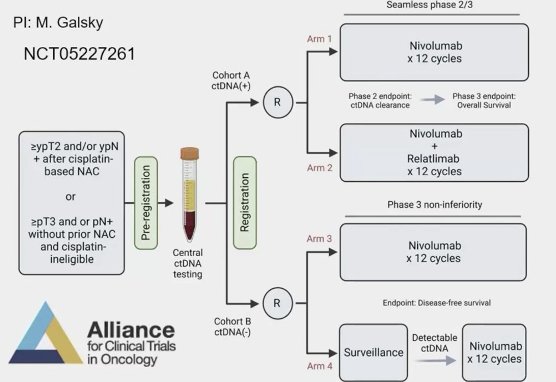
The MODERN study, led by Dr. Galsky, is a ctDNA-guided trial designed to evaluate treatment escalation and de-escalation strategies in MIBC. The study aims to determine whether patients with detectable ctDNA benefit from intensified therapy and whether those with undetectable ctDNA can safely forgo immediate treatment until MRD is detected.
Refinements in patient selection and advancements in systemic therapy may enhance outcomes for patients pursuing bladder preservation. However, the definition of a complete clinical response (cCR) to identify those who can safely avoid radical cystectomy remains unstandardized. Various trials, such as Alliance (incorporating DDR gene alterations, imaging, and TURBT), HCRN GU 16-257 (using cytology, imaging, and TURBT), and RETAIN (focusing on gene alterations, imaging, and TURBT), have attempted to define response criteria. Despite these efforts, a significant number of patients on active surveillance have experienced recurrence. The integration of ctDNA into response assessments could refine patient selection, improve outcomes, and expand bladder preservation strategies.
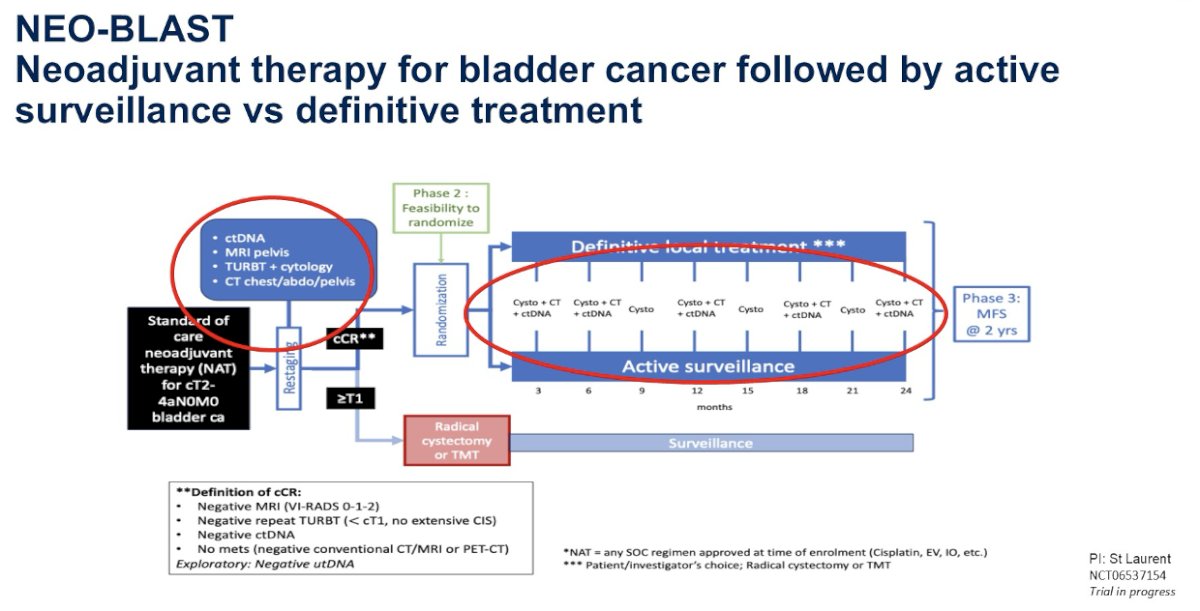
The NEO-BLAST trial is investigating neoadjuvant therapy for MIBC, incorporating ctDNA as part of the criteria to assess clinical complete response (cCR). Patients who achieve a complete response may proceed with local definitive treatment or surveillance instead of radical cystectomy.
Dr. Alimohamed discussed the current challenges of incorporating ctDNA into clinical decision-making, highlighting that ctDNA evaluation remains costly and is often inaccessible outside major academic centers. Additionally, prospective validation is still pending, making it difficult to establish standardized clinical applications. The rapid evolution of ctDNA technology, systemic therapies, and treatment paradigms further complicates data interpretation, underscoring the need for ongoing research and validation.
In the current clinical context, ctDNA is only informative but does not yet alter standard practice. For now, NAC remains recommended regardless of ctDNA status, and in the neoadjuvant setting, detection of ctDNA after 2 or 4 cycles does not necessarily prompt treatment changes beyond updated imaging. Similarly, in the adjuvant setting, if ctDNA is undetectable after radical cystectomy, adjuvant nivolumab is still offered to patients meeting high-risk criteria.
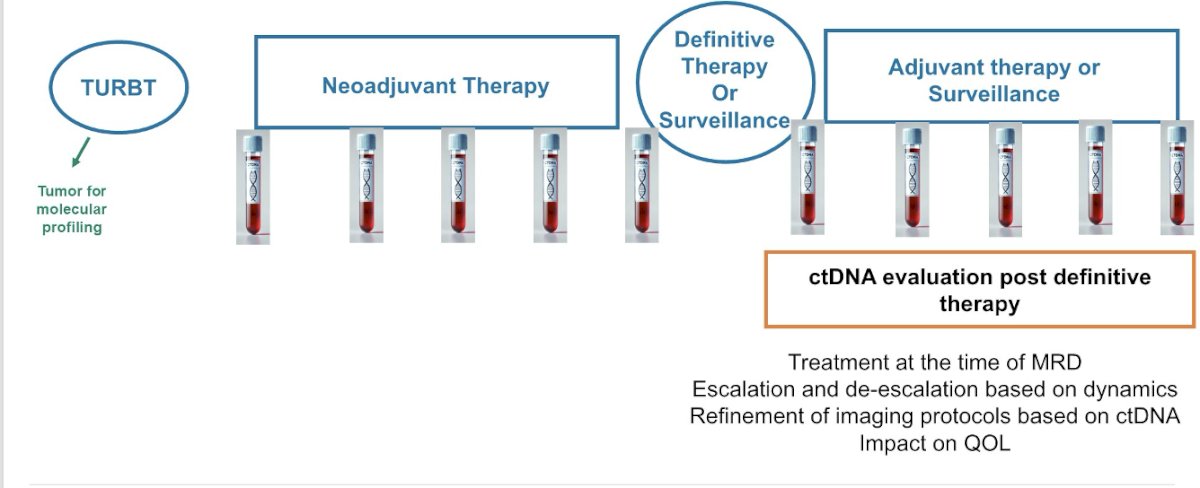
In the future clinical context, ctDNA is expected to play a more active role in clinical decision-making. At baseline, it could help guide treatment selection. During neoadjuvant therapy, ctDNA detection and dynamics may allow for treatment adjustments—escalating therapy for non-responders and potentially de-escalating for responders. In the pre-definitive therapy setting, ctDNA could become part of the assessment for clinical complete response, influencing the choice between definitive therapy and surveillance, with potential implications for quality of life. Post-definitive therapy, ctDNA monitoring could guide MRD-driven treatment strategies, support escalation or de-escalation decisions, refine imaging protocols, and further impact patient outcomes and quality of life.
Dr. Alimohamed concluded her presentation with three key messages:
- ctDNA is a prognostic biomarker in MIBC.
- ctDNA detection and dynamics are important in this disease—currently informative but with many potential clinical applications in the future clinical context.
- ctDNA-guided treatment may improve survival and quality of life in patients with MIBC.
Presented by: Nimira S. Alimohamed, MD, FRCPC, Medical Oncologist at the Tom Baker Cancer Centre, Clinical Assistant Professor in the Department of Medicine at the University of Calgary, Calgary, AB, Canada.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
References:- Rubin EJ, Yeku OO, Morrissey S. NEJM at ESMO - Perioperative Durvalumab with Neoadjuvant Chemotherapy in Operable Bladder Cancer. N Engl J Med. 2024 Nov 14;391(19):e44. doi: 10.1056/NEJMe2411490. Epub 2024 Sep 15. PMID: 39282940.
- Patel KM, van der Vos KE, Smith CG, Mouliere F, Tsui D, Morris J, Chandrananda D, Marass F, van den Broek D, Neal DE, Gnanapragasam VJ, Forshew T, van Rhijn BW, Massie CE, Rosenfeld N, van der Heijden MS. Association Of Plasma And Urinary Mutant DNA With Clinical Outcomes In Muscle Invasive Bladder Cancer. Sci Rep. 2017 Jul 17;7(1):5554. doi: 10.1038/s41598-017-05623-3. PMID: 28717136; PMCID: PMC5514073.
- Christensen E, Birkenkamp-Demtröder K, Sethi H, Shchegrova S, Salari R, Nordentoft I, Wu HT, Knudsen M, Lamy P, Lindskrog SV, Taber A, Balcioglu M, Vang S, Assaf Z, Sharma S, Tin AS, Srinivasan R, Hafez D, Reinert T, Navarro S, Olson A, Ram R, Dashner S, Rabinowitz M, Billings P, Sigurjonsson S, Andersen CL, Swenerton R, Aleshin A, Zimmermann B, Agerbæk M, Lin CJ, Jensen JB, Dyrskjøt L. Early Detection of Metastatic Relapse and Monitoring of Therapeutic Efficacy by Ultra-Deep Sequencing of Plasma Cell-Free DNA in Patients With Urothelial Bladder Carcinoma. J Clin Oncol. 2019 Jun 20;37(18):1547-1557. doi: 10.1200/JCO.18.02052. Epub 2019 May 6. PMID: 31059311.
- Sfakianos JP, Basu A, Laliotis G, Cumarasamy S, Rich JM, Kommalapati A, Glover M, Mahmood T, Tillu N, Hoimes CJ, Selig G, Kollipara R, Stewart TF, Rivero-Hinojosa S, Dutta P, Calhoun M, Sharma S, Malhotra M, ElNaggar AC, Liu MC, Ferguson JE 3rd, Diniz M, Mehrazin R, Wiklund P, Tan A, Shah S, Galsky MD. Association of Tumor-informed Circulating Tumor DNA Detectability Before and After Radical Cystectomy with Disease-free Survival in Patients with Bladder Cancer. Eur Urol Oncol. 2024 Jul 15:S2588-9311(24)00174-3. doi: 10.1016/j.euo.2024.07.001. Epub ahead of print. PMID: 39013741.
- Szabados B, Kockx M, Assaf ZJ, van Dam PJ, Rodriguez-Vida A, Duran I, Crabb SJ, Van Der Heijden MS, Pous AF, Gravis G, Herranz UA, Protheroe A, Ravaud A, Maillet D, Mendez MJ, Suarez C, Linch M, Prendergast A, Tyson C, Stanoeva D, Daelemans S, Rombouts M, Mariathasan S, Tea JS, Mousa K, Sharma S, Aleshin A, Banchereau R, Castellano D, Powles T. Final Results of Neoadjuvant Atezolizumab in Cisplatin-ineligible Patients with Muscle-invasive Urothelial Cancer of the Bladder. Eur Urol. 2022 Aug;82(2):212-222. doi: 10.1016/j.eururo.2022.04.013. Epub 2022 May 14. PMID: 35577646.
- Bellmunt J, Hussain M, Gschwend JE, Albers P, Oudard S, Castellano D, Daneshmand S, Nishiyama H, Majchrowicz M, Degaonkar V, Shi Y, Mariathasan S, Grivas P, Drakaki A, O'Donnell PH, Rosenberg JE, Geynisman DM, Petrylak DP, Hoffman-Censits J, Bedke J, Kalebasty AR, Zakharia Y, van der Heijden MS, Sternberg CN, Davarpanah NN, Powles T; IMvigor010 Study Group. Adjuvant atezolizumab versus observation in muscle-invasive urothelial carcinoma (IMvigor010): a multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2021 Apr;22(4):525-537. doi: 10.1016/S1470-2045(21)00004-8. Epub 2021 Mar 12. PMID: 33721560; PMCID: PMC8495594.
- Powles T, Assaf ZJ, Degaonkar V, Grivas P, Hussain M, Oudard S, Gschwend JE, Albers P, Castellano D, Nishiyama H, Daneshmand S, Sharma S, Sethi H, Aleshin A, Shi Y, Davarpanah N, Carter C, Bellmunt J, Mariathasan S. Updated Overall Survival by Circulating Tumor DNA Status from the Phase 3 IMvigor010 Trial: Adjuvant Atezolizumab Versus Observation in Muscle-invasive Urothelial Carcinoma. Eur Urol. 2024 Feb;85(2):114-122. doi: 10.1016/j.eururo.2023.06.007. Epub 2023 Jul 26. PMID: 37500339.
- Drakaki A, et al,. 1970MO - Circulating tumor DNA (ctDNA) clearance with neoadjuvant durvalumab (D) + tremelimumab (T) + enfortumab vedotin (EV) for cisplatin-ineligible muscle-invasive bladder cancer (MIBC) from the safety run-in cohort of the phase III VOLGA trial. Annals of Oncology (2024) 35 (suppl_2): S1135-S1169. 10.1016/annonc/annonc1616